
Abstract
Abstract
Purpose
The study was undertaken to: (1) describe the characteristic radiological features and problems of management of the loss of one condyle of the femur or tibia following septic arthritis of the knee in infancy and (2) test a hypothesis of the cause of the loss of a single condyle.
Methods
Radiographs of eight children with the loss of one condyle of the femur or the tibia following septic arthritis in infancy were reviewed. The course and outcome in two of these children who underwent reconstructive operations were studied. The knees of 35 stillborn foetuses were dissected to determine if the presence of synovial septae could account for the isolated loss of one condyle following infection.
Results
All eight cases showed characteristic features of loss of half the epiphysis, the underlying physis and part of the adjacent metaphysis; the other condyle was totally spared. The two children who underwent elaborate reconstructive procedures had poor outcomes at skeletal maturity, despite a series of additional operations. The foetal cadaveric study showed that complete infrapatellar synovial septae are present in some foetuses approaching 40 weeks of gestation.
Conclusions
The pattern of loss of a femoral or tibial condyle following septic arthritis is consistent with total preservation of the other condyle. The outcome of surgical reconstruction of the missing condyle is poor. The presence of a complete synovial septum could result in the localisation of infection to one half of the joint, with the destruction of one condyle.
Introduction
Loss of one condyle of the femur or tibia following septic arthritis of the knee in early infancy can have devastating long-term effects, warranting repeated operations throughout childhood and permanent disability, despite such intervention. Hence, it would be profoundly useful if the pathogenesis of this complication is understood so that measures could be taken to prevent it. While the loss of one condyle due to joint sepsis has been well documented in the literature, little is known about its pathogenesis [1–6].
Anatomists and embryologists suggest that the knee develops by the cavitation of mesenchymal condensation between the femur, patella and tibia, which later coalesce to form the patello-femoral and femoro-tibial joint cavities. They estimate that, by the tenth week of intra-uterine development, the knee joint consists of a single cavity [7]. However, several studies have also demonstrated the presence of synovial folds or plicae in foetuses, children and adults that are considered to be remnants of septae separating the compartments of the developing joint [8–18].
We hypothesised that one possible explanation for the selective destruction of one condyle without any damage to the other condyle may be due, in part, to the persistence of a complete vertical septum dividing the knee joint into medial and lateral femoro-tibial compartments. We undertook this study to test this hypothesis and determine whether a complete vertical septum dividing the joint is a foetal developmental variation that may persist into early infancy.
We also reviewed the records of children with loss of a condyle of the femur or the tibia following neonatal septic arthritis to determine the pattern of damage to the joint and to evaluate the results of reconstruction of the missing condyle.
Materials and methods
The study was undertaken after Institutional Ethical Committee approval.
Clinical study
The archived radiographs of the Paediatric Orthopaedic Service collected over 20 years were reviewed to identify patients who had presented at this hospital with loss of either the medial or lateral condyle of the tibia or femur in infancy; radiographs of eight such cases were available for study. The patterns and extent of destruction of the epiphysis, growth plate and the metaphysis were documented. As the initial treatment in the neonatal period in all but one case was provided at other hospitals, details of the exact timing and nature of treatment were not available in all cases. One neonate had been treated with an arthroscopic lavage through a superolateral portal, one neonate had been treated by arthrocentesis and the others were treated by some form of open drainage.
Only one child with the loss of a femoral condyle and one child with the loss of a condyle of the tibia underwent procedures in early childhood to reconstruct the missing condyle, and they were followed up to skeletal maturity. Their sequential radiographs were studied and details of the initial surgical reconstruction and subsequent operations were noted from the records. The status of the knee of these children with reference to residual deformity, joint motion and joint stability that was recorded at skeletal maturity was noted.
Cadaveric study
After obtaining informed consent from the parents, the knee joints of 35 stillborn foetuses with a gestational age of over 20 weeks were dissected. Through a transverse incision at the proximal pole of the patella, the quadriceps tendon was divided just above the patella and the patellar retinaculae were divided transversely at the same level. The patella was reflected distally and the joint was inspected to identify infrapatellar synovial plicae in particular. If an infrapatellar plica was present, it was classified into one of the patterns described by Kim et al. [14] (cord, split septum, fenestrated septum or complete vertical septum).
Results
Radiological pattern of joint destruction
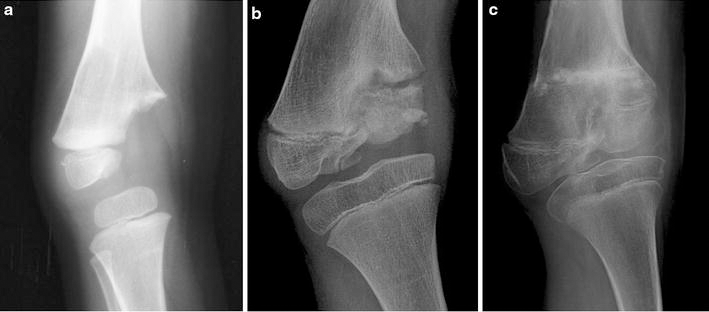
The pattern of bone destruction noted on the initial radiographs was consistent; the entire half of the epiphysis of the femur or tibia along with the growth plate and the adjacent part of the metaphysis were missing in all the patients. The destruction did not cross the midline of the joint and stopped short at the region of the tibial spine when the tibia was affected or the intercondylar region of the femur when the femur was affected. The intact condyle was normal in configuration in every instance (Figs. 1, 2a). Among the six children with loss of the femoral condyle, the medial condyle was destroyed in two cases and the lateral femoral condyle was destroyed in four cases. In both the children with tibial condylar loss, the medial condyle was destroyed. The child who had been treated by an arthroscopic lavage through a superolateral portal had a loss of the medial femoral condyle.

Radiograph of the knee of an infant showing destruction of the lateral femoral condyle. The medial femoral condyle is well preserved

Genu varum secondary to the loss of the medial tibial condyle in a child (
Clinical course of patients who underwent attempts at reconstruction of the missing condyle
Case 1
A male baby who developed neonatal septicaemia with multifocal septic arthritis involving the right shoulder, right elbow and left knee was initially treated by arthrocentesis of all the affected joints and the administration of parenteral antibiotics. Significant damage to the left knee and right shoulder ensued. At the knee, the medial half of the proximal tibial epiphysis and the growth plate were destroyed. Progressive genu varum developed, for which a corrective osteotomy was performed at 2 years of age. A knee–ankle–foot orthosis (KAFO) was used once the osteotomy united. Despite this treatment, the deformity progressively increased until a varus deviation of 30° associated with medial ligament laxity was noted at 4 years of age (Fig. 2a). At this point, an attempt was made to reconstruct the medial tibial condyle with the ipsilateral patella. The patellar graft was mobilised on a pedicle of a third of the patellar tendon and rotated so that its articular surface was aligned to the femoral condyle. Care was taken to ensure that the continuity of quadriceps and two-thirds of the patellar tendon was maintained. The borders of the patella and medial border of the lateral tibial condyle were freshened to ensure contact of raw cancellous surfaces and fixed with horizontal Kirschner wires (K-wires). A fat graft was interposed between the patella and the elevated tibial metaphysis to prevent union of the graft to the metaphysis (Figs. 2b, 3). Within 2 years, the genu varum recurred and 3 cm of shortening of the tibia was noted. The grafted patella had failed to unite to the lateral tibial condyle and had displaced distally with depression of its articular surface (Fig. 2c). The patella was re-fixed to the lateral tibial condyle with K-wires and a fibular strut graft was inserted under the patella to support it and keep it elevated. The varus deformity recurred and, at 8 years, epiphyseodesis of the lateral tibial growth plate was performed with three staples. The progression of the deformity was controlled but the knee remained distorted and unstable (Fig. 2d). At 20 years, the boy still needs a KAFO for support while walking.
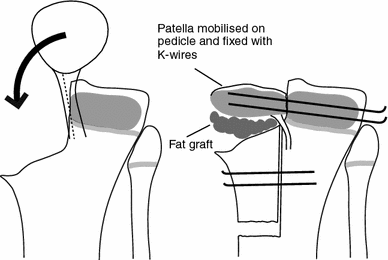
The diagram shows the details of the reconstruction of the missing medial tibial condyle
Case 2
A baby girl developed septic arthritis of the right knee in early infancy. Though an arthrotomy and drainage was done, the medial half of the femoral condyle was destroyed, resulting in progressive genu varum and a flexion deformity (Fig. 4a). At 18 months of age, an antero-lateral closed wedge, supracondylar valgus osteotomy was performed. A KAFO was worn after union of the osteotomy. A year later, the deformity recurred and early collateral ligament laxity and knee instability was noted. A reconstructive procedure of the right medial condyle was performed. The proximal third of the fibula was mobilised without detaching the insertion of the biceps femoris in order to retain the physeal and epiphyseal blood supply. The fibula was rotated by 180° so that the fibular head was in contact with the tibial condyle and the distal end of the fibular segment was fixed into the medullary cavity of the femur (Fig. 5). Weight-bearing was permitted with a KAFO after union of the fibular graft to the femur. Recurrence of the varus deformity was noted at 4 years of age, for which a supracondylar corrective osteotomy was performed. Over time, the head of the fibula took the shape of the missing condyle but remained small (Fig. 4b). The growth plate of the transplanted fibula appeared viable, but its contribution to longitudinal growth of the femur was not proportionate to the growth of the normal half of the tibial growth plate and, consequently, the varus deformity recurred and yet another corrective osteotomy was needed at 9 years (Fig. 4c). At the age of 11 years, epiphyseodesis of the lateral half of the femoral growth plate was performed. At skeletal maturity, she had instability and complex angular and torsional deformities at the knee, for which a supracondylar osteotomy was performed. At the last follow-up, she has an acceptable alignment of the knee and 100° of pain-free motion but she has a 9-cm shortening of the limb.
Loss of the medial femoral condyle has resulted in genu varum in a young child (
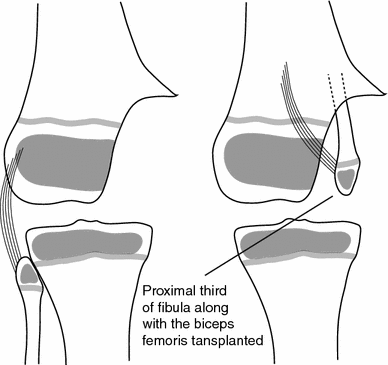
The diagram shows the details of the reconstruction of the missing femoral condyle
Cadaveric dissections
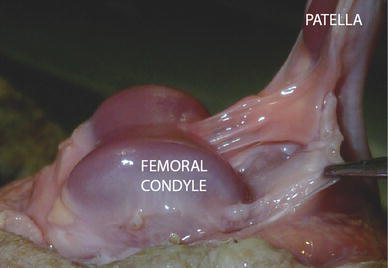
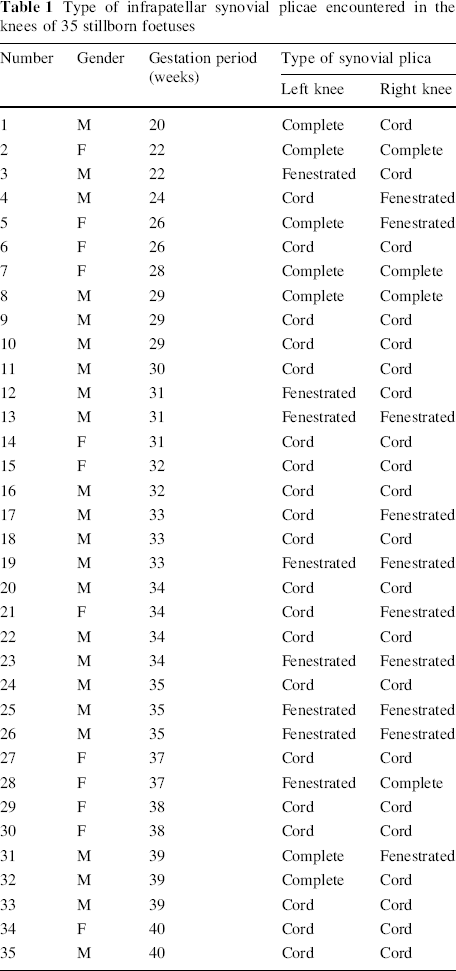
The mean gestational age of the 35 foetuses was 32.3 weeks (range 20–40 weeks). Of 70 foetal knees that were dissected, 11 (15.7 %) had a well-formed complete vertical infrapatellar septum that separated the knee joint cavity into medial and lateral halves (Fig. 6). In 18 knees (25.7 %), the fenestrated type of plica was encountered. Here, the septum was well formed, but there was a foramen that would enable the free flow of fluid across the septum (Fig. 7). In the remaining knees, a small ligamentum mucosum corresponding to the cord type plica of Kim et al. [14] was noted (Table 1). In one knee, there was a suprapatellar septum that divided the suprapatellar bursa into medial and lateral halves.
A complete infrapatellar synovial septum noted in a stillborn foetus A well-formed infrapatellar synovial septum with a fenestration noted in a stillborn foetus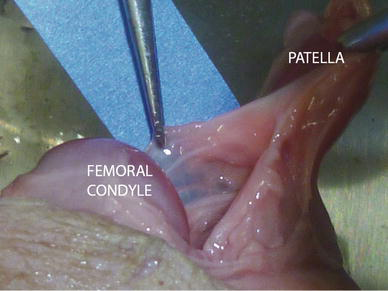
Type of infrapatellar synovial plicae encountered in the knees of 35 stillborn foetuses
Discussion
The protean manifestations of the sequelae of septic arthritis of the knee have been lucidly outlined by Strong et al. [19]. Of the patterns of bone and cartilage tissue destruction noted in their study, destruction of part of the epiphysis was seen in 6 % of affected children. Among children who present with apparent loss of a femoral or tibial condyle, there are some which have cartilaginous remnants of the “missing” condyle that cannot be visualised on the plain radiograph but can be appreciated when an arthrogram is performed [1, 4, 19]. Some degree of regeneration of these condyles can occur over time. However, true loss of the condyle can also occur [3, 5, 19] and treatment of these cases is more challenging. Strong et al. [19] point out that, when true destruction of part of the epiphysis does occur, the joint is unstable and a significant deformity develops rapidly; this has been our experience also. The two illustrative cases in whom reconstruction of the missing condyle was attempted clearly show how difficult it is to treat this complication of septic arthritis of the knee.
It may be argued that these reconstructive procedures were ill-advised. However, if left alone, the outcome at skeletal maturity may be worse than that noted in the two patients on which we operated, as illustrated in an adolescent who had had no treatment (Fig. 8). The other option would have been to perform repeated corrective osteotomies as and when needed to correct recurrent deformities and deal with joint instability by bracing throughout life. Langenskiöld noted that up to six osteotomies may be needed before skeletal maturity in these children [5]. The number of osteotomies needed in the two children who underwent reconstruction was fewer than this. It remains conjectural if reconstructive procedures for the missing condyle described here and reported in the literature [2, 3, 6] offer an advantage over repeated osteotomies and bracing. Either way, the final outcome will never be optimal and this highlights the need to prevent this disastrous complication.

Radiograph (
The patients we report with the loss of one condyle had documented history of septic arthritis but some authors have attributed this pattern of destruction to osteomyelitis affecting a single condyle rather than a primary septic arthritis [3, 5, 6, 19]. Strong et al. suggest that this pattern of destruction may be due to metaphyseal infection spreading to the epiphysis through transphyseal blood vessels. It is certainly possible that the suppuration within the joint could have followed destructive osteomyelitis involving one condyle, but the sparing of the articular cartilage over the adjacent condyle once pus is in the joint cavity still needs to be explained. The characteristic pattern of destruction noted in all the radiographs suggest that the destroyed part of the bone alone was exposed to the destructive influences, while the unaffected part of the bone was, in some way, protected from these factors. The two mechanisms of cartilage and bone destruction in neonatal septic arthritis include proteolytic degradation and vascular occlusion. Either or both these mechanisms may have contributed to the destruction of the condyle in the cases we encountered. We hypothesised that only the affected condyle was exposed to the proteolytic enzymes of the bacteria. Such a situation would account for the fact that the intact condyle appeared normal. This would only be possible if the pus was strictly loculated in either the medial or lateral half of the joint. A complete synovial septum that divided the joint could be one plausible explanation for such a phenomenon (Fig. 9).
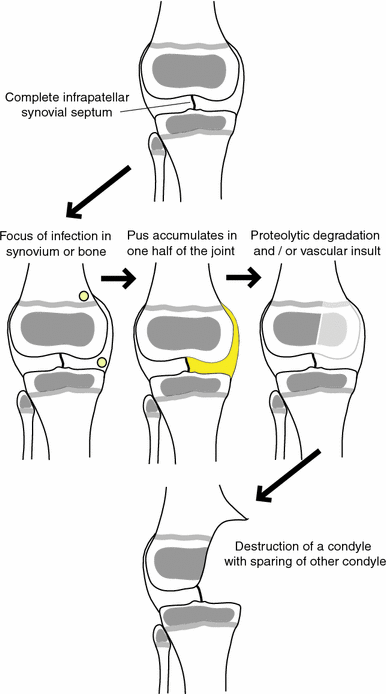
Diagrammatic representation of the hypothesis of the cause of the loss of a femoral or tibial condyle following septic arthritis in the neonate in the presence of a complete infrapatellar synovial septum
The foetal dissection study shows that a well-formed infrapatellar septum that divided the joint cavity into a medial and a lateral half was present in some foetuses, including a few approaching 40 weeks of gestation. An arthroscopic study had reported similar findings [17]. This implies that some of these complete septae could persist into early neonatal life and could then account for the localisation of infection in either the medial or lateral half of the knee. Arthroscopic drainage of an infected knee joint may be difficult in such situations, as the passage of the arthroscope may be hindered by the presence of a complete infrapatellar septum [9, 15]. It is pertinent to note that, in the child who had an arthroscopic lavage through the superolateral portal, the medial femoral condyle was destroyed. It would have been interesting to know if the surgeon noted the presence of a septum or had any problem in decompressing the joint and draining the pus. Synovial plicae have also been shown to be thickened in response to inflammation at arthroscopy [13, 16], and it is also possible that inflammatory adhesions can seal off fenestrations in incomplete septae.
We paid special attention to infrapatellar plicae, as the orientation of this plica is such that it could possibly divide the knee into medial and lateral halves. However, other well-formed plicae dividing the joint have been reported in the literature. Two studies reported suprapatellar plicae in the form of a membrane separating the suprapatellar pouch from the femoro-tibial compartment with a frequency of 16.7 and 15 %, respectively [17, 18]. These observations add to the evidence that synovial septae that divide the cavity of the knee joint may be present in neonates.
Though we cannot confirm if such septae were present in children with the loss of one condyle, we feel that such a possibility needs to be kept in mind while treating infants with septic arthritis of the knee. If pus is localised to either the medial or lateral half of the joint by a complete septum, the diagnosis may be missed if the surgeon introduces the needle into the uninvolved side of the joint while performing a diagnostic aspiration. Similarly if an arthroscopic lavage of the infected joint is undertaken, the possibility of a loculated collection of pus must be borne in mind.
Footnotes
Acknowledgements
The clinical fellowship of Stéphane Tercier was supported by Swiss grants (Fonds du Département Médico-Chirurgical de Pédiatrie et de Perfectionnement du CHUV, Fondation SICPA, Fondation de l'Hôpital Orthopédique de Lausanne et Fonds de la Société Suisse d'Orthopédie et Traumatologie). K.M. Girisha received grants from the Indian Council of Medical Research (Grant No. 54/5/2010-BMS) for foetal autopsy studies.