
Abstract
Purpose
Lateral growth arrest is recognised as the most common form of avascular necrosis (AVN) seen in the management of developmental dysplasia of the hip (DDH). The purpose of this report is to present a new technique that is of benefit in the early identification and subsequent radiological monitoring of lateral growth arrest and which may permit appropriate timely surgical intervention.
Methods
We performed a retrospective review of the medical records and serial radiographs of 11 patients (three males and eight females) with lateral growth disturbance in the proximal femoral physis. We devised a new technique (named the ‘Tilt angle’) for serial radiographic observation of lateral growth arrest.
Results
This study included 11 hips in 11 patients. Ten patients had screw epiphyseodesis performed after progression of lateral growth arrest was noted. One patient did not have screw epiphyseodesis but the results for this patient are included, as they provide an interesting ‘control’ case for comparison. The average age of screw epiphyseodesis was 12 years. Seven patients demonstrated improvement in their tilt angle following screw epiphyseodesis (i.e. less valgus), one showed no change and two continued to decline.
Conclusions
Using a new technique to monitor the progression of lateral growth arrest, we noted that screw epiphyseodesis can be used for guided growth of the proximal femoral physis. This technique can be employed for serial radiographic observation of lateral growth arrest and can guide the clinician on the optimal timing of screw epiphyseodesis. Further studies are needed in order to clarify the optimal timing of screw epiphyseodesis.
Introduction
Avascular necrosis (AVN) is a recognised complication following treatment for developmental dysplasia of the hip (DDH). Lateral growth arrest (type II) is noted to be the most common type [1]. Damage to the lateral aspect of the capital femoral physis typically results in premature lateral epiphyseodesis. This can cause tilting of the femoral head into valgus as a consequence of the tethering effect on the physis. At skeletal maturity, this may result in a short neck with valgus angulation and, if excessive, can lead to marked uncovering of the femoral head in the acetabulum, posing challenges for adult salvage procedures.
Kalamchi and MacEwen [1] also reported that early recognition of lateral growth arrest can be challenging, but one must be alert to the presence of lateral ossification, lateral physeal irregularity and bridging, lateral notching of the epiphysis and a lateral metaphyseal defect in the early radiological detection of this form of AVN. These appearances are often subtle and, indeed, asymmetrical growth in the physis may not become evident until the age of 9 or 10 years.
The purpose of this report is to present a new technique that is of benefit in the early identification and subsequent radiological monitoring of lateral growth arrest and which may permit appropriate timely surgical intervention of screw epiphyseodesis for guided growth.
Materials and methods
We performed a retrospective review of the medical records and serial radiographs of 11 patients (eight females and three males) with lateral growth disturbance in the proximal femoral physis. The patient demographics are detailed in Table 1.
Patient demographics and age at surgery. Tilt angle outcomes following screw epiphyseodesis
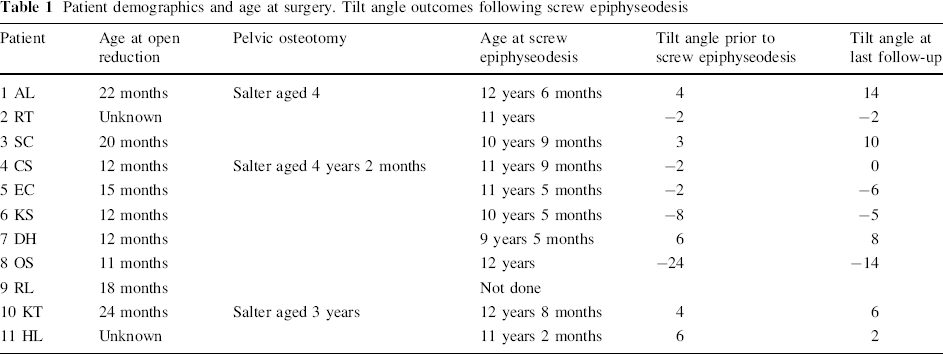
Eleven hips required open reduction (after a 1-week period in traction) via an anterior surgical approach combined with adductor tenotomy to achieve concentric reduction. One case required a proximal femoral shortening osteotomy at the time of open reduction. Three other cases required a pelvic osteotomy (Salter innominate osteotomy) at a later stage. All patients remained under regular clinical and radiological follow-up.
If lateral growth arrest was suspected, the follow-up interval was reduced in order to observe for any progression in lateral growth arrest. However, it was evident from the patient records that there were no specific criteria or consensus for the timing of screw epiphyseodesis. When surgery was indicated, a percutaneous technique using a single cannulated, partially threaded cancellous screw was used to position the threaded portion of the screw across the open segment of the physis.
A consistent finding in other reports is that it can be difficult to identify lateral growth arrest at an early age. In an attempt to overcome this issue, we devised a new technique that can be used for early detection and which can be applied to identify trends in lateral growth arrest. This tool may be of benefit in determining the appropriate timing of surgical intervention (screw epiphyseodesis) and is helpful in monitoring the outcomes of surgery until skeletal maturity. We have called this technique the ‘Tilt angle’ (Fig. 1). This is described below.
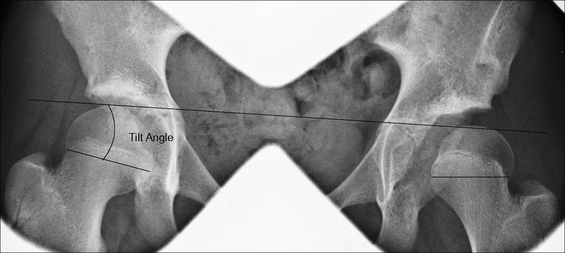
Calculating the ‘Tilt angle’. A horizontal reference line is used (Hilgenreiner's line or the inferior margin of the teardrop). The physeal line is the line that joins the lateral and medial aspects of the capital physis. The tilt angle is the angle formed between the physeal line and the horizontal reference line. Note that, in the normal hip (right), the physeal line runs from superolateral to inferomedial. In the affected hip (left), if there is excessive tilt, then the physeal line runs from inferolateral to superomedial and, in these cases, a negative value is assigned to the angle for the purposes of data interpretation
A horizontal reference line is used, for example, Hilgenreiner's line or the inferior margin of the teardrop. A second line, the physeal line, is then identified, joining the most lateral and medial points of the physis. The intervening angle between the reference line and the physeal line is the ‘Tilt angle’. Note that, in the normal hip, in this example, the right hip, the physeal line runs from superolateral to inferomedial and the tilt angle is assigned a positive value for the purposes of data interpretation. If there is excessive tilt, i.e. a physeal line running from inferolateral to superomedial, then a negative value is assigned to the tilt angle. It is important to recognise that only standard anteroposterior (AP) radiographs of the pelvis and proximal femora (i.e. correct positioning of limbs with internal rotation to account for femoral anteversion with the patella facing forward) can be included, as any deviation with regard to hip adduction, abduction or rotation could potentially affect the value of the tilt angle. If these radiological criteria are adhered to, then this technique is particularly valuable for early detection of lateral growth arrest and the identification of changing trends that may prompt timely surgical intervention.
Results
Two independent reviewers obtained tilt angle measurements for both normal and affected hips in the serial radiographs of 11 patients. Statistical analysis was performed using Bland–Altman plots to assess the reproducibility of the technique [2]. There was no significant difference between the two sets of values for either hip (P-value for correlation was 0.97 and 0.75 for affected and normal hips, respectively) (Figs. 2 and 3).
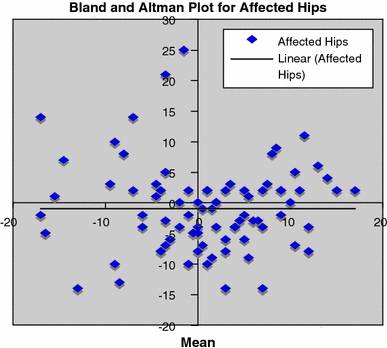
Bland–Altman plot of the tilt angle measurements for hips with lateral growth arrest. Correlation R = 0.0037 (P-value 0.97)
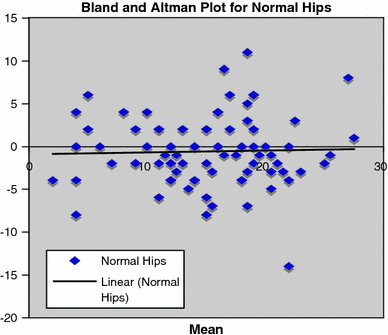
Bland–Altman plot of the tilt angle measurements for normal hips. Correlation R = 0.034 (P-value 0.75)
Using the tilt angle technique, measurements for both normal and affected hips for each individual were plotted graphically. Figure 4 illustrates the data for one individual. Tilt angle measurements were recorded from 2.5 years of age. It is evident that the trend for the normal hip tilt angle remains relatively constant over time. In comparison, the hip with lateral growth arrest demonstrates deterioration in the tilt angle, especially after 8 years of age. In this patient, screw epiphyseodesis was performed at 12 years of age and the subsequent improvement in the tilt angle measurement may suggest a role for guided growth. Similar findings were noted in the other patients in this series and pre- and post-operative tilt angle values at the final follow-up are included in Table 1. Improvement in tilt angles following screw epiphyseodesis was observed in seven individuals, with deterioration noted in two. No change was recorded in one patient.
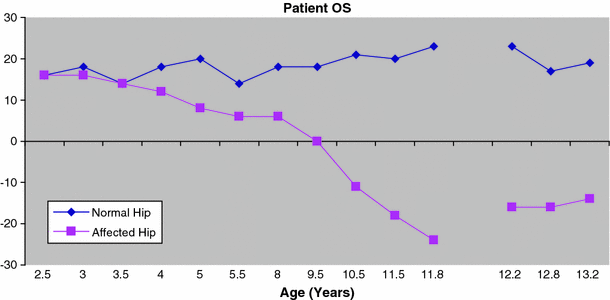
Patient OS. Avascular necrosis (AVN) suspected at age 5 years according to the case notes. Lateral growth arrest first documented at the age of 10 years. Note the significant deterioration in the tilt angle after 8 years of age. Screw epiphyseodesis carried out at 12 years of age (gap in the chart lines). Improved tilt angle post-surgery until physis closed at 13.2 months
One case did not have screw epiphyseodesis and Fig. 5 illustrates the outcome in this patient. It is evident that the trend for the normal hip shows little variation over time; however, in the affected hip, there is clearly a significant change in the tilt angle trend beyond 6 years of age. Figure 6 illustrates the serial radiological change in this individual.
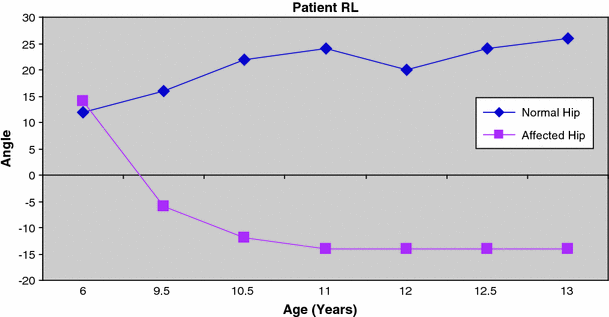
Patient RL. Lateral growth arrest first documented at the age of 10 years. Screw epiphyseodesis not performed
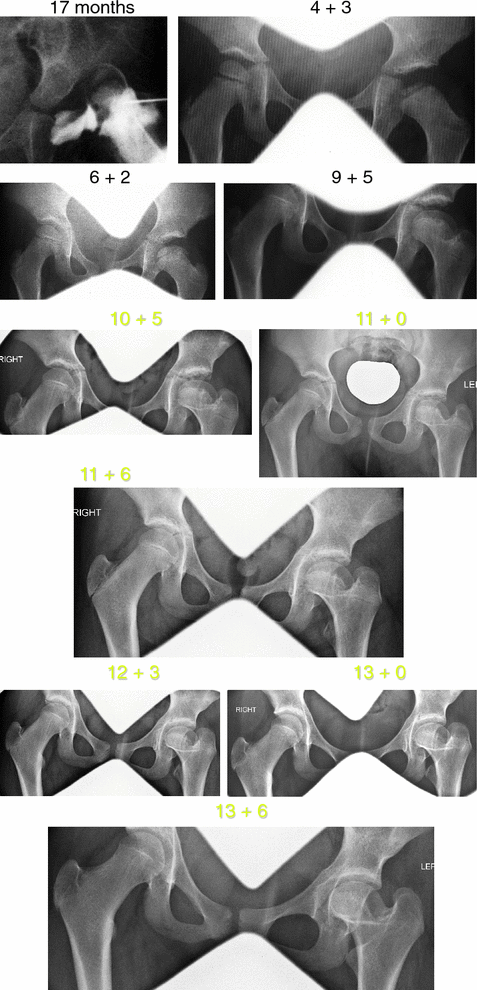
Radiographic series for patient RL demonstrating progression of lateral growth arrest and change in tilt angle over time
The average age of screw epiphyseodesis in this series was 12 years.
Discussion
Lateral growth arrest is recognised as the most common form of AVN seen following treatment for DDH [1]. Many studies [1, 3–6] have described the aetiology and clinical outcomes following lateral growth arrest; however, very few have discussed the management of these cases. Gage and Cary [7] concluded that trochanteric epiphyseodesis was necessary to prevent relative trochanteric overgrowth in DDH. However, to our knowledge, the effects of screw epiphyseodesis on the medial capital physis have not been described. We, therefore, devised a new technique to identify early lateral growth arrest (Fig. 1) that can also be applied to serial radiographs for monitoring and, indeed, to assess the outcomes following screw epiphyseodesis. The ‘Tilt angle’ technique can be applied to standard AP pelvic radiographs, is easily reproducible, is not subject to significant intra- or inter-observer variability and, perhaps most importantly, may serve as a useful tool to guide timely surgical intervention with medial screw epiphyseodesis to allow optimal potential for guided growth.
Much interest recently has centred on describing the 3-dimensional changes associated with lateral growth arrest. In a series of 11 patients, Joo et al. used computed tomography to form 3-dimensional reconstructions of the proximal femur [8]. In addition to the typical valgus configuration seen in the coronal plane on standard AP pelvic radiographs, their work demonstrated increased antetorsion and anteversion in a significant proportion of cases. Furthermore, they identified that the physeal bridge may, in some cases, be located in the posterolateral area of the capital femoral physis, though it was seen to lie anterolateral in the majority of cases (5 hips out of 6). Whilst we accept that this is an important study in understanding the complex 3-dimensional deformity associated with lateral growth arrest, it is not without risk or burden in the clinical setting and may add little extra to surgical decision-making for screw epiphyseodesis, above and beyond the information that can be obtained from simple AP and lateral radiographic analysis. One must consider the radiation doses involved and the requirement of sedation or general anaesthesia, particularly in younger patients, in order to obtain optimal imaging.
Other reports have also described the radiological features of lateral growth arrest. Oh et al. stated that lateral growth disturbance of the proximal femur can be recognised radiologically by the following criteria: (a) lateral tilt of the capital epiphysis on the neck, (b) length of neck being shorter on the lateral side compared with the medial side and (c) bridging of bone across the lateral physis. However, they did acknowledge that it can be difficult to identify lateral growth arrest at an earlier age [9]. In our study, we noted limitations when these principles are applied for sequential radiological analysis. In particular, lateral tilt of the capital epiphysis, if measured using a line joining the most medial and lateral aspects of the epiphysis, is subject to significant intra- and inter-observer variability. It is, therefore, an unsuitable tool for serial measurement and trend observation. As described by the authors, the medial to lateral neck ratio is calculated just before closure of the physis and, again, we could not apply this to serial observation. Although the bridging of bone across the physis is easily identifiable, it is very difficult to quantify the extent of the bridge on a 2-dimensional AP pelvic radiograph and again to apply this to serial images to identify a trend.
When planning screw epiphyseodesis, intra-operative imaging with an image intensifier facilitates optimal screw placement across the open segment of the physis (Fig. 7). If screw placement occurs late, then positioning becomes more challenging, as the target area of the open segment of the physis diminishes and the potential for guided growth also reduces. The tilt angle technique may help to avoid late screw placement by the early detection of growth arrest.
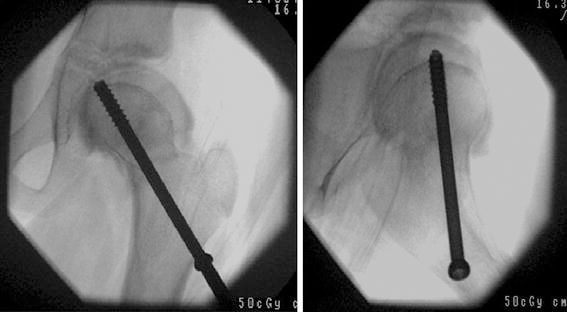
Anteroposterior (AP) and lateral intra-operative images
We accept that there are limitations to the tilt angle technique, for example, the assumption that it is a 2-dimensional analysis in the coronal plane of what is essentially a 3-dimensional abnormality. However, as our results suggest, it can be helpful in the early detection and monitoring of lateral growth arrest. In particular, it is useful for trend observation of changes in growth in the physis and, when compared with trends in the normal hip, may be a valuable simple tool to guide timely surgical intervention. Furthermore, our results do give support for the role of screw epiphyseodesis in guided growth of the proximal femoral physis. Further work is required in order to clarify the optimal timing of screw insertion to maximise the potential for guided growth following the early detection of lateral growth arrest using the tilt angle technique.