
Abstract
Purpose
Posterior only approaches for spinal deformity are increasingly popular and posterior spinal release is utilized to gain flexibility for correctional maneuvers. Prior biomechanical data support the use of facetectomy and rib head resection for gaining flexibility in the sagittal and coronal planes but to date there has been no quantification of stiffness reduction provided by these techniques for axial correction through a pedicle screw construct. We sought to determine the contribution of posterior spinal releases (facetectomy, rib head resection) on axial plane stiffness.
Methods
Four fresh-frozen human cadavers were instrumented with fixed angle pedicle screws in the thoracic spine. The torque needed to produce 25° axial deflections at individual spinal segments (levels T5–T11) was measured using a custom needle deflection torque device attached to commercially available vertebral rotating construct. After the intact specimen was tested, torque measurements were repeated following a full facetectomy and posterior rib head resection
Results
Complete facetectomy resulted in an 18% decrease of torque needed to produce 25° of axial deformity compared to the intact specimen (P < 0.001). Rib resection added an additional 36% decrease in torque (P < 0.001).
Conclusions
Complete facetectomies (Ponte or Smith-Petersen osteotomies) decrease the force required to rotate spinal segments with respect to the axial plane by approximately one-fifth. Posterior rib head resection should be considered to further loosen the spine if additional axial correction is desired.
Introduction
Posterior only approaches for spinal deformity are increasingly popular, with surgeons utilizing more extensive posterior releases, such as Ponte or Smith-Petersen Osteotomies (SPOs) to improve correction [1]. Many authors are reporting that posterior releases with segmental fixation through pedicle screws have obviated the need for anterior releases, or discectomies, to loosen the spine before correction and fusion [2–7].
The axial plane, which manifests as a thoracic prominence also receives greater attention in pedicle screw based correction maneuvers. Benefiting from three-column fixation, direct spinal rotation techniques with pedicle screws are described [8]. Posterior releases, though originally described to shorten the posterior column for sagittal correction, may also serve to improve axial flexibility of the spinal segment.
Extensive posterior spinal release with osteotomy was described in 1945 by Smith-Petersen for correction of kyphosis associated with ankylosing spondylitis [9]. This osteotomy involves resection of the interspinous ligament, spinous processes, ligamentum flavum, and facet joints as well as the inferior portion of the lamella. The deformity was reduced with extension of the operative table and uninstrumented fusion held with serial casting. While associated anterior release has been described as part of the “Smith-Petersen osteotomy” [10], this was not included in the initial description of the procedure. In 2006 the Ponte procedure was described for correction of Scheurmann's Kyphosis with nearly identical ligamentous and osseous resection to the Smith-Petersen osteotomy with the deformity reduced by and fusion held with pedicle screw fixation [1]. For the purposes of this discussion, the terms “Ponte” and “Smith-Petersen” osteotomy will be used interchangeably.
Biomechanical studies on the effect of spinal releases predate common usage of pedicle screw constructs for deformity correction. These studies have not applied forces to the spinal specimens through three-column fixation, such as a pedicle screw construct [11–13]. We are not aware of any evaluation of the biomechanical effect of posterior releases on spinal rotational maneuvers applied through pedicle screws.
In order to determine the decrease in force needed to axially rotate the spine through a pedicle screw construct after a complete posterior release a cadaver model was analyzed.
Materials and methods
Four fresh-frozen human cadavers were used for this investigation. They had been stored at −50°C and were thawed to a cooled room temperature. The specimens had died at ages 59–76 years; none had any known spinal pathology. There were 3 females and one male. The thoracic spine was exposed posteriorly from T4 to T12 level, with only muscular tissue removed; all ligamentous tissue, including the interspinous ligaments, were initially left intact. The cadavers had been used for a cervical instrument demonstration, but no portion of the thoracic region had been disturbed except for our approach to the spine and the thoracic rib cage was intact.
The 5th through 11th thoracic vertebrae were instrumented with pedicle screws. Screws were placed by free-hand technique. No facetectomy was performed at the time of screw placement. Screws were all placed as one typically would place the superior screw in a construct, with every effort to preserve the neighboring facet joint. All screws were 5.5 mm diameter, 45 mm length, fixed angle screws (M8, Medtronic Sofamor Danek, Minneapolis, MN).
Biomechanical testing was performed on levels T5 through T11. Each level was axially rotated 25° with a commercially available segmental rotation construct (Vertebral Column Manipulation instrument set, Medtronic Sofamor Danek, Minneapolis, MN). The construct was attached only to the bilateral pedicle screws at a single level at a time; there was no attempt to perform en bloc rotational maneuvers. Adjoining levels were not fixed, however, no axial rotation was noted beyond the immediately adjacent one or two levels implying minimal torque transmission beyond that range. The rotation applied was also nondestructive in nature, with the spine recoiling back to neutral after torque was released. Each measurement was repeated and recorded 3 times to acquire the most reproducible result. The torque needed to produce 25° axial deflections at individual segments was measured using a custom needle deflection torque device attached to the rotation construct (Fig. 1).

Experimental setup with cadaver spine exposed, pedicles instrumented, segmental spinal derotation instrumentation applied and custom torque measurement device attached
The intact specimen was tested, and used to establish the internal baseline for each level of each specimen. A complete facetectomy and posterior release was performed at all levels tested (T5 to T11—leaving T4–T5 and T11–T12 intact). The interspinous ligament, ligamentum flavum, facet joints and portions of the spinous processes were resected (Fig. 2). These were intended to duplicate common description of Ponte or Smith-Petersen Osteotomies [1]. The torque measurements were repeated following these releases. Finally, bilateral rib head resections were performed; again, all levels were released prior to torque measurements. The medial 2–4 cm of rib, including vertebral and transverse process articulation were removed with roungeur. The torque measurements were repeated for the third time at each level.

Demonstration of complete facetectomy (Ponte or Smith-Petersen osteotomy) prior to rib head resection
The data was analyzed for statistical significance. The data for the torque measurement for intact spine were established as baseline for each level. Each subsequent torque measurement after posterior release and rib resection was measured and compared to the intact data. The percentage of torque required to produce axial deviation of the spine was reported as a percentage of initial baseline. Comparisons were analyzed for statistical significance using the paired t-test, significance set as a P-value < 0.05.
Results
The decreasing torque required to produce 25° of axial rotation at each level after sequential posterior release is recorded in Table 1. The data is presented for each of the 24 levels tested and for the overall result combining all levels tested. Complete facetectomy resulted in an 18% decrease of torque needed to produce 25° of axial deformity compared to the intact specimen (P < 0.001). Rib resection added another 36% decrease in torque from the posterior released specimen (P < 0.001). Rib resection and posterior release combined decreased stiffness by 47% form the intact specimens (P < 0.001).
Percentage change in torque required for 25 degrees of axial deflection at each instrumented level
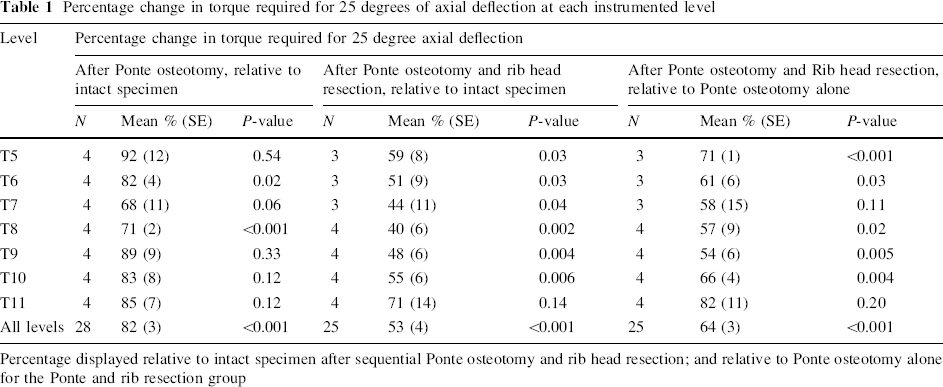
Percentage displayed relative to intact specimen after sequential Ponte osteotomy and rib head resection; and relative to Ponte osteotomy alone for the Ponte and rib resection group
Torque measurements at each level were very consistent over three measurements in all cases. One specimen demonstrated breakage of the pedicles with rotation after rib resection at 3 levels (the upper three, T5 through 7). This specimen's data for these levels was excluded from rib resection measurements.
Discussion
Our analysis of a cadaver model demonstrated that complete facetectomies (Ponte or Smith-Petersen osteotomies) decrease the force required to rotate spinal segments with respect to the axial plane by approximately one-fifth. There has been a number of clinical series reporting excellent results with posterior only treatment of challenging spinal deformity, however, there is a paucity of biomechanical information on this subject.
Feiertag et al. performed a series of experiments on cadaveric torsos, with intact rib cages and sternums, to test anterior versus posterior releases with respect to spinal stability. Greater instability was created by anterior release, consisting of complete discectomy and rib resection than facetectomy and rib head resection from posterior approach [12]. Testing was only for coronal and sagittal planes, and it is unlikely that the unilateral facetectomy would be deemed comparable to currently proposed Ponte osteotomies.
More recently, Oda et al. expanded significantly on Feiertag's work. Sixteen functional spinal units were harvested from 6 cadaver torsos to test anterior to posterior and posterior to anterior releases [13]. The specimens included the posterior 5 cm of ribs and were mounted for testing in flexion, extension, and axial rotation. Specifically the posterior releases described included laminectomy and bilateral total facetectomy. They reported that such a posterior release created 45% increase in axial rotation of the spinal segment with uniformly applied torque. Interestingly, the contribution to motion of the complete facetectomy alone was 15% more than the medial facetectomy. We feel this is consistent with our data showing 18% less torque required for defined motion after complete facetectomy. In the same study, bilateral rib resection created incrementally 82% more motion. Although significant (reported P-values < 0.05), these results were far less impressive than the motion created by anterior discectomy and their conclusion was to recommend anterior release when feasible [13]. Our testing protocol did not include anterior release as we chose to focus on posterior-only procedures.
Most recently, Anderson et al. have tested flexion stiffness in 23 individually mounted thoracic motion segments [14]. They measured torque necessary to produce 3.2 degrees of flexion in the isolated segments. This study found resection of the supraspinous and infraspinous ligaments to provide 6.59% decrease in necessary torque and when combined with complete posterior soft tissue release (facet joints, etc.) a 44.72% decrease. When a Ponte/Smith-Petersen osteotomy was added, the total decrease in torque was 67.71% from intact baseline. This significant increase shown in sagittal flexibility with posterior release is complementary to our study showing significant increase in axial plane flexibility; taken together indicating a decrease in force needed for multi-planar correction from a posterior approach following Ponte/Smith-Petersen osteotomies.
There are a number of limitations of our cadaver model. Specimens provided are typically far older than patients considered for spinal deformity surgery; the mean age of our cadavers at death was 67 years. Age and preparation of specimens may contribute to an osteoporotic spine that behaves differently than an actual spinal deformity patient. In an attempt to address this limitation, a minimal amount of deflection (25°) was tested, to avoid any destructive changes to the specimens. Nevertheless, one specimen did demonstrate breakage of the metal-bone interface with continued testing and had to be discounted prior to post-rib-resection testing.
Unlike prior biomechanical studies, our testing was applied by hand to produce a desired deflection. Most studies have relied upon systems of weights and pulleys [12] or MTS [11, 13, 14] to apply a standardized force to a spinal specimen. This has required that the specimen is segmented and fixed to a testable construct. These systems would seem to have an inherent advantage in reproducibility. However, by applying force to an intact cadaver model by hand, our study potentially more readily duplicated the surgical scenario. The cadavers did not require additional preparation to fit to a testing mechanism, and our application of torque through a pedicle screw construct instead of an endplate rotation is identical to the intra-operative application of forces. Our measurements were notably consistent with regard to repetition (3 measurements in all levels and cases), different specimens, and among the different levels tested. Finally, this model could serve as baseline data for future in vivo investigations on actual spinal mobility in surgical cases.
Summary
Posterior facetectomy or Smith-Petersen/Ponte Osteotomy is thought to decrease the torque required to correct axial deformity. A cadaveric study to test this hypothesis was performed. Posterior facetectomy decreased the torque required to produce axial rotation of 25° through a pedicle screw construct by 18%.
Footnotes
Medtronic Sofamor Danek provided the instruments, implants and cadavers for this project. None of the authors have received funding related to this manuscript.