
Abstract
Purpose
At Haukeland University Hospital (HUH), we used overhead skeletal traction for displaced supracondylar humerus fractures (SCHF) in children until closed reduction and crossed wire fixation was introduced in the early 1990s. Though there are obvious and well-documented benefits of wire fixation, the aim of this study was to document and compare the results and complication rates for both methods.
Patients and methods
One hundred and thirty-nine patients treated for SCHF between 1988 and 1998 were available for follow-up. Of these, 40 children were treated with a plaster cast, 46 with overhead skeletal traction and 45 with crossed wire fixation. Eight children were treated with open reduction and crossed wires. The mean time to follow-up was 7.1 years [standard deviation (SD) 3.2].
Results
The length of hospital stay was 2 days for those treated with crossed wire fixation compared to 11 days for traction (P < 0.001). The rate of nerve injury in Gartland type 3 fractures was 19%. There was no significant difference in the number of complications or in the functional outcome after skeletal traction or wire fixation, but there were more reoperations in the traction group (P = 0.04). Patients treated solely with a plaster cast had a mean of 4° increased extension of the affected elbow compared to 1° in the crossed pin fixation group (P = 0.02). Though this has little clinical relevance, it does indicate improved reduction in the operated patients, as one would expect.
Conclusions
The introduction of crossed wire fixation has significantly reduced the number of days for which patients are hospitalised for SCHF. The rate of nerve injuries in Gartland type 3 fractures is high. Despite the fact that this study includes the first patients to be treated with crossed wire fixation at our institution, no significant increase in the risk of complications could be found compared to skeletal traction.
Keywords
Introduction
A displaced supracondylar humerus fracture (SCHF) is the fracture in childhood that gives the most frequent and serious complications [1–4]. Undisplaced fractures, Gartland type 1, are generally treated with immobilisation in a cast with good results [3, 5, 6]. Historically, there has, however, been shown to be considerable danger of serious complications with the treatment of displaced SCHF in a plaster of Paris (POP) cast with hyperflexion [4]. This is why Dunlop started using skin traction for these fractures in the late nineteen twenties [7]. This reduced the rate of serious complications significantly [8], but still resulted in up to 33% cubitus varus deformity [9]. Skeletal traction with a K-wire [5, 10] or a screw [11] in the olecranon was later shown to give better control of the fracture reduction. In 1939, Miller described “blind nailing” of distal humeral fractures in adults [12] and in 1948, Swenson suggested percutaneous crossed pin fixation for SCHF in children [13]. He used this method to avoid complications and deformity when the elbow was too swollen or the fracture too unstable to treat well with hyperflexion in a POP cast. Flynn et al. [14] used crossed pin fixation from 1956 and published their results, including a classification for outcome for SCHF, in 1974. Pirone et al. [15] examined 230 children treated for SCHF and compared 130 fractures treated with a POP cast with 78 treated with crossed K-wire fixation and 24 treated with skeletal traction. They concluded that crossed wire fixation was the method that gave the best results and that it was a safe method. Controversy, however, remains over whether one should use crossed wire fixation or two radial pins to avoid iatrogenic ulnar nerve injury [16, 17].
During the 1980s and -90s, crossed wire fixation came to be universally accepted as the treatment of choice. It was introduced to Haukeland University Hospital (HUH) in 1992 by the senior author (LE). Before this, overhead skeletal traction was used as the standard treatment for SCHF at HUH, and from 1992 until crossed wire fixation was firmly established as the treatment of choice in 1995, skeletal traction was still used by surgeons on call. Though there are obvious and well-documented benefits of wire fixation, the aim of this study was to document and compare the results and complication rates of overhead skeletal traction and crossed wire fixation.
Patients and methods
HUH is a tertiary referral centre for paediatric orthopaedics and trauma for a population of approximately 900,000 in Western Norway. It is the only hospital treating displaced SCHF in a population of approximately 300,000 in and around the city of Bergen. The majority of undisplaced fractures are, however, treated at a separate institution, Bergen Legevakt (BLV).
Two hundred and sixty-eight patients were treated at HUH for a distal humerus fracture from 01.01.1988 to 31.12.1998. By reviewing the case notes of these patients, 181 consecutive patients with SCHF were identified. One patient had bilateral fractures and was excluded because function and deformity could not be compared to an uninjured arm. A total of 141 patients were available for follow-up. Two of these turned out to be lateral humerus condyle fractures and were excluded, leaving 139 patients. The parents of all of the children gave their informed consent to their child partaking in this study.
All 139 patients were examined in the outpatient clinic of our institution by one of the authors, on days specifically set up for this study. The patients were seen after a nurse had pulled a stocking over both arms so that the examiner could not see any scars and was, therefore, “blinded” to the type of treatment and side of injury. Elbow carrying angle, extension and flexion, lower arm rotation and shoulder external rotation was recorded for both arms.
The carrying angle is the angle between the upper and lower arm with the elbow in 0° extension and was measured using a goniometer. Lower arm rotation was recorded as degrees of supination and pronation from the neutral position with the elbow flexed 90°. The maximum external rotation in the shoulder was measured with the glenohumeral joint in the neutral position in the sagittal and frontal plane and the elbow in 90° of flexion. We also tested nerve function and vascular status (pulse, capillary refill, temperature). Nerve function was tested by comparing the two sides. Reduced sensation (touch or pain/pinprick) compared to the other side for one or more nerves was registered as sensory nerve loss. Testing function and strength in flexion of the distal interphalangeal joint of the 5th (ulnar nerve) and 2nd (median nerve) finger and dorsal flexion of the wrist and metacarpophalangeal joints (radial nerve) was used as a screening test of motor function.
The medical records of all patients were examined separately from the clinical examination. We recorded the injured arm, the date and time of injury, time of admittance and time of surgery. Pre- and post-operative vascular status, nerve function, infection and the number of reoperations were also noted. The activity of the children when they were injured and the place of injury was also recorded.
The patients were divided into four groups according to the treatment they received; POP cast only (40 children), overhead skeletal traction (46 children), closed reduction with percutaneous crossed wire fixation (45 children) and open reduction with crossed wire fixation (8 children).
Fracture classification and treatment selection
The fractures were classified retrospectively using Wilkins’ modified version of Gartland's classification [3, 6]. Type 1 fractures are minimally displaced, extension type fractures, defined as having the anterior humeral line [18] transect some part of the capitellum ossification centre. Type 2 fractures may also have only dorsal angulation, but the whole ossification centre is behind the anterior humeral line. There may be some rotation or lateral angulation of the distal fragment, but there is some posterior cortical contact. Type 3 fractures are totally displaced and there is total loss of contact between the fragments.
In 25 of the 139 cases in this series, the primary X-rays were not available at follow-up and the Gartland type was, therefore, determined only from the radiologist's X-ray report and the case notes when possible. In four of these cases, it was not possible to classify the fracture from the notes (Table 1).
Type of treatment versus Gartland type
The distribution of Gartland types in the different treatment groups can be seen in Table 1. There is no difference in the distribution of fracture types between the closed reduction wire fixation and traction groups (P = 0.43). Nor did we find any difference between these two groups and the open reduction group (P = 0.83, P = 0.61). Not surprisingly, there is, however, a significant number of less displaced type 1 and 2 fractures in the POP group compared to the wire fixation (P < 0.001) and traction (P < 0.001) groups. Six of the 139 fractures, or 4%, were flexion type injuries. Five of these were severely displaced and classified as Gartland type 3. The sixth was not classifiable.
Treatment methods/surgical technique
POP cast group
Undisplaced fractures were treated with a POP cast with the elbow flexed at 90°. The cast was, as a rule, applied in the emergency room without anaesthesia and no attempt at reduction or casting in flexion more than 90° was done for fear of complications. In three cases, however, we found that closed reduction and plaster cast alone was done under general or regional anaesthesia.
Overhead skeletal traction
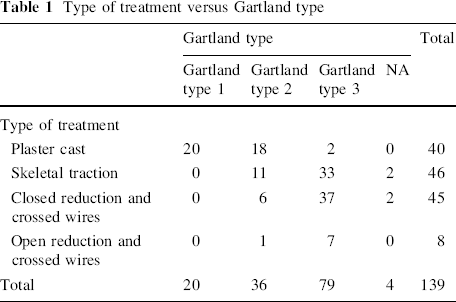
With the patient under general anaesthesia, the fracture was reduced, a winged Palmer screw [11] was placed in the olecranon and traction was arranged as shown in Fig. 1. The patients were confined to bed. On the 10th to 12th day, a plaster cast was applied to the arm while still in traction. The traction was removed and the arm was immobilised in this plaster cast for a further 2–3 weeks, i.e. a total immobilisation period of approximately 4 weeks.
Crossed wire fixation
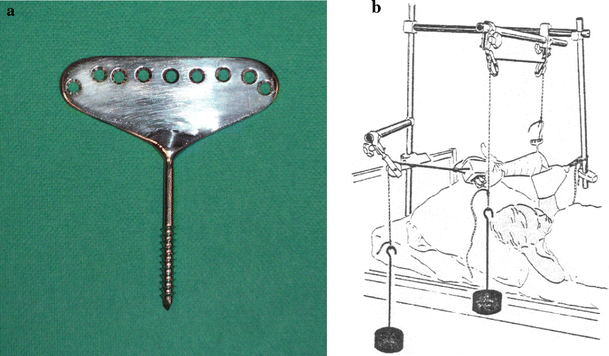
The patients were treated under general anaesthesia. The fracture was reduced by manual traction with the elbow in extension, followed by flexion of the elbow with simultaneous pressure applied to the proximal surface of the olecranon. Reduction was checked with a C-arm image intensifier. A 1.6-mm Steinmann pin/Kirschner wire was inserted percutaneously from the radial condyle, or from the ulnar side, depending on the fracture, across the fracture and out the opposite side of the proximal fragment. We let the pins only just perforate the opposite cortex to get the best possible fixation in the proximal fragment. Similarly, a pin was placed from the other side. The ulnar pin was placed with special attention in order to avoid the ulnar nerve in its groove. The pins were cut and bent 1 cm outside the skin to prevent migration and facilitate easy removal. Reduction and pin placement was checked with the image intensifier before the application of a cast from the wrist to the axilla with the elbow in 90° of flexion. An example of pre- and post-operative X-rays is shown in Fig. 2. The pins were removed in the outpatient clinic without an anaesthetic 4 weeks post-operatively.
Eight patients were treated with open reduction and crossed pin fixation when the fracture could not be reduced to an acceptable position by closed means or opening the fracture was considered necessary because of neurovascular injury. These fractures were registered as a separate group so that we could study factors, such as time to surgery, relating to these patients separately.
No specific exercises or physiotherapy was recommended after cast removal. All children treated for SCHF in our hospital are given a clinical follow-up appointment approximately 3 months after cast removal to assess the functional outcome. This was also the case for the children in all four of the above groups.
Criteria for grading outcome
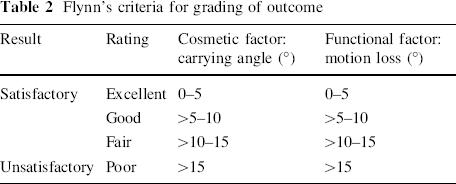
We used Flynn's criteria [14] for outcome to compare the results of treatment in the four groups. In this classification, separate scores are given for carrying angle (cosmetic score) and range of motion (ROM) (functional score). Flynn's criteria for outcome can be seen in Table 2.
Flynn's criteria for grading of outcome
Statistics
Student's t test was used to compare the means of continuous variables between the treatment groups. The Chi-squared test was used to compare categorical variables between the different treatment groups. All P values were two-tailed and the level of statistical significance was set to 5% (P ≤ 0.05). All analyses were done using SPSS versions 14.0 and 15.0.
Results
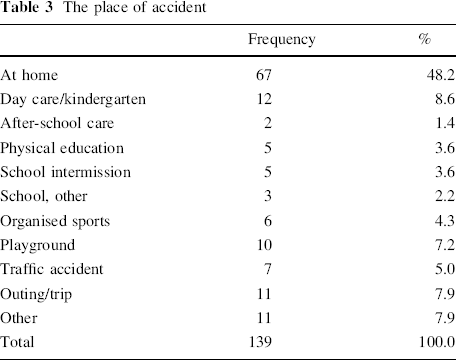
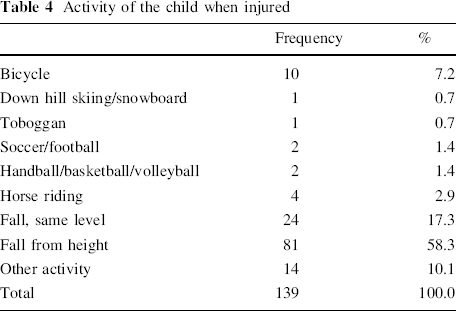
Sixty (43%) of the 139 children included in this series were girls and 79 (57%) were boys. The mean age at injury was 6.6 (1–13.5, standard deviation [SD] 2.7) years for the whole patient series; for girls it was 6.9 (SD 2.8) years and for boys it was 6.4 (SD 2.7) years (P = 0.29). The left arm was injured in 57% of the children and the right in 43%. The activity of the child when the injury occurred and the place where the injury occurred was registered and the results can be seen in Tables 3 and 4. Most (81%) injuries occurred at home or out of school, including 4.3% during organised sports like soccer, handball etc. Nineteen percent of injuries occurred at school or in day care. A fall from height (a tree, horse riding etc.) was the mechanism described in 61% of the cases. The distribution of fractures per month can be seen in Fig. 3. Only 19.1% of the fractures were sustained in the winter months of November to February and only 1.4% of the fractures occurred during typical winter sports. The time from injury to follow-up had a mean of 7.1 (2.5–15.6, SD 3.2) years for the whole group and for plaster cast (POP) 6.1 (SD 2.5), skeletal traction 9.9 (SD 2.5), crossed wire fixation 5.2 (SD 2.4) and open reduction 6.9 (SD 2.9).
The place of accident
Activity of the child when injured
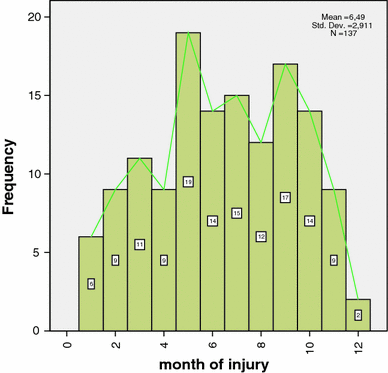
Month of injury
The median length of hospital stay in the POP group was 1 day (range 0–9), in the skeletal traction group 11 days (range 2–16), in the closed reduction pin fixation group 2 days (range 1–31) and in the open reduction group 2 days (range 2–6). The difference in the length of hospital stay between the skeletal traction and crossed pin fixation groups was highly statistically significant (P < 0.001).
The time of injury was recorded in 64 of the 99 patients operated. The median time from injury to surgery was 6.0 h (range 1.6–21.3) in these patients. In the closed reduction and crossed pin fixation groups, the time from injury to surgery was more than 8 h in 6 of the 37 patients for whom this information was available. For those where open reduction was necessary, 3 of 7 had to wait more than 8 h for surgery. This difference, however, was not statistically significant (P = 0.11).
Residual deformity at final follow-up
At final follow-up, no statistical differences in clinical measurements were found between the three groups of patients that received operative treatment. Though not clinically relevant, there was, however, a slight difference in elbow extension and carrying angle between the POP and closed reduction pin fixation groups. Elbow extension was increased by a mean of 4.3° (SD 5.2) in the POP group, from mean 12.9° extension on the uninjured side to 17.2° on the injured side at follow-up. In patients treated with crossed pin fixation, this increase was just 0.8° (SD 7.7) (P = 0.018). There was also a slight difference in the carrying angle between these two groups. The mean reduction in the carrying angle compared to the uninjured side was 1° (SD 6.6) in the POP group compared to 4.8° (SD 6.9) in patients treated with crossed pin fixation (P = 0.012).
Outcome/Flynn class
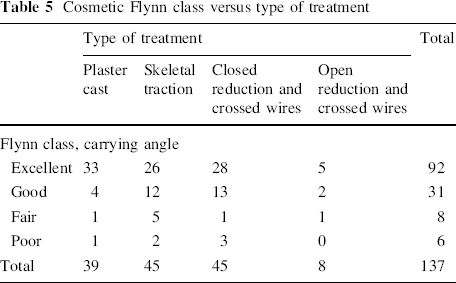
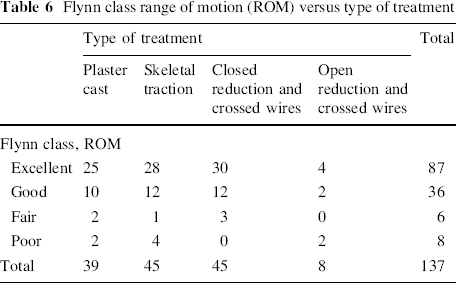
Flynn's criteria [14] for outcome can be seen in Table 2. In Table 5, we present the patients in four categorical groups according to Flynn's classification for cosmetic outcome (carrying angle) and the type of treatment. We found no significant difference in outcome between the treatment groups (P = 0.22). In Table 6, we present the equivalent for functional outcome (ROM). No significant difference was found in functional outcome (P = 0.34). When all patients were seen as one group, 123/137, or 90%, had an excellent or good result (both cosmetic and ROM). Flynn et al. defined excellent, good and fair outcomes as satisfactory results. Using their criteria, 94% of patients had a satisfactory outcome in this series as a whole.
Cosmetic Flynn class versus type of treatment
Flynn class range of motion (ROM) versus type of treatment
Complications
Neural injury
Signs of nerve injury were found at some point during treatment or follow-up in 17 (12.2%) of the 139 included patients. Fifteen of these occurrences were in patients with Gartland type 3 fractures, making the rate of nerve injury in Gartland type 3 fractures 19% in this series. The median nerve was injured in nine patients, the radial nerve in six and the ulnar nerve in three patients. The distribution of neural complications according to treatment method is presented in Table 7.
Nerve injuries
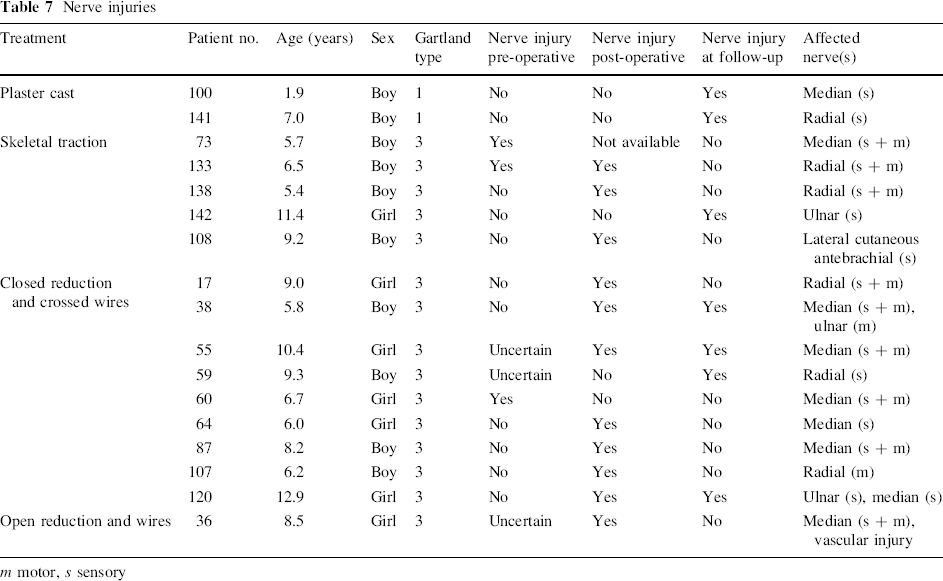
m motor, s sensory
In the plaster cast group, two patients were found to have sensory loss of the median and radial nerve, respectively, at follow-up. This had not been diagnosed prior to the follow-up visit.
We found no statistically significant differences in the rate of nerve injuries at final follow-up between the plaster cast group and the skeletal traction (P = 0.49) or crossed wire fixation groups (P = 0.50). Likewise, there was no significant difference in the rate of nerve injuries between the skeletal traction group and the crossed wire group at final follow-up (P = 0.18). The apparent increased rate of nerve injuries post-operatively in the crossed wire fixation group was not statistically significant when compared to the skeletal traction group (P = 0.25) or the open reduction group (P = 0.82). This was also the case when only cases with potential iatrogenic nerve injury that had no nerve injury prior to surgery were selected in the traction and crossed wire groups (P = 0.28). One patient in the traction group (patient no. 108) had transient anaesthesia on the lateral aspect of the forearm after reoperation with crossed wires because of a fracture that would not reduce in traction. If this patient is included in the crossed wire group for analysis, there is still no statistically significant difference between the groups whether all patients with a registered nerve injury are analysed (P = 0.26) or if only cases that had no nerve injury prior to surgery are selected (P = 0.09).
Vascular injury
In the skeletal traction group, two patients had a weak radial pulse on admittance. In both of these cases, the pulse normalised after treatment. One child in the same group was noted to have a cold extremity after treatment, but this normalised on the first post-operative day. In the closed reduction and crossed pin fixation group, three patients had a weak or absent radial pulse pre-operatively, but the pulse reappeared after reduction in all cases. One child had a primary open reduction with exploration of the brachial artery because of a cold, pulseless extremity that did not improve. At the time of surgery, the median nerve and brachial artery were found to be impinged in the fracture. The artery was repaired with a venous patch.
Infection
There were no registered cases of infection in any of the treatment groups in this series.
Reoperations
Four of the 46 patients treated with skeletal traction had reoperations because of unsatisfactory primary reduction or redislocation of the fracture during traction. One child had remanipulation of the fracture under general anaesthesia and continued skeletal traction, two children were treated with open reduction and crossed wire fixation and one with closed reduction and crossed wires. The two children treated with open reduction were not included in the open reduction and crossed wire fixation groups. There were no reoperations in the closed reduction and crossed wire fixation groups and, compared to the traction group, this was a significant difference (P = 0.04).
Discussion
The epidemiological data in this series is consistent with earlier publications [3, 15]. There are more boys (57%) than girls, more left elbows (57%) than right and the mean age at injury was 6.5 years. It is interesting to see that, even in a winter sport nation like Norway, SCHF is predominantly a summer injury, with a fall from height as the most usual mechanism of injury and only 1.6% (2/120) of the fractures occurred during typical winter sports. In 1998, all fractures in children were registered prospectively in Bergen [19]. The incidence of fractures was found to be 245 per 10,000 children under 16 years of age. Sixty-three of 1,725 (3.7%) registered fractures in that study were SCHF. The fact that most undisplaced SCHF are treated at another institution in Bergen (Bergen Legevakt) accounts for the relatively few type 1 fractures in our series.
The incidence of nerve injury with SCHF has been reported to be between 12 and 20% [1, 2, 15]. Twelve percent of the 139 patients in this series had a nerve injury. Fifteen patients with Gartland type 3 fractures had signs of nerve injury at some point, making the rate of nerve injury in Gartland type 3 fractures 19% in this series. No nerve injuries were found in patients with Gartland type 2 fractures. In the plaster cast group, two patients were found to have sensory loss of the median and radial nerve, respectively, at follow-up. This had not been diagnosed prior to the follow-up visit. Both of the fractures were Gartland type 1 and it is not probable that these nerve injuries resulted from the fracture. It is possible that these nerve injuries are a complication of a tight POP cast. Two of the patients in the crossed wire group and one in the traction group had an ulnar nerve injury at follow-up that was not recognised pre-operatively (Table 7). Both of the children treated with crossed wires also had median nerve involvement. It is very possible that these children have iatrogenic nerve injuries, but, because of the multi-nerve involvement, this is not likely to be due to pin placement alone. A Palmer winged olecranon screw was used in the traction patients and, therefore, no medial entry point was used in these patients. Median and radial nerve injuries are more common than ulnar injuries in this series. The apparent increase in the total number of neural injuries seen in Table 7 in the crossed wire fixation group (9/45) compared to the skeletal traction group (5/46) was not significant (P = 0.25), but there is a weak correlation, and one cannot help to speculate if this would not be different if the study groups had been larger. However, this cannot be answered with our study's size and design.
Though hardly clinically relevant, there was, in this series, a statistically significant (P = 0.018) increase in elbow extension of 3.5° in the POP group compared to patients treated with crossed pin fixation. We do not presume to be able to measure the clinical ROM or angles to tenths of a degree, or even differences of only a few degrees, but this number does, in our opinion, say something about a difference in the average of the two groups. We interpret this to represent an extension deformity that has not remodelled after 7 years follow-up. Conversely, there was 4° more loss of carrying angle in the crossed wire group compared to the POP patients. Both of these differences can probably be explained by the difference in distribution of fracture types in the two groups. In the POP group, fractures were less displaced than in the crossed wire group, but there was quite a high proportion of type 2 fractures that had been left with an extension displacement in the cast, as hyperflexion casting was not used for fear of complications. In the crossed wire group, however, the posterior angulation of the fractures was reduced as exactly as possible in all cases. It is also probable that the difference in fracture distribution, with more type 3 fractures in the crossed wire group, can account for the reduction in the mean carrying angle in this group.
There was no difference in the residual deformity at follow-up between the skeletal traction and open and closed crossed wire fixation groups. The outcome was graded as excellent or good in 90% of patients according to Flynn, with satisfactory results in 94% of patients. We found no difference in the rate of complications in any of the groups. This confirms earlier studies that show skeletal traction and crossed wire fixation to be equally accurate and safe treatment options for Gartland type 2 and 3 fractures [3, 15]. The obvious difference between the two treatments is seen in the duration of the hospital stay. This was a median of 11 days (2–16) for the children treated with skeletal traction, 2 days (1–31) in the closed reduction pin fixation group and in the open reduction group, it was 2 days (range 2–6). The markedly shorter hospital stay for children treated with crossed wire fixation is, of course, of great benefit to the patient and the family and reduces the cost of treatment. Both treatments necessitate a minor operation under general anaesthesia and the later removal of hardware (pins or Palmer screw) during or at the end of treatment. The Palmer screws were removed under general anaesthesia, whereas the pins are removed with premedication only.
The time from injury to surgery was more than 8 h in 6 of the 37 patients for whom this information was available in the closed reduction and crossed pin fixation groups. In 3 of 7 patients in the open reduction group, the time to surgery was more than 8 h. This difference is not statistically significant (P = 0.11). Walmsley et al. [20] reviewed 171 type 3 fractures and found an increased rate of open reduction (33.3% vs. 11.2%) if surgery was delayed by more than 8 h. There are several other recent studies that have not been able to show any difference in the rate of open reduction if surgery is delayed [21–26]. There was no increase in the rate of complications after open reduction in this series. Our current opinion is that surgery for SCHF can wait until the next day if there are no signs of neurovascular injury, so that a surgeon with sufficient experience of these fractures can be present.
This study has all of the normal limitations of a retrospective study. However, the fact that the patients are selected consecutively before and after the introduction of a new method makes the groups more comparable in our opinion. There is also a relatively long follow-up of 7.1 years (SD 3.2). The study sheds light on the fact that the results were no worse with crossed wire fixation, even though the method was new to the surgeons at the time. One criticism of the study could be that the time to follow-up in the wire fixation and traction groups was different. In the skeletal traction group, the mean age at follow-up was 16.7 years (SD 3.8) and the patients, as a consequence, were mostly skeletally mature. The mean age in the wire fixation group was 11.8 years (SD 3.0) and the patients were still growing, though very little growth potential is left in the distal humerus at this age. This might, theoretically, be a source of bias, but would, in that case, give more remodelling and potentially better results in the wire fixation group. The results are, however, already very good and can only get marginally better.
Conclusions
The introduction of crossed wire fixation has significantly reduced the number of days that patients are hospitalised for supracondylar humerus fractures (SCHF). The rate of nerve injury in Gartland type 3 fractures in this series is high (19%). However, despite the fact that this study includes the first patients to be treated with crossed wire fixation at our institution, no statistically significant increase in the risk of complications could be found with crossed wire fixation compared to skeletal traction.
Overhead skeletal traction with a winged Palmer screw is also a safe and accurate method which leaves little deformity and can still be considered in institutions where crossed wire fixation is not possible because of the lack of resources or qualified surgeons. Both methods result in an excellent outcome for the vast majority of patients.