
Abstract
Purpose
Neglected congenital muscular torticollis (CMT) is a common presentation in developing countries like India, with the primary concern of the patients being cosmesis. Little has been published regarding the management of such patients. The aim of our study was to evaluate the results of bipolar release in this age group.
Methods
Over a period of five years, 14 patients older than ten years (range 10–19 years) with neglected CMT were operated on with bipolar release of sternocleidomastoid muscle and z-plasty lengthening of the sternal end. Postoperative protocol included head halter traction for three weeks followed by intensive physical therapy. Results were evaluated using a modified version of the system of Lee et al.
Results
At an average follow-up of around three years (range 1–5 years), excellent results were noted in three patients, good in seven, fair in two, and poor in two. Postoperative improvements in range of motion, head tilt, chin deviation and cosmesis were noted in all patients, and these improvements were statistically significant. No surgery-related complications or recurrences requiring surgery occurred in any of the patients.
Conclusions
This study concluded that patients with CMT presenting after ten years of age definitely benefit from surgery, and that bipolar release is an adequate and complication-free method for such patients.
Introduction
Congenital muscular torticollis (CMT) is the third most common congenital musculoskeletal anomaly after dislocation of the hip and clubfoot [1], with a reported incidence of 0.3–1.9% [2, 3]. There seems to be a slight male preponderance of CMT cases, with a relative ratio of approximately 3:2 [4]. The right hand side is more frequently affected [5].
Patients with congenital muscular torticollis present with tilting of the head toward the affected side due to a fibrotic and shortened sternocleidomastoid muscle [1]. Skull and facial asymmetry or plagiocephaly may occur in the presence of prolonged uncorrected head tilt. The characteristic appearance associated with torticollis includes recessed eyebrow and zygoma, deviation of the chin point and nasal tip, inferior orbital dystopia on the affected side, commissural canting toward the affected side, inferiorly and posteriorly positioned ipsilateral ear, and distorted craniofacial skeletal structures [6].
When diagnosed early, CMT can be managed conservatively with good or excellent results. In fact, spontaneous resolution is expected in most patients [5, 7]. In patients over one year of age, corrective surgery has both cosmetic and functional benefits, with the best outcomes being obtained between the ages of one and four [8]. After the age of five, the form and efficacy of treatment are controversial. Some authors have stated that operative treatment is of little value after this age, and the results are even worse when the operation is done after puberty and may lead to more complications [9].
Neglected congenital torticollis is quite common in developing countries like India, where patients commonly present at an age of more than ten years. Little has been published on the management of such patients. The aim of our study was to evaluate the results of bipolar release in this age group.
Materials and methods
Over a period of six years, 14 cases were operated on for neglected congenital muscular torticolis. Inclusion criteria included age more than ten years, absence of any previous surgery, and absence of any congenital malformation. Detailed birth and family history data were taken. No pathology that could have been the cause of the torticollis was determined in any of the patients, and there were no other congenital deformities. Preoperative assessment was done for restriction of neck movements, head tilt and facial asymmetry, as per the scoring system of Lee et al. [10].
Bipolar release was performed (i.e., release of both the inferior and the superior head) in all cases. Inferior release was done through an incision 1 cm above the the medial third of the clavicle. The clavicular head was released completely while the sternal head was lengthened by z-plasty. The mastoid head was released though an incision just below the tip of the mastoid process. All tight fascial sheaths were released, taking due precaution not to injure any neurovascular structure. It was not necessary to release the carotid sheath in any of the cases.
The postoperative protocol included head halter traction for three weeks and physiotherapy, including both active and passive movement. After three weeks, traction was applied during the night only. During the day the patient was put on a cervical collar. Patients were reviewed every three weeks for three months, six-weekly for one year, and thereafter every six months. At each follow-up, neck range of movement (ROM), head tilt and craniofacial asymmetry were assessed. At the final assessment, postoperative complications (including scarring, loss of sternomastoid column, and lateral bands) were recorded. A scoring system modified from Lee et al. [10], which included function and cosmetic results, was used. An excellent result corresponded to 17–18 points; a good result to 15–16 points; a fair result to 13–14 points; and a poor result to less than 12 points (Table 1).
Scoring system for assessment of congenital muscular torticollis; modified from Lee et al. [10] (LOR is limitation of rotation)
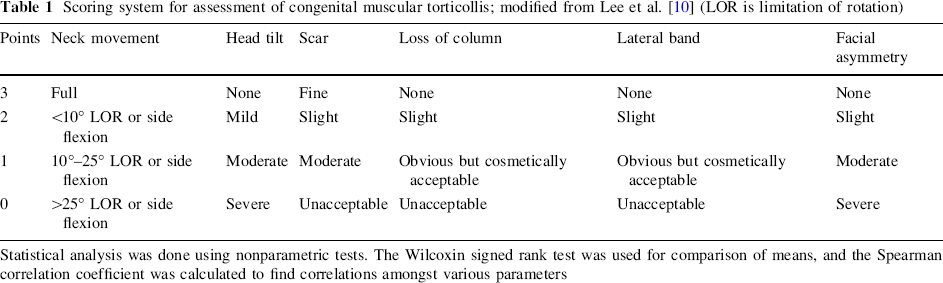
Statistical analysis was done using nonparametric tests. The Wilcoxin signed rank test was used for comparison of means, and the Spearman correlation coefficient was calculated to find correlations amongst various parameters
Results
Mean age of the patients was 13.4 years. Nine of the patients were boys while five were girls, and their ages at presentation ranged from ten years to nineteen years. Eleven of the patients had involvement of the right side, while three had involvement of the left side.
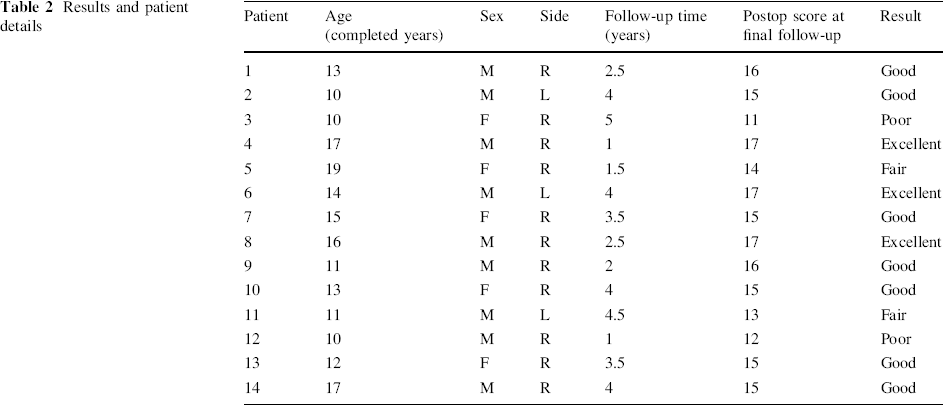
The mean follow-up for the patients was around three years (range 1–5 years). Excellent results were noted in three patients, good in seven, fair in two, and poor in two (Table 2). No surgery-related complications or recurrences requiring surgery occurred in any of the patients. The age of the patient was not found to have any statistically significant relationship with postoperative results.
Results and patient details
Postoperatively there was improvement in the functional range of movement in all patients. Restriction of movement was 10–25° in only one patient. Others had movements within normal limits or a restriction of less than 10°. Cosmetic improvement in the form of reduction in head tilt and chin deviation was present in all patients. Postoperative head tilt was mild or fully corrected in ten of the patients, while none had an unacceptable head tilt postoperatively. The V-shape of the neck at the sternum was retained in all 14 patients, as we performed a z-plasty of the sternal end of the muscle. There was no cosmetically unacceptable scar visible at either of the two surgical sites in any of the patients.
Statistically significant improvements in neck ROM, head tilt and facial asymmetry were seen postoperatively (Table 3; Figs. 1, 2, 3). Correlation analysis showed a significant positive correlation between preoperative neck ROM and final functional outcome, and between preoperative head tilt and final functional outcome (Table 4). However, age at presentation and facial asymmetry had no significant correlation with the final functional outcome (Table 4).
Comparative analysis of preoperative and postoperative neck ROM, head tilt and facial asymmetry
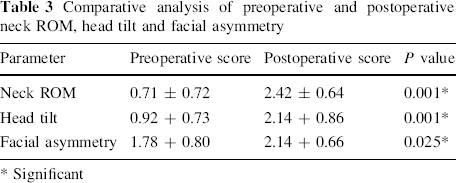
Significant
Spearman correlation analysis between age at presentation, preoperative neck ROM, preoperative head tilt and preoperative facial asymmetry
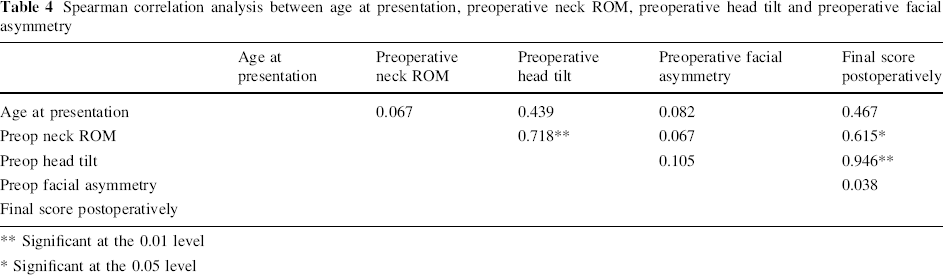
Significant at the 0.01 level
Significant at the 0.05 level

Preoperative picture of a 13-year-old girl with muscular torticollis to the right.
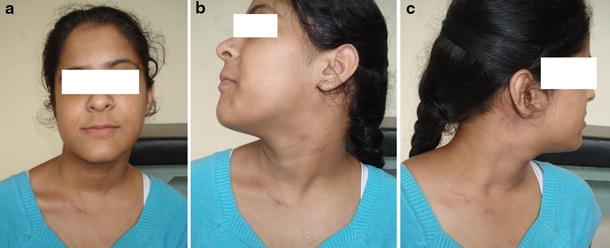
Six-week-postoperative picture of the girl from Fig. 1 after bipolar release and z-plasty of the sternal attachment of the sternomastoid. The V shape above the sternum is maintained.

Preoperative (
Discussion
Most cases of CMT resolve completely, either spontaneously within months after birth or following the early initiation of conservative measures such as gentle controlled passive manual stretching exercises on the affected side [5, 7]. Sonmez et al. found that 95% of the patients diagnosed and treated effectively before an age of one year did not need surgical treatment [11].
Conservative management is usually tried before an age of one year. Nonoperative therapy after the age of one year is rarely successful [12]. The goals of surgical correction for older children are improvement in cosmetic deformity and cervical motion. The timing of surgery is controversial. Reversal of the craniofacial asymmetry is best achieved at an early age, when there is high growth and remodeling potential. Canale et al. [12] reported that full recovery of facial asymmetry after four years of age is difficult to obtain. Characteristically, there is flattening of the occiput contralaterally and depression of the malar prominence ipsilaterally, with downward displacement of the ear, eye and mouth on the affected side. Provided that the surgery is done while the patient is immature, these skeletal deformities may improve following surgery [13].
Late presentation of congenital muscular torticollis is quite common in developing countries like India, where many female patients present with cosmetic concerns just prior to a planned wedding. Lee et al. [10] and Minamitani et al. [14] reported that late release of the sternocleidomastoid muscle for patients more than six years of age could yield acceptable results. In a group of patients over the age of 26, Ippolito and Tudisco [15] reported that, although there was no resolution in facial asymmetry, there was improvement in the neck movements of all patients, and there were no complications. In contrast, Coventry and Harris [16] reported that the upper limit for good results after surgery for muscular torticollis is twelve years. Ling [17] also maintains that the benefit of treatment is limited over the age of five, and that the complication rate is high.
In our study, we observed functional and cosmetic improvements in all the patients. Our results of bipolar release with z-plasty point indicate that good results can be obtained in patients treated late provided that optimum surgery and rehabilitation are carried out.
Although there are various surgical procedures for CMT, unipolar and bipolar release are the most popular. Subcutaneous tenotomy is not recommended, as it does not achieve adequate release, while total resection of the sternocleidomastoid muscle—the most effective method in older children—carries the significant risk of injuring the spinal accessory nerve. Bipolar releases are usually used in older children with a severe deformity. Wirth et al. [18], in a review of 55 patients with an average follow-up of fifteen years after surgical release, recommended that biterminal release should be performed at the age of 3–5 years in all patients who do not respond to nonoperative treatment. As advocated by Wirth et al., we also believe that bipolar release combined with z-plasty preserves the normal V contour of the sternocleidomastoid and ensures a better cosmetic outcome.
The postoperative immobilization protocol for congenital muscular torticollis is also controversial (Fig. 4). The various techniques utilized include traction, cast, halo vest and collar. In the initial days following surgery, the patient has a tendency to keep the head in its former position in order to reduce pain, and compliance with the prescribed exercises is poor. If the head remains in this position, the released structures will regain their former tightness. Gentle cervical traction given immediately postoperatively ensures sustained correction. Once postoperative pain subsides, the patient can be shifted to a collar, and an exercise protocol can be initiated to ensure a satisfactory outcome. We ensured strict adherence to our postoperative protocol in all patients by providing regular follow-up and motivation to ensure a uniformly good outcome. Though our study does not establish improved outcomes with cervical traction, we strongly believe that postoperative traction and strict adherance to physiotherapy protocol play important roles in helping the patient to overcome the abnormally adjusted position of the head and neck.

Postoperative immobilization techniques:
Facial asymmetry is the most significant factor affecting the cosmetic outcome. We obtained improvements in facial asymmetry in most of our patients. However, the extent of the improvement varied. We also found that the perception of facial asymmetry decreased markedly in the immediate postoperative period, indicating that whatever the bony changes that occur, they usually look compounded by the abnormal soft tissue structures. We believe that surgical bipolar sectioning of the sternocleidomastoid muscle should be considered even in adults with irreversible facial and skeletal deformities. The surgery restores the range of neck motion and resolves the head tilt; it can therefore improve quality of life.
From our correlation analysis we found that a greater restriction in neck ROM and a more severe head tilt (as seen preoperatively) were associated with a poorer final outcome. This finding is expected, but it should be noted that our results do not contraindicate surgery in such patients. However, there was no correlation between age of the patient or preoperative facial asymmetry and the final outcome. Thus, we believe that surgery should be performed in all cases of congenital muscular torticollis, however old the patient may be at presentation, and however severe the facial asymmetry.
One potential limitation of our study was the subjectivity involved in measuring the preoperative and postoperative variables, such as head tilt, neck ROM, facial asymmetry, scar, etc. We also didn't attempt to measure interobserver variability in the measurement, which is a potential drawback of this study.
To conclude, we believe that bipolar release is a very viable option for correcting neglected congenital muscular torticollis. The procedure is much more effective than unipolar release or subcutaneous tenotomy, and is relatively complication-free and safe when compared to total resection of the sternocleidomastoid muscle. Lengthening of the sternal head by z-plasty restores the V shape of the base of the neck, which adds to the cosmesis, especially in a female patient. Postoperative head halter traction and a well-planned physiotherapy protocol go a long way toward ensuring good to excellent results.