
Abstract
Purpose
The spontaneous recovery rate of neonatal brachial plexus palsy (NBPP) is often cited as 75–95%. However, recent reports have found the recovery rate to be much lower. The purpose of this study was to perform an evidence-based review aimed at summarizing the available English language information regarding prognosis following NBPP based on the Narakas classification.
Methods
A Medline database search was performed to identify articles that focused on the natural history, outcome, prognosis, or conservative treatment of neonatal brachial plexus birth injury from 1966 to 2006. Twenty-four articles were identified. The articles were graded according to the Oxford Evidence Based Grading Scale and data regarding sample size, follow up, study purpose, Narakas grouping, Mallet scale, and recovery of function at 3 and 6 months were extracted. Of the 24 articles, 11 were included for review. Data analysis included odds ratios and percent recovery.
Results
Of the 11 studies, only one was given a grade of a Level I study, three were given a grade of Level II, and seven were given a grade of Level IV. Sixty-four percent of infants classified as Narakas I and II had spontaneous recovery of biceps function at 3 months of age and only 9% of the Narakas III and IV group had recovery. Sixty-five percent of the Narakas I and II group had complete recovery at 6 months of age and only 14% of the Narakas III and IV group had recovery. The odds of biceps recovery at 3 months of age for the Narakas I and II group was 19 times higher compared to the III and IV group. The odds of complete recovery were 11 times higher for the Narakas I and II group compared to the III and IV group.
Conclusion
The quality of the literature regarding the prognosis of neonatal brachial plexus injury is poor. Based on the Narakas classification, recovery better for NBPP classified as Narakas I and II.
Introduction
The incidence of neonatal brachial plexus palsy (NBPP) is 1.51 per 1,000 live births in the United States [1]. The literature typically cites spontaneous recovery as 75–95% for NBPP [2–5]. However, more recent reports have indicated that only about two-thirds of infants have spontaneously recovery [6–8].
Beginning at 3 weeks of age, the severity of an infant's NBPP can be characterized by the Narakas classification [9]. This classification system categorizes NBPP from I to IV. Narakas I is the least severe and is a palsy limited to the nerve roots C5 and C6 in the upper trunk. This is the most common type of NBPP, making up approximately 73% of all NBPP [10]. Narakas II is an injury to nerve roots C5, C6, and C7. Narakas III is a global palsy effecting nerves C5, C6, C7, C8, and T1. Narakas IV is the most severe and is a global palsy that is characterized as a flaccid arm with or without Horner's syndrome. Approximately 25% of palsies are global (i.e., Narakas III or IV) [10]. By utilizing this classification scheme, a prognosis for recovery may be determined.
The purpose of this study was to perform an evidence-based review aimed at summarizing the available English language information regarding the prognosis of NBPP using the Narakas classification.
Methods
We conducted a search of the English language literature that focused on the natural history, outcome, prognosis, or conservative treatment of neonatal brachial plexus birth injury from 1966 to 2006. The Medline computerized database was utilized to search the following key words: (1) brachial plexus neuropathy (489 total hits, three studies identified); (2) brachial plexus and neonatal (92 total hits, three studies identified); (3) brachial plexus and newborn (85 total hits, five studies identified); (4) paralysis and obstetric (219 total hits, 12 studies identified); (5) brachial plexus birth palsy and prognosis (two total hits, one study identified). Following a review of the article title and/or abstract, 24 studies were identified and underwent further analysis by two separate reviewers. Articles were graded according to the Oxford Evidence Based Grading Scale (Table 1). Information regarding sample size, length of follow up, study purpose, Narakas grouping, Mallet scale, and recovery of function at 3 and 6 months were extracted from the articles. Following the review of the articles, 13 were excluded due to the lack of outcome data and 11 were included for analysis. Data analysis included percent recovery and odds ratios.
The Oxford Evidence Based Grading Scale
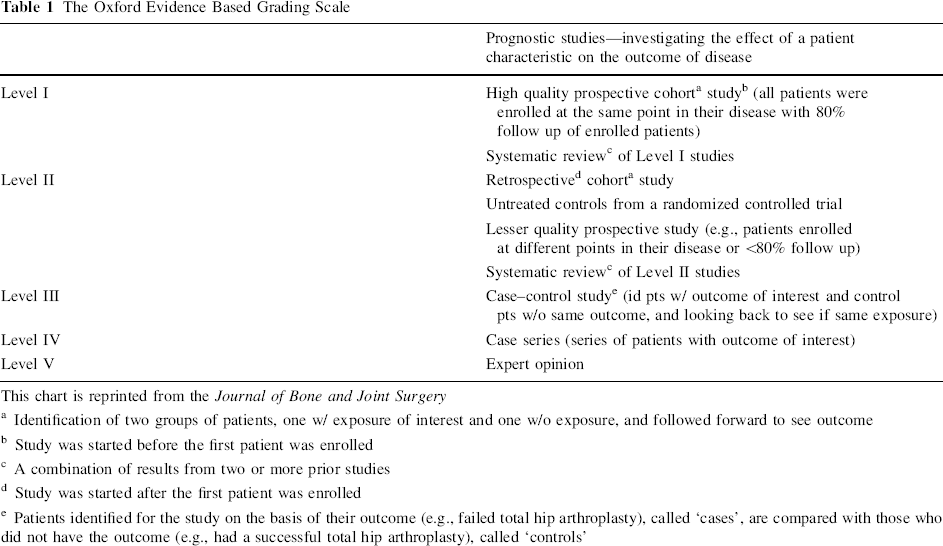
This chart is reprinted from the Journal of Bone and Joint Surgery
Identification of two groups of patients, one w/ exposure of interest and one w/o exposure, and followed forward to see outcome
Study was started before the first patient was enrolled
A combination of results from two or more prior studies
Study was started after the first patient was enrolled
Patients identified for the study on the basis of their outcome (e.g., failed total hip arthroplasty), called ‘cases’, are compared with those who did not have the outcome (e.g., had a successful total hip arthroplasty), called ‘controls’
This study (#06-10-21) was reviewed by the Cincinnati Children's Hospital Institutional Review Board and was granted exemption from review due to the nature of the study material.
Results
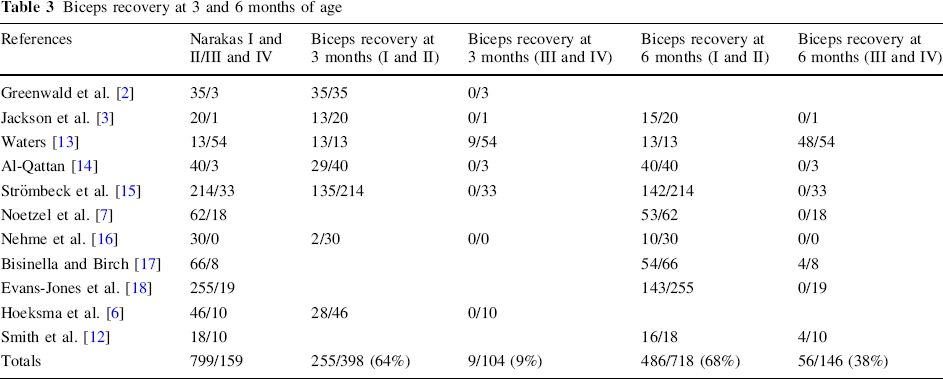
According to the Oxford Evidence Based Grading Scale, one study (9%) was given a rating of a Level I prospective cohort study, three studies (27%) were rated a Level II retrospective cohort study, and the remaining seven studies (64%) were rated a Level IV case series study (Table 2). Table 3 illustrates biceps recovery at 3 and 6 months of age. Of the Narakas I and II group, 255 (64%) patients showed biceps recovery at 3 months of age and only nine (9%) patients of the Narakas III and IV group (III and IV) showed recovery. Four hundred and eighty-six (68%) cases of group I and II had biceps recovery at 6 months of age and only 56 (38%) of group III and IV had recovery. Table 4 shows complete recovery at 3 and 6 months of age. Of group I and II, only 50 (59%) patients had complete recovery at 3 months of age and 291 (65%) at 6 months of age. None (0%) of the cases in group III and IV showed complete recovery at 3 months of age and only eight (14%) had complete recovery at 6 months of age.
Characteristics of the included studies
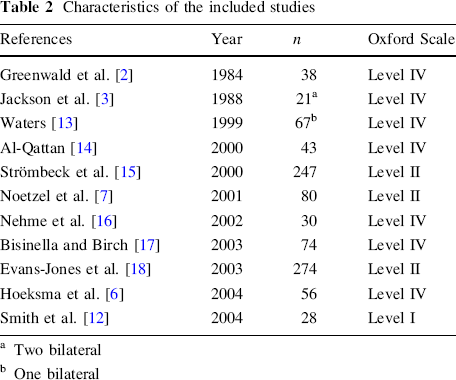
Two bilateral
One bilateral
Biceps recovery at 3 and 6 months of age
Complete recovery at 3 and 6 months of age
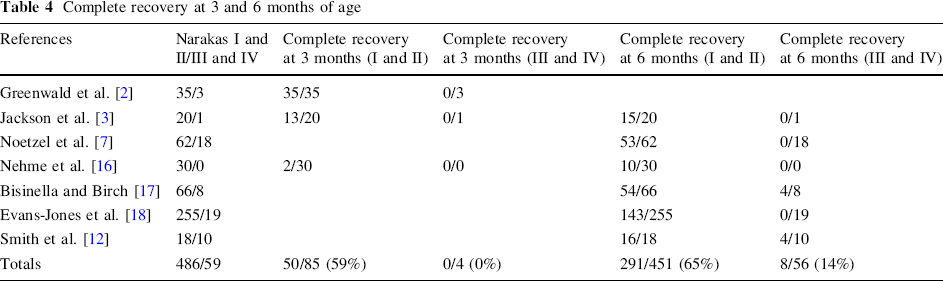
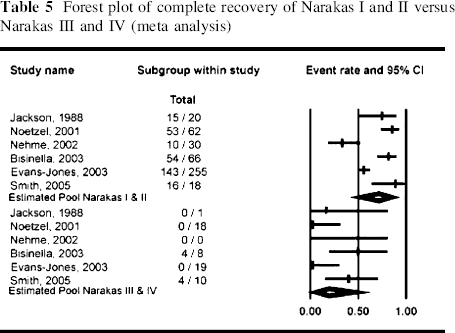
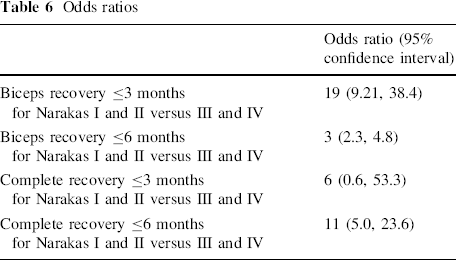
Table 5 is a forest plot illustrating complete recovery at 6 months of age for group I and II versus group III and IV. The spontaneous recovery rate favors group I and II compared to group III and IV. Table 6 shows the odds ratios for biceps and complete recovery. The odds of biceps recovery at 3 months of age was 19 times higher for group I and II compared to group III and IV. The odds of complete recovery at 6 months of age was 11 times higher for group I and II compared to group III and IV. The confidence intervals for these odds ratios are wide due to the small sample size, but are still indicative of a statistically significant association.
Forest plot of complete recovery of Narakas I and II versus Narakas III and IV (meta analysis)
Odds ratios
Discussion
There are a number of studies that have evaluated neurological and biceps recovery in NBPP patients. Hoeksma et al. [6] evaluated 56 children with NBPP that were born at the Academic Medical Centre, Amsterdam, the Netherlands, between 1991 and 1998. Thirty-seven (66%) children recovered within the first 6 months and 19 (34%) did not achieve full neurologic recovery [6]. Full neurologic recovery was defined as normal muscle strength in all muscle groups and incomplete recovery was defined as a loss in strength in any muscle group [6].
Another study by Noetzel et al. [7] examined 80 infants and found that 53 (66%) achieved complete recovery. Nine had mild weakness, seven had moderate weakness, and three had severe weakness [7]. Complete recovery was defined as antigravity movement in the biceps, triceps, and deltoid muscles by 4.5 months of age and severe weakness was defined as a lack of antigravity movement at the shoulder and elbow [7].
In the meta-analysis by Pondaag et al. [8], the authors examined all articles in English, French, German, or Dutch that made reference to the incidence, natural history, or outcome of NBPP. These authors identified over 1,000 articles, but further screening reduced the number of articles to 42 [8]. Articles to be included in this study required: a prospective study design, a study population based on demographics, a minimum follow up of 3 years, and an outcome assessment [8]. None (0%) of the studies which these authors identified met all four criteria and only seven (17%) met at least two criteria [8]. Of the seven that were identified, the recovery rate ranged from 7 to 90% [8]. Also, two of the seven (29%) studies were considered to be the most ‘ideal’ due to the nature of their study design, study population, length of follow up, and assessment of the end-point.
The study by Jackson et al. [3] examined all infants born at the University of California at Irvine Medical Center between July 1983 and December 1986, and identified 21 children with 23 palsies. Two patients were lost to follow up, but at the last check at 2 days and 5 months, these children had not recovered completely [3]. Of the remaining 19 palsies, 18 were classified as group I and II and only one was a classified as group III and IV [3]. Thirteen out of 19 palsies (68%) recovered by 6 months of age. The only palsy classified as group III and IV did not recover [3]. Patients had a minimum follow up of 1 year and a maximum follow up of 4 years [3]. However, this study was limited by the nature of its design. It was a hospital-based study and thus, was prone to referral bias.
The study by Sjöberg et al. [11] examined all children born in Malmo, Sweden, from 1973 to 1982. Forty-eight children were identified with NBPP [11]. Thirteen (27%) of these children had permanent sequela and four (8%) were considered to be ‘almost well’ by 12–18 months of age [11]. Forty-six children (96%) were classified into group I and II and two children (4%) were classified as group III and IV [11]. Both children in group III and IV were found to have permanent disability [11]. Of those with NBPP, 73% recovered and, if the ‘almost recovered’ children were included as part of the permanent palsies, only 65% showed complete recovery [11]. However, this study was limited as well. Its study population was not selected in any methodological fashion. Inflow and outflow of the population was restricted to a minimum [11]. This minimum length of follow up was complete recovery and the maximum follow up was 3–12 years [11].
In the current study, we identified over 800 articles in our Medline search and only 11 met our inclusion criteria. One of these 11 studies was identified as being a prospective study, with the remaining studies categorized as retrospective and case series [12]. The findings in the current study are similar to those found in Pondaag et al.'s meta-analysis, in terms of the quality and number of articles included in the study. Pondaag et al. [8] concluded that the quality of the literature is poor and the often cited excellent prognosis is based on studies that do not have the ‘width of scope’ to support these findings. Our results indicate that 64% of group I and II have spontaneous recovery of biceps function at 3 months of age. The odds of recovery are 19 times higher for group I and II compared to group III and IV. These results support the conclusions of the studies conducted by Hoeksma et al. [6], Noetzel et al. [7], and Pondaag et al. [8], who found their recovery rates to be near 66%.
Limitations within our study must be acknowledged. A sample size of 11 is small, yet it is consistent with other studies in the literature that had similar inclusion criteria. Also, only one of the 11 (9%) studies included in our analysis was prospective with a small sample size. The remaining studies were retrospective case series and were considered to be less reliable, since they are often prone to information and recall bias.
From our results, we can conclude that the previously reported spontaneous recovery rate of 75–95% appears to be overly optimistic. The recovery rate is better for Narakas I and II compared to Narakas III and IV. We advise physicians to be careful when reporting recovery rates and children with NBPP should seek additional treatment to help avoid long-term disability.
Footnotes
Acknowledgments
Internal departmental funds were utilized to support this research.