
Abstract
Abstract
Background
Previous studies report that children above the 95th percentile in weight for their age had an increased risk for complications following titanium elastic nailing for femur fractures. The purpose of this study is to examine whether obesity, defined as body mass index (BMI) > 95th percentile, and/or simple weight correlates with an increased rate of complications.
Methods
The incidence of complications was compared between obese and non-obese patients and also between patients who weighed ≥50 kg and those <50 kg.
Results
The overall complication rate was 23% (16/71). The complication rate was 17% (10/58) for “non-obese” patients and 46% (6/13) for “obese” patients. This difference was statistically significant (P = 0.03). The complication rate was 46% (6/13) in children who weighed ≥50 kg and 17% (10/58) in children who weighed <50 kg. This difference was also statistically significant (P = 0.03).
Conclusions
This study demonstrates that obesity (BMI > 95th percentile) and weight over 50 kg predispose patients to increased risk of surgical complications when undergoing flexible elastic nailing for femur fractures. Both obese children and children weighing ≥50 kg were two times more likely to have a complication when undergoing this procedure.
Introduction
As the prevalence of childhood obesity garners increasing attention across the world, evidence for its deleterious effects on children's health continues to grow [1]. Nearly all organ systems are adversely affected by obesity. Orthopedic implications among obese children have also been reported [2, 3]. The majority of children suffering from slipped capital femoral epiphyses are obese (50–70%), as is the case with Blount's disease (as much as 80% of patients are obese) [4]. Obesity is also known to increase the risk of complications associated with many orthopedic surgeries among adults [4–8]. Specifically, complications associated with the operative treatment of femur fractures have been reported in the context of obesity among adults and children [2, 9]. Specifically, the increased risk of complications associated with the elastic nailing of femur fractures in obese children has been recently reported [2].
According to the Centers for Disease Control and Prevention (CDC), the recommended definition of obesity among children should be calculated using the body mass index (BMI). While adults, who have stopped growing, maintain relatively constant body fat percentages over the course of their lives, children's amount of body fat varies considerably according to their age and gender at the time of measurement. Therefore, to determine the weight status category of a child or teen, the CDC recommends using a BMI-for-age growth chart, where children who fall at or above the 95th percentile are “obese.”
The purpose of this study is to examine whether obesity, defined as BMI > 95th percentile, and/or weight correlates with an increased rate of complications after titanium elastic nailing for femur fractures in children.
Materials and methods
Internal review board (IRB) approval was obtained prior to the start of this retrospective chart review. A retrospective chart review was performed for all pediatric patients with diaphyseal femur fractures treated with flexible titanium intramedullary nails (Synthes, Paoli, PA, USA) at the authors’ institution from 1998 to 2003. For the current study, the patient height and weight were also collected from these charts. The BMI was then calculated. The data collected included age, height, and weight and complications. Surgery time, estimated blood loss, weight-bearing status, and brace use was also recorded and examined in relation to complications.
All surgeons were fellowship trained pediatric orthopedic surgeons with academic appointments at a level 1 pediatric trauma center, where all of the surgeries were performed. All patients received a general anesthetic. All nails were inserted distally to proximally.
Obesity was determined according to the CDC guidelines. The BMI was plotted on the CDC's age- and gender-specific percentile chart. Children who placed over the 95th percentile were considered “obese.” Those between the 85th and 95th percentiles were considered “at risk of obesity,” 5th to 85th as “healthy weight,” and those below the 5th percentile were considered “underweight.” The incidence of complications amongst obese patients was compared to the incidence of complications amongst non-obese patients using Fisher's exact test.
The incidence of complications was also compared among patients under 50 kg and those greater or equal to 50 kg.
The incidence of complications among patients ≥50 kg was also compared to those who weighed <50 kg using Fisher's exact test.
Inclusion criteria included surgery using titanium elastic nails for a femur fracture in a patient with open physes. Exclusion criteria included underlying neuromuscular disease, metabolic bone disorder, or pathologic fracture. Patients were also excluded if their age, height, and weight were not available to calculate their BMI.
Results
The charts of 94 patients were available for review. All data, including height and weight, was available for 71 patients.
The average age was 9 years and 3 months (range 4–15 years). There were 51 boys and 20 girls. Eight patients were “underweight,” or under the 5th percentile. Thirty-nine patients were of a “healthy weight,” or between the 5th and 85th percentiles. Eleven patients were “overweight,” or between the 85th and 95th percentiles. Thirteen patients were “obese,” or above the 95th percentile.
Thirteen patients weighed 50 kg or more. Four of these patients did not qualify as “overweight” or “obese,” as their BMIs were below the 85th percentile. Fifty-eight patients weighed less than 50 kg. Fifteen of these patients were “overweight” or “obese,” with BMI greater than the 85th percentile. Table 1 details patients by age, height, weight, BMI, and BMI percentile. This clarifies the difference between patients greater or equal to 50 kg and those defined as obese by their BMI.
Age, height, weight, body mass index (BMI), and complications
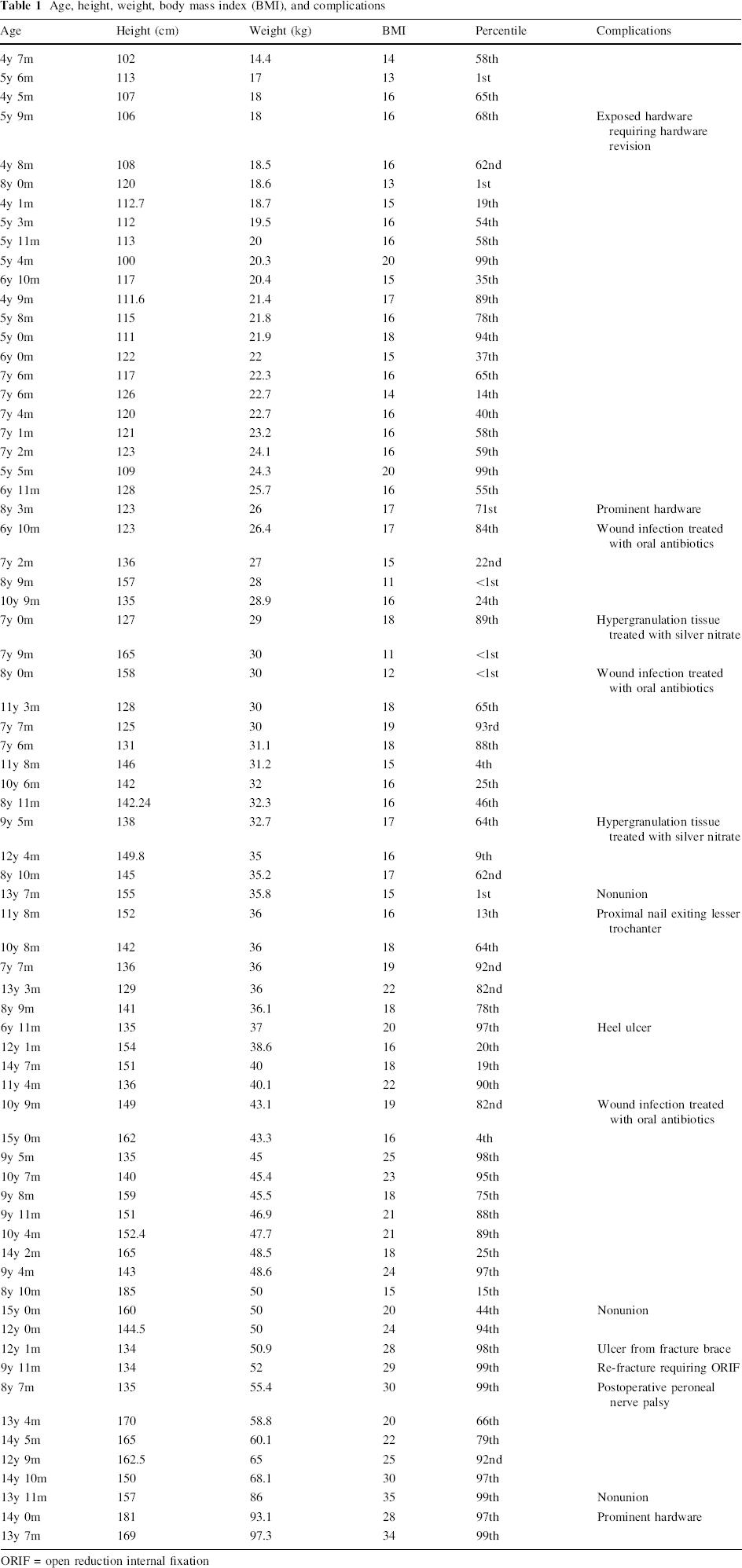
ORIF = open reduction internal fixation
Complications according to height, weight, and percentile are listed in Table 2. No patient had more than one complication.
Height, weight, BMI, and complications
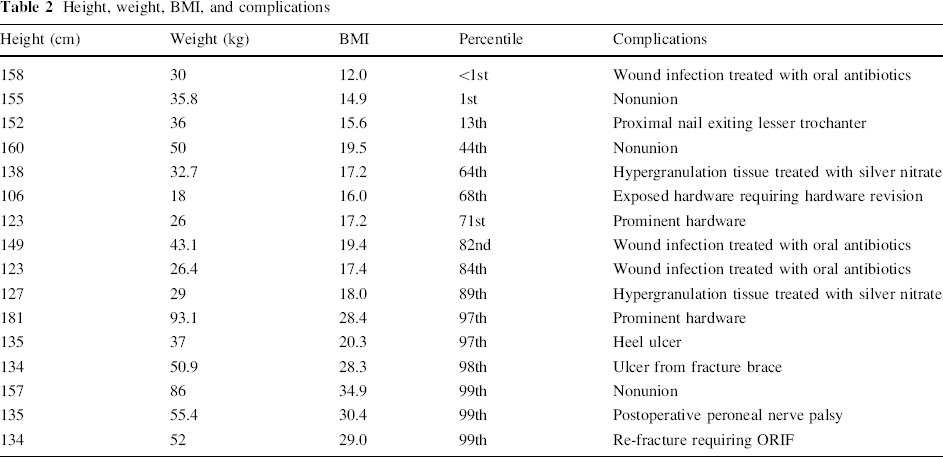
The heel ulcer, grade 1, was treated with wound care and by unloading the heel. The ulcer from the fracture brace was also grade 1 and healed after modifications were made to the brace.
The overall complication rate was 22.5% (16/71). There were ten complications among the 58 “non-obese” patients (17.2%) and six complications in the 13 “obese” patients (46.2%). When compared via Fisher's exact test, this difference was statistically significant (P = 0.03).
The complication rate among children who weigh ≥50 kg was 46.2% (6/13) compared with a 17.2% rate (10/58) for those <50 kg. This difference was statistically significant (P = 0.03).
Although there were six complications among children with a BMI over the 95th percentile and six complications among children greater than 50 kg, these two groups are similar but not identical. There is one child who was above the 95th percentile in BMI who weighed only 37 kg (he was only 6 years old), and one child who weighed 50 kg, but was only in the 44th percentile in BMI (he was 15 years old).
Five of the complications which occurred in the children with a BMI under the 95th percentile and in the children less than 50 kg were wound infections treated with oral antibiotics (three) and hypergranulation tissue treated with silver nitrate (two). These may be considered as “minor” complications. When considering “major” complications, the complication rate among non-obese children (BMI under the 95th percentile) is 8.6% (5/58). There were no “minor” complications in the obese patients or in the group of patients over 50 kg.
Surgery time ranged 28–150 min, averaging 67 min. Eight complications occurred in cases that lasted under an hour, and eight complications occurred in cases that lasted over an hour. Surgery time did not correlate with BMI.
Average blood loss was 44 cc. The estimated blood loss ranged from 5 to 400 cc. This did not correlate with BMI, weight, or complications.
Weight-bearing status was available for 68 of the 71 patients (96%). Forty-one patients (69%) were kept non-weight-bearing for 6 weeks, 13 patients (19%) were allowed to partially weight-bear for 6 weeks, and 14 patients (20%) were allowed to place weight on their leg as tolerated postoperatively. Thirteen of the 16 complications (81%) occurred among patients who were kept non-weight-bearing.
Brace and immobilization data was available for 67 of the 71 patients (94%). Postoperatively, four patients (6%) were placed in a cast, seven (10%) were placed in a fracture brace, 28 (42%) were placed in a knee immobilizer, and 28 (42%) received no external supportive devices. Eleven complications occurred among patients who received immobilization, while five occurred among patients who were not immobilized.
All three patients who had nonunions of their fractures were kept non-weight-bearing and were placed in a knee immobilizer postoperatively.
Discussion
Obesity is a rampant problem among children around the world. Obese patients are more likely to have medical problems and complications related to orthopedic surgery. There is an increased incidence of elevated blood lipids, steatohepatitis, and cholelithiasis in obese children [4, 10]. Obese children show a predisposition to increased glucose tolerance and contribute significantly to the rising number of noninsulin-dependent diabetes mellitus diagnoses [10]. It has been reported that nearly a third of obese children suffer from hypertension, which, when coupled with elevated blood lipids, places these children at risk for coronary heart disease [10]. It has also been reported that obese children suffer more often from sleep apnea and, possibly, a related diminution of learning and memory function than their non-obese peers [4, 10]. Foran et al. [4, 10] have shown that obesity correlates with a worse outcome following total knee arthroplasty. Green et al. [5] have reported obesity to increase the risk of nonunion after humerus fractures in adults. The treatment of nonunions in obese patients has been shown to be fraught with complications [6]. Anesthesia risks also increase for obese children [11, 12].
Previous study of femur fractures treated with intramedullary elastic nails in children has suggested that larger children have a higher complication rate [2]. This study examined obesity by comparing patient weight to their age, not by calculating the BMI. This study may have defined children who are merely tall for their age as obese, and may have misidentified those who are short for their age as underweight.
Ho et al. [13] showed an increased risk of complications among older children who underwent titanium elastic nailing for femur fractures. The authors found that children over the age of 10 years had a greater risk of complications than those under the age of 10. They commented that the increased complication rate among the older children may be due to increased weight and size, but the previous study of this group of patients did not take BMI into consideration. Moroz et al. [14] demonstrated that children weighing greater than 50 kg are more likely to have a poor outcome following titanium elastic nailing of femur fractures. In addition, Wall et al. [15] found that the malunion rate was four times greater in association with titanium elastic nails as compared to stainless steel nails.
The data presented in this study is not sufficient to explain causality, only to point out the correlation that increased weight and obesity increased the complication rate after titanium elastic nailing for femur fractures in children. The majority of patients reported in this study were treated before the publication of the literature that has pointed out that heavier children have a higher incidence of complications using this construct. Hopefully, this study will help to prevent the future treatment of obese patients with flexible titanium elastic nails. A weakness of this study is that there is almost complete overlap of the group of complications among obese patients defined by BMI and patients over 50 kg. Surgeons should surely consider alternative fixation for femur fractures in patients who are both over 50 kg and greater than the 95th percentile in BMI.
This study is clearly weakened by its retrospective nature. For example, two patients were noted to have prominent hardware. For many patients treated with flexible intramedullary nails, the ends of the rods are palpable. Because this is a retrospective review, it is difficult to determine whether there were additional patients who had prominent hardware that was not recorded in the clinic charts.
This study demonstrates that obesity and weight ≥50 kg predispose patients to increased risk of surgical complications when undergoing flexible elastic nailing for femur fractures. Obese children were twice as likely to have a complication when undergoing this procedure, as were patients ≥50 kg. Families should be informed of the increased risks in these patient groups. These findings have prompted the authors to consider alternative surgical techniques for the treatment of femur fractures in older, larger children.