
Abstract
Abstract
Purpose
Acute tibial tubercle avulsion fractures typically occur in adolescent boys involved in certain sports. All of the excerpted authors recommend open reduction and internal fixation (ORIF) as the only method to manage the displaced form of the injury. We attempted to select the optimal medical treatment of various types of this injury. The closed reduction and internal fixation (CRIF) method was selectively used.
Methods
During a period of 10 years (1997–2006), we treated 12 children with an acute injury to the tibial tubercle. Ogden's classification was used to describe the type of injury. Nine patients with a displaced fracture were treated surgically, using either the CRIF or ORIF methods. In cases of intraarticular fracture, the use of the CRIF method was tested. The suitability of the CRIF method was decided during manipulation of the fragments under an X-ray amplifier.
Results
According to Ogden's classification, three children were classified with type 1A, one with 1B, three with 2A, four with 3A, and one with 3B. In patients with the displaced extraarticular injury (types 1B and 2A), the ORIF method of treatment was necessary. In all but one case of intraarticular fracture (type 3A and 3B), the CRIF method was sufficient.
Conclusions
The authors recommend that, for displaced intraarticular Ogden's type 3A or 3B fracture, the CRIF method should be considered as a first choice.
Introduction
Acute tibial tubercle avulsion fractures are uncommon. These injuries typically occur in adolescent boys involved in certain sports. It mainly happens by a strong quadriceps contraction during knee extension or by a rapid passive flexion of the knee against the contracting quadriceps [1].
The tibial tubercle develops postnatally, primarily as a structural modification of the anterior portion of the proximal tibial epiphysis [2, 3]. Ehrenborg and Lagergren [4] divided tibial tubercle development into four stages: cartilaginous, apophyseal, epiphyseal, and bony. Ogden et al. [2, 3] described three histological zones in the tibial tubercle growth plate. There is a progressive change from fibrocartilage to columnar cartilage from proximal to distal just before physiologic epiphysiodesis. The physiologic epiphysiodesis occurs in the same direction. These changes predispose to avulsion injury of the tibial tubercle just before or during the later stages of physiologic epiphysiodesis [5].
Materials and methods
A retrospective analysis of patients treated in the period 1997–2006 at the Regional Pediatric Trauma Center, Thomayer Teaching Hospital, Prague, Czech Republic, was performed. We found 101 cases of children of all ages with proximal tibial (epi)physeal injury. Of these, 12 (11.8%) were acute tibial tubercle avulsion fractures in adolescents, which means that 0.26% of all physeal injuries of children of all ages were treated at our institute during the tested period. Plane radiographs were used to confirm the diagnosis.
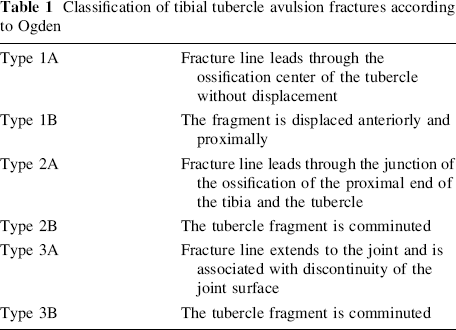
The fractures were classified according to Ogden′s schedule (Table 1).
Classification of tibial tubercle avulsion fractures according to Ogden
This study considered the age of children, sex, mechanism of injury, clinical signs, radiographs, method of treatment, and follow-up. The follow-up was for the duration of 1 year.
Results
All 12 patients were adolescents. The mean age at the time of injury was 14 years 6 months, with a range from 12 years 3 months to 16 years 10 months. All but one were boys. Eleven patients (all boys) were injured during sports (seven soccer players and four athletes, either high or long jumpers). The only girl in the study was injured during rapid walking. Only one patient had symptoms suggestive of Osgood-Schlatter's disease (OSD) before the injury. All patients expressed complaints of pain and experienced swelling over the tibial tubercle at the first examination. The patients with displaced injury (nine of the 12 cases) were not able to walk. Three quarters of the cases (eight of the 12) occurred on the right leg. None of the injuries were compound fractures.
The lateral radiograph confirmed the diagnosis in all cases. There were three patients with type 1A, one of type 1B, three of type 2A, four of type 3A, and one of type 3B, according to Ogden's classification. No case of type 2B occurred in our cohort.
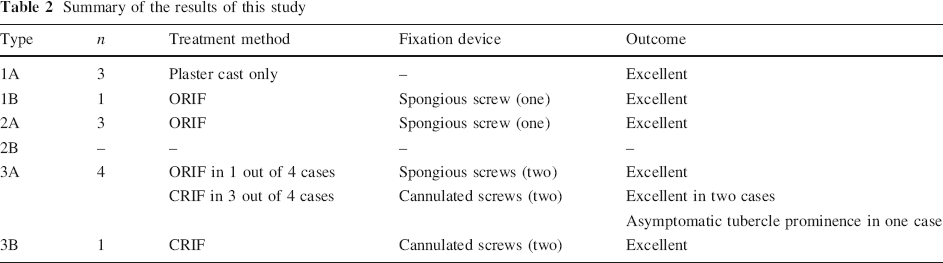
Three patients with an undisplaced form of the injury (type 1A) were treated nonoperatively by plaster casting for 4 weeks. All were healed without sequels.
Four patients with displaced extraarticular form of the injury (types 1B and 2A) were treated by the open reduction and internal fixation (ORIF) method using one spongious screw and then plaster casting for a 4-week period. All healed without any complications and with a full range of movement (ROM).
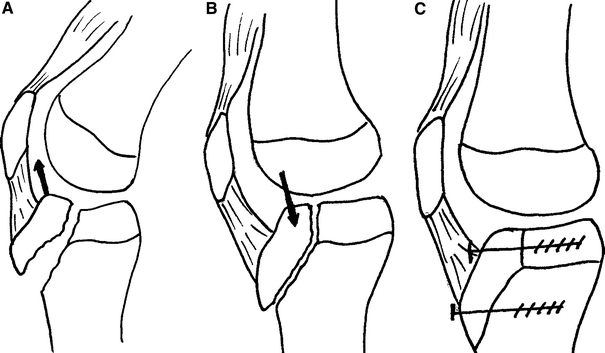
Four of the five patients with displaced intraarticular form of the injury (types 3A or 3B) were treated by the closed reduction and internal fixation (CRIF) method using two cannulated screws and plaster casting for 4 weeks (Fig. 1a, b). In all of these cases, the closed reduction by hyperextension of the knee joint forced accurate positioning of the fragments with fully articular surface congruence. The straight pressure of the femoral condyle against the displaced fragment of the tibial tubercle made the accurate reduction possible (Fig. 2a–c). The last of the five cases was treated by the ORIF method using two spongious screws. In these cases, the periosteal flap interposition restrained the fragments of the tibial tubercle from adequate reduction. All of these patients were healed without any limitation of the ROM, the same as in previous cases of the cohort. The only sequel within the cohort was a painless hypertrophy of the tibial tubercle in the case of one boy treated by the CRIF method (Table 2).

Summary of the results of this study
Discussion
DeMorgan should be given the credit for the first case describing this adolescent injury, reported in 1853 [6]. Poland [7], in 1898, published a description of a case of ten male adolescents’ injuries; nine of them were caused by violent muscular action of the quadriceps during the sporting activity. The inability of the patient to extend their leg at the knee joint from the time of the accident was a prominent clinical sign. Poland gave a notice of an erroneous diagnosis of the patellar fracture in three patients, in which the ORIF of the tibial tubercle fragment was performed using a pin. The other cases were treated by closed reduction of the tibial tubercle fragment, which was held in its position by strapping or by the use of a bandage of plaster of Paris. Only one of the ten patients healed with a poor result.
Later, a number of authors presented their cohorts, classification schedules, or studies of postnatal skeletal development of the tibial tubercle. In all of these works, the sporting activity was identified as the most frequent cause of the injury, and in almost all cases, the children afflicted were boys. The age ranged from 9 to 17 years [1, 5, 6, 8, 9]. These data are in agreement with our findings. The Ogden's classification, which is a modification of the former Watson-Jones’ classification, is mostly used for classifying these injuries. Ryu and Debenham [10] added a type 4 to describe an avulsion fracture of the entire proximal tibial epiphysis. We do not consider this type of injury as a tibial tubercle injury, but as a separation of the entire proximal tibial epiphysis. Frankl et al. [11] suggested an addition of the type 1C for fractures with an associated avulsion of the patellar tendon. McKoy and Stanitski [1] proposed to add a type 5. According to them, type 5 is the Ogden type 3B combined with a type Salter-Harris IV fracture of the proximal tibia, forming a “Y” configuration. The latter two types (1C and 5) did not occur during our research period.
OSD is suggested by Ogden et al. [9] to be a possible predisposing cause of the acute tibial tubercle injury. He presented nine patients with pre-existing OSD from the series of 14 acute injuries. Seven of them involved the contralateral knee and there was no evidence of similar involvement of the side of an acute injury. Bolesta and Fitch presented four patients with OSD from the series of 16 patients with an acute tibial tubercle injury [6], Mosier and Stanitski two of 19 [5], and Chow et al. mentioned only one patient from 16 [8]. In our study, there was only one patient with preexisting OSD from the 12 acute injury cases.
All of the excerpted authors recommend ORIF as the only method to manage the displaced form of the tibial tubercle injury [1, 5, 6, 8, 9, 12, 13]. The method of osteosynthesis varies from tension band in younger children to screws in older cases. In our material, we used the ORIF method in cases where we could not achieve accurate positioning of the fragments by closed reduction. This was because of the large displacement of a small fragment of the tubercle and/or when the interpositioning of surrounding soft tissue into the fracture line occurred. This means that we used the ORIF method in the following cases: (a) in all displaced extraarticular injuries of types 1B and 2A; (b) in the case of one of the five patients with intraarticular type 3A or 3B. For the remaining four patients, the method of closed reduction by hyperextension of the knee joint was successful. The accurate positioning of the fragments with fully articular surface congruence was established. In these cases, the fragments were stabilized by two cannulated screws inserted in parallel percutaneously. This method was fully sufficient for fracture management.
Bolesta and Fitch [6], Frankl et al. [11], and Mosier and Stanitski [5] presented some additional injuries associated with the tibial tubercle fracture; patellar ligament detachment or peripheral tears of the lateral meniscus. In our series, we did not find such injuries in patients treated by the ORIF method, and no consecutive problems with the knee joint occurred in our series during the follow-up.
Only sporadic cases of compartment syndrome as a complication of the acute tibial tubercle fracture were mentioned in the literature [1]. In our study, no patient with compartment syndrome occurred.
Sequels following acute tibial tubercle avulsion fractures are rare in the reported series. There is a hypothesis of genu recurvatum in patients under 11 years of age because of premature closure of the anterior physis, but no such a case has been reported in a previously normal patient [1]. Other sequels reported in the literature include malunion, nonunion, fracture through a fixation device, saphenous nerve neuroma [6], prominent tubercle, pain on squatting, numb below tuberosity or posterior cruciate laxity [8], leg length discrepancy, or deep venous thrombosis [9]. In a follow-up of our series of all 12 cases, only one patient suffered from a prominent tibial tubercle, but it was asymptomatic. This patient was one of the four treated by the CRIF method.
Conclusion
In cases of displaced intraarticular tibial tubercle fracture (types 3A and 3B), closed reduction should be attempted first. If the correct fragment positioning is achieved, the closed reduction and internal fixation (CRIF) method should be considered as a first choice. In any other case, the open reduction and internal fixation (ORIF) method is fully indicated.
Footnotes
Acknowledgments
This study was supported by a grant from the Czech Ministry of Healthcare IGA no. 9132-3/2007.