
Abstract
Purpose
Release of the psoas tendon for flexion deformity of the hip in children with cerebral palsy has traditionally been performed at the pelvic brim, lateral to the neurovascular bundle, or at its insertion into the lesser trochanter. As the psoas tendon is lateral to the pectineus, the traditional exposure of the tendon through an approach medial to the pectineus is limited by the extent to which the pectineus can be retracted proximally.
Technical note
We describe the use of the anteromedial approach used for the developmentally dislocated hip to expose the psoas tendon between the pectineus and the neurovascular bundle. This provides a much better visualisation of the tendon as it crosses the superior pubic ramus to its insertion. The use of this approach has not been described in cerebral palsy.
Introduction
Flexion deformities of the hip in children with cerebral palsy often lead to excessive anterior pelvic tilt, increased lordosis, hip subluxation and dislocation [1]. Several soft-tissue surgeries, such as psoas tenotomy, lengthening and muscle recession, have been described to address this problem [1–4]. The psoas tendon is commonly accessed at two sites: the pelvic brim and at its insertion into the lesser trochanter. Exposure at the pelvic brim, as described by Sutherland et al., is the preferred approach, as recession or lengthening at this level leads to less hip flexor weakness [2, 3]. This approach involves the exposure and retraction of the neurovascular bundle at the pelvic brim [2]. When there is an associated adduction deformity, an additional incision at the groin or a long incision across the groin is required to release the adductors. Other surgeons prefer the medial approach, as described by Ludloff [5], to expose the psoas tendon between the pectineus and the adductor brevis. Tenotomy or muscle recession of the psoas is performed near its insertion [1]. As the psoas tendon is lateral to the pectineus, adequate exposure of the tendon through an approach medial to the pectineus is difficult. The proximal extent of exposure is hindered by the extent to which the pectineus can be stretched and retracted proximally (Fig. 1). We describe an approach to the psoas tendon which combines the advantages of a single incision for the adductor and psoas release: good exposure near the pelvic brim and the ease of performance.
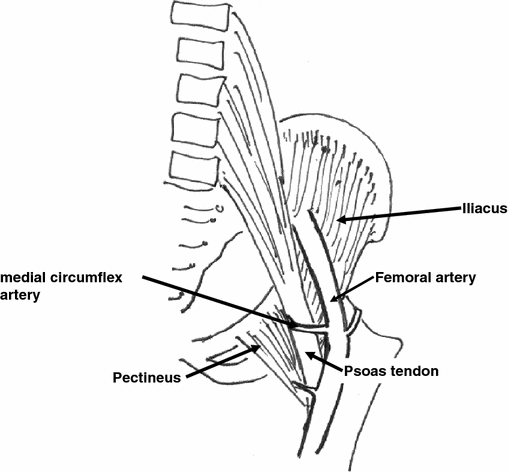
Exposure of the psoas tendon through an approach medial to the pectineus muscle is limited by the extent to which the pectineus can be retracted laterally and proximally
Surgical approach
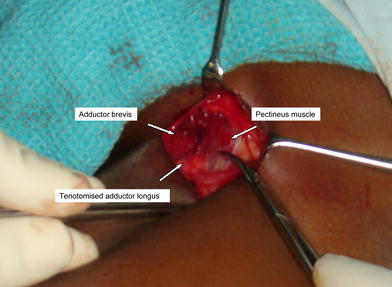
Surgery is performed with the patient in the supine position. A 2–3-cm incision is made just distal to the groin crease, with one third of the incision medial to the taut adductor longus tendon (Fig. 2). The adductor longus is identified and divided close to its origin. The gracilis is identified medially as a thin sheet near its origin and then divided. The pectineus is then identified lateral to the adductor brevis and the fascia overlying the pectineus muscle is divided longitudinally to expose the muscle (Fig. 3). It is essential that the plane of dissection be under the fascia overlying the pectineus muscle, otherwise, the definition of planes becomes indistinct as one dissects lateral to the pectineus. The plane between the pectineus (medially) and the neurovascular bundle (laterally) is developed using blunt dissection with a small gauze ball held at the tip of an artery clamp. Flexing and rotating the hip externally help identify the psoas tendon at its insertion into the lesser trochanter. A wad of connective tissue fat is commonly found overlying the psoas tendon. The fat is dissected off the psoas sheath using blunt dissection and the tendon is exposed to its insertion (Fig. 4). As the pectineus is retracted medially, the psoas tendon can be exposed proximally over the hip joint. The head of the femur can be palpated in this region when the limb is rotated and the psoas tendon can be traced proximally as it crosses the anterior capsule of the hip and on to the pubis. Care must be taken to not injure the medial femoral circumflex artery, which traverses the operative field (Fig. 1). If exposure is compromised as a result of the inability to retract the vessel proximally, it can be ligated. Once the tendon is exposed adequately, the sheath is split and the tendon is separated from the iliacus muscle proximally. Musculotendinous recession is carried out at this level if desired. If division near the insertion is preferred, the cut end can be sutured onto the anterior capsule of the hip, as described by Bleck [1]. Alternatively, the tendon can be lengthened at this site over the hip capsule [3]. A drain is usually not required post-operatively, as bleeding is minimal. In our experience of this approach for musculotendinous recession of the psoas and adductor tenotomy in 25 patients with cerebral palsy, we have not encountered any complications during the procedure.
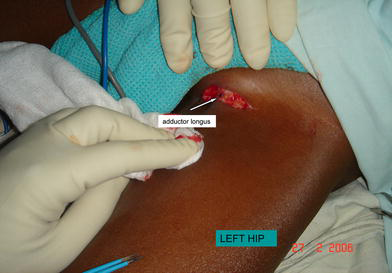
A 2–3-cm incision is made over the taut adductor longus tendon, just distal to the groin crease
As the interval between the pectineus and the neurovascular bundle is defined, it is essential that the plane of dissection be under the fascia of the pectineus
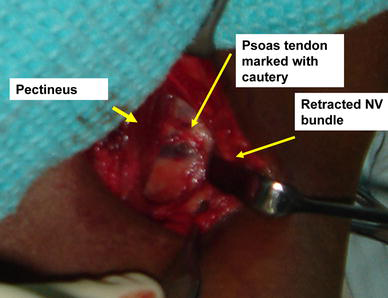
Retracting the pectineus medially and the neurovascular bundle laterally provides a good exposure of the psoas tendon
Discussion
Most surgeons consider the iliopsoas to be the primary cause for hip flexion deformities in ambulatory patients [2]. Treatments for flexion deformities have focussed on operations of the iliopsoas tendon. Division of the tendon at its insertion into the lesser trochanter is performed only in patients who require walking aids post-operatively [1, 2]. It is not performed in ambulatory patients, as it leads to the loss of power in the hip flexors, making it difficult for the patient to climb steps. The tendon is commonly approached between the pectineus and the adductor brevis [1]. The pectineus, which crosses the psoas tendon near its insertion, can be retracted proximally and laterally only to a certain extent, thus, limiting the exposure of the psoas tendon to its distal portion. Lengthening or musculotendinous recession of the tendon through this approach is difficult. For musculotendinous recession, the psoas tendon can be accessed at the pelvic brim, lateral to the neurovascular bundle [2, 3].
Once the psoas tendon is isolated using either of the approaches mentioned above, it is released using different techniques. Bleck divides the tendon near its insertion and sutures it onto the capsule [1]. Matsuo advocates controlled lengthening of the iliopsoas tendon between the inguinal ligament and its insertion [3]. As the psoas portion of the muscle complex is mostly directly related to the lordotic posture and pelvis alignment, it would be best to preserve all of the muscle fibres of the iliacus and lengthen or recess only the psoas element of the muscle complex [3]. This preserves the strength of the hip flexors and reduces the flexion deformity at the same time [3]. Sutherland et al. [2] advocates separation of the psoas tendon from the iliacus and division near the pelvic brim.
Weinstein [4] and Weinstein and Ponseti [7] described the anteromedial approach for the developmentally dislocated hip, in which they exposed the joint between the pectineus and the neurovascular bundle. This was a modification of the medial approach described by Ludloff [5] and popularised by Mau et al. [6], where the dislocated joint was exposed between the pectineus and the adductor brevis. Using the anteromedial approach, blood loss was minimal and visualisation was found to be excellent. The medial femoral circumflex vessel, which was found traversing the operating field, was often ligated when encountered. Eighteen of 20 patients required ligation of the vessel in their study [7]. Weinstein and Ponseti [7] and Morcuende et al. [8] found that ligation of the vessel did not result in a higher incidence of avascular necrosis compared to the other series. Excellent visualisation of the hip joint and the psoas tendon was possible using this approach [4]. We have used this approach in patients with cerebral palsy to gain a good exposure of the psoas tendon.
The purpose of this article is not to discuss the merits of division of the psoas tendon at different sites or the clinical outcomes of each procedure. The approach described above exposes the psoas tendon from its insertion to near the pelvic brim. It allows the psoas tendon to be dealt with by any of the preferred methods––lengthening, musculotendinous recession or tenotomy. To the best of our knowledge, this approach has not been described in cerebral palsy for psoas tendon exposure. It is simple and easy to perform. The fear of damaging the neurovascular bundle using this approach is unfounded, as there is no greater risk than the exposure at the pelvic brim, from the lateral to the neurovascular bundle. There is the additional advantage of utilising the same incision for the adductor tenotomy, which is often a concurrent procedure. The size of the incision remains small, unlike the approach described by Sutherland. We found the exposure of the psoas tendon to be superior to the conventional Ludloff medial approach, as the psoas tendon is better visualised when it is approached from lateral to the pectineus.
In conclusion, we recommend that this direct approach to the psoas tendon be used for patients with cerebral palsy, as it is safe, easy to perform and provides the surgeon with a good exposure of the tendon.