
Abstract
Background
Mindfulness- and acceptance-based interventions are increasingly studied as a potential treatment for a variety of mental conditions.
Objective
To assess the effects of mindfulness- and acceptance-based interventions on psychotic symptoms and hospitalization in patients with psychosis
Methods
MEDLINE/PubMed, Embase, the Cochrane Library, and PsycINFO were screened from inception through April 2015. Randomized controlled trials (RCTs) were analyzed when they assessed psychotic symptoms or hospitalization in patients with psychosis; affect, acceptance, mind-fulness, and safety were defined as secondary outcomes.
Results
Eight RCTs with a total of 434 patients comparing mindfulness-based (4 RCTs) or acceptance-based interventions (4 RCTs) to treatment as usual or attention control were included. Six RCTs had low risk of bias. Moderate evidence was found for short-term effects on total psychotic symptoms, positive symptoms, hospitalization rates, duration of hospitalization, and mindfulness and for long-term effects on total psychotic symptoms and duration of hospitalization. No evidence was found for effects on negative symptoms, affect, or acceptance. No serious adverse events were reported.
Conclusion
Mindfulness- and acceptance-based interventions can be recommended as an additional treatment for patients with psychosis.
Introduction
Psychotic disorders are severe mental conditions that typically manifest themselves mainly by positive symptoms (delusions and hallucinations) and negative symptoms (lack of motivation, reduction in spontaneous speech, and social withdrawal).1,2 These disorders are typically chronic in nature and often restrict quality of life and social function.3–5 Even when patients are compliant to psychopharmaceutical treatment, symptoms, especially negative symptoms, often persist,2,6 and about 30% of patients are therapy refractory. 7
Mindfulness- and acceptance-based interventions are increasingly studied as a potential treatment for a variety of physical8–11 and mental conditions.10,12,13 Despite conceptual differences between different acceptance- and mindfulness-based interventions, they share many theoretical underpinnings. These approaches do not try to alter the content of dysfunctional thoughts and symptoms but to alter the patients’ relationship towards these thoughts and symptoms. A mindful and accepting observation of every pleasant or unpleasant experience (including thoughts) in the present moment is intended.14,15 However, the specific techniques that are used to achieve this goal differ between different approaches. 13 Primarily mindfulness-based interventions like mindfulness-based cognitive therapy (MBCT) or mindfulness-based stress reduction (MBSR) that are more or less direct translations of Buddhist mindfulness traditions into Western medicine use formal mindfulness training like sitting or walking meditation as a main intervention.15,16 While MBSR has been originally designed as an intervention for chronic pain and stress-related symptoms, MBCT combines MBSR with cognitive-behavioral therapy and is normally led by a trained therapist.15,16 MBCT thus focuses more on a therapeutic approach rather than general stress reduction. 16 On the other hand, primarily acceptance-based interventions like acceptance and commitment therapy (ACT) or acceptance-based behavior therapy (ABBT) are multimodal approaches that have integrated cognitive interventions into a theoretical framework of mindfulness and acceptance and include shorter and more informal mindfulness exercise.13,14,17 Another major difference between primarily mindfulness-based and primarily acceptance-based intervention is that the former are mostly offered as group sessions 16 and the latter mostly as individual sessions. 14
As patients with psychotic disorders frequently engage in avoidance strategies like substance abuse or distraction—or on the other extreme, may become engrossed by their symptoms—mindfulness- and acceptance-based interventions have been proposed as approaches to alter the patients’ relationship towards their symptoms and hence reduce symptom-related distress. 18
The aim of this systematic review and meta-analysis was to investigate whether mindfulness- and acceptance-based interventions are effective and safe interventions for reducing psychotic symptoms and hospitalization in patients with psychosis.
Methods
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews and meta-analyses 19 and the recommendations of the Cochrane Collaboration 20 were followed.
Eligibility Criteria
Types of Studies
Randomized controlled trials (RCTs) were eligible. No language restrictions were applied.
Types of Participants
Adults with psychotic disorders (ie, schizophrenia, schizoaffective disorder, schizophreniform disorder, delusional disorder, brief psychotic disorder, and psychotic disorder not otherwise specified) were eligible if they were diagnosed by
the Diagnostic and Statistical Manual, 4th Edition, Revised (DSM-IVR), 1 the Research Diagnostic Criteria (RDC), 21 or the International Classification of Disease 22 (ICD) 22 ;
any other clinician-based diagnosis criterion; or
unclear diagnostic criteria but were currently treated for psychotic disorders.
Studies involving participants with comorbid physical or mental disorders were eligible for inclusion.
Types of Interventions
Experimental
Control
Treatment as usual,
attention control, or
other active nonpharmacological interventions were eligible.
Types of Outcome Measures
To be eligible, RCTs had to assess at least 1 primary outcome:
improvement in the severity of symptoms of psychosis, measured by clinician-rated scales, such as the Brief Psychiatric Rating Scale, 23 the Positive and Negative Syndrome Scale, 24 the Clinical Global Impression Scale, 25 or any other validated scale; or
hospitalization, assessed as number of hospitalized patients or days in hospital in a predefined follow-up period.
Secondary outcomes included
affect, assessed as
depressive symptoms, measured by self-rating scales such as the Beck Depression Inventory, 26 or by clinician-rated scales, such as the Hamilton Rating Scale for Depression 27 or any other validated scale; and
anxiety symptoms measured by clinician-rated scales, such as the Hamilton Anxiety Scale 28 or self-report scales such as the Beck Anxiety Inventory 29 or any other validated scale;
acceptance, assessed by validated scales such as the Acceptance and Action Questionnaire II 30 ;
mindfulness, assessed by validated scales such as the Kentucky Inventory of Mindfulness Skills 31 ; and
safety of the intervention assessed as amount of extrapyramidal symptoms or number of adverse events.
Search Methods
Medline/PubMed, Embase, the Cochrane Library, and PsycINFO were searched from their inception through April 13, 2015. The literature search was constructed around search terms for “mindfulness- and acceptance-based interventions” and search terms for “psychosis.” For PubMed, the following search strategy was used: (Psychotic Disorders[MeSH Terms] OR Paranoid Disorders[MeSH Terms]OR Affective Disorders, Psychotic[MeSH Terms] OR Psychosis[Title/Abstract] OR Psychotic[Title/Abstract] OR Schizophrenia[MeSH Terms] OR Schizophrenia[Title/Abstract] OR Schizophrenic[Title/Abstract] OR Schizoaffective[Title/Abstract]) AND (Mindfulness[Title/Abstract] OR MBSR[Title/Abstract] OR MBCT[Title/Abstract] OR Acceptance-based[Title/Abstract] OR (Acceptance[Title/Abstract] AND Commitment[Title/Abstract])). The search strategy was adapted for each database as necessary.
Additionally, reference lists of identified original articles or reviews were searched manually, and the Mindfulness Research Guide (www.mindfulexperience.org) was screened.
Two review authors independently screened abstracts identified during literature search and read potentially eligible articles in full to determine whether they met the eligibility criteria. Disagreements were discussed with a third review author until consensus was reached.
Data Extraction and Management
Two authors independently extracted data on patients (eg, age, gender, diagnosis); interventions (eg, type, frequency, duration); control interventions (eg, type, frequency, duration); cointerventions; outcomes (eg, outcome measures, assessment timepoints); and results using an a priori developed data extraction form. Discrepancies were discussed with a third review author until consensus was reached.
Risk of Bias in Individual Studies
Risk of bias was assessed by 2 review authors independently using the risk of bias tool proposed by the Cochrane Back Review Group. 32 This tool assesses risk of bias on the following domains: selection bias, performance bias, attrition bias, reporting bias, and detection bias using 12 criteria as (1) low risk of bias, (2) unclear risk of bias, or (3) high risk of bias. Discrepancies were discussed with a third review author until consensus is reached. Studies that met at least 6 of the 12 criteria and had no serious flaws were rated as having low risk of bias. Studies that met fewer than 6 criteria or had a serious flaw were rated as having high risk of bias. 32
Data Analysis
Assessment of Effect Size
Separate meta-analyses were planned for
short-term (outcome measures taken closest to 4 weeks after the intervention) and long-term effects (closest to 12 months after the intervention) and
different control interventions (treatment as usual, attention control, other) using Review Manager 5 software (Version 5.2, The Nordic Cochrane Centre, Copenhagen) by a random effects model. 20 Meta-analyses were conducted if at least 2 RCTs for a specific comparison were available. 20
For continuous outcomes, standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated as the difference in means between groups divided by the pooled standard deviation. A negative SMD was defined as indicating beneficial effects of the intervention compared to the control intervention for symptoms and affect while a positive SMD was defined to indicate beneficial effects for acceptance and mindfulness. If necessary, scores were inverted by subtracting the mean from zero. 20
To evaluate the magnitude of the overall effect size, Cohen's categories were used with (1) SMD=0.2 to 0.5, small; (2) SMD=0.5 to 0.8, moderate; and (3) SMD>0.8, large effect sizes. 33
For dichotomous outcomes, risk ratios (RRs) with 95% CI were calculated by dividing the risk of event in the experimental group (ie, the number of participants with the respective outcome divided by the total number of participants) by the risk of event in the control group. 20
Levels of evidence were determined using the van Tulder recommendations as (1) strong evidence: consistent findings among multiple RCTs with low risk of bias; (2) moderate evidence: consistent findings among multiple high-risk RCTs and/or 1 low-risk RCT; (3) limited evidence: 1 RCT with high risk of bias; (4) conflicting evidence: inconsistent findings among multiple RCTs; and (5) no evidence: no RCTs. 34
Assessment of Heterogeneity
To analyze statistical heterogeneity between studies, the I 2 statistics, a measure of how much variance between studies can be attributed to differences between studies rather than chance, was calculated. The magnitude of heterogeneity was categorized as (1) I 2 =0%-25%, low heterogeneity; (2) I 2 =26%-50%, moderate heterogeneity; (3) I 2 =51%-75%, substantial heterogeneity; and (4) I 2 =76%-100%, considerable heterogeneity. 35 The chi 2 test was used to assess whether differences in results were compatible with chance alone. Given the low power of this test when only few studies or studies with low sample size are included in a meta-analysis, a P value≤0.10 was regarded to indicate significant heterogeneity. 20
Subgroup and Sensitivity Analyses
Subgroup analyses were conducted for
type of intervention (primarily acceptance-based such as ACT or ABBT or primarily mindfulness-based such as MBCT or MBSR) and
type of participants (manual-based diagnosis; other or unclear diagnosis).
Subgroup differences were tested using a chi 2 test for heterogeneity across subgroup. I 2 statistics for subgroup differences were computed as the percentage of the variance between the different subgroups that is due to genuine subgroup differences rather than chance. 20
To test the robustness of significant results, sensitivity analyses were conducted for studies with high vs low risk of bias. If statistical heterogeneity was present in the respective meta-analysis, subgroup and sensitivity analyses were also used to explore possible reasons for heterogeneity.
Risk of Bias across Studies
Assessment of risk of publication bias was originally planned by investigation of funnel plot asymmetry (using Review Manager 5 software) if at least 10 studies were included in a meta-analysis. 36 However, as less than 10 studies were included in each meta-analysis, funnel plots were not analyzed.
Results
Literature Search
Three hundred seventy-two records were retrieved in the literature search. Of 247 nonduplicate records, 238 were excluded because they were not randomized, did not include patients with psychosis, and/or did not include mindfulness- or acceptance-based interventions. Nine full-text articles on 8 RCTs with a total of 434 patients were assessed for eligibility.37–45 All 8 RCTs were included in qualitative analysis and meta-analysis (Figure 1).

Flowchart of the results of the literature search.
Study Characteristics
Characteristics of the sample, interventions, outcome assessment, and results are shown in Table 1.
Characteristics of the Included Studies
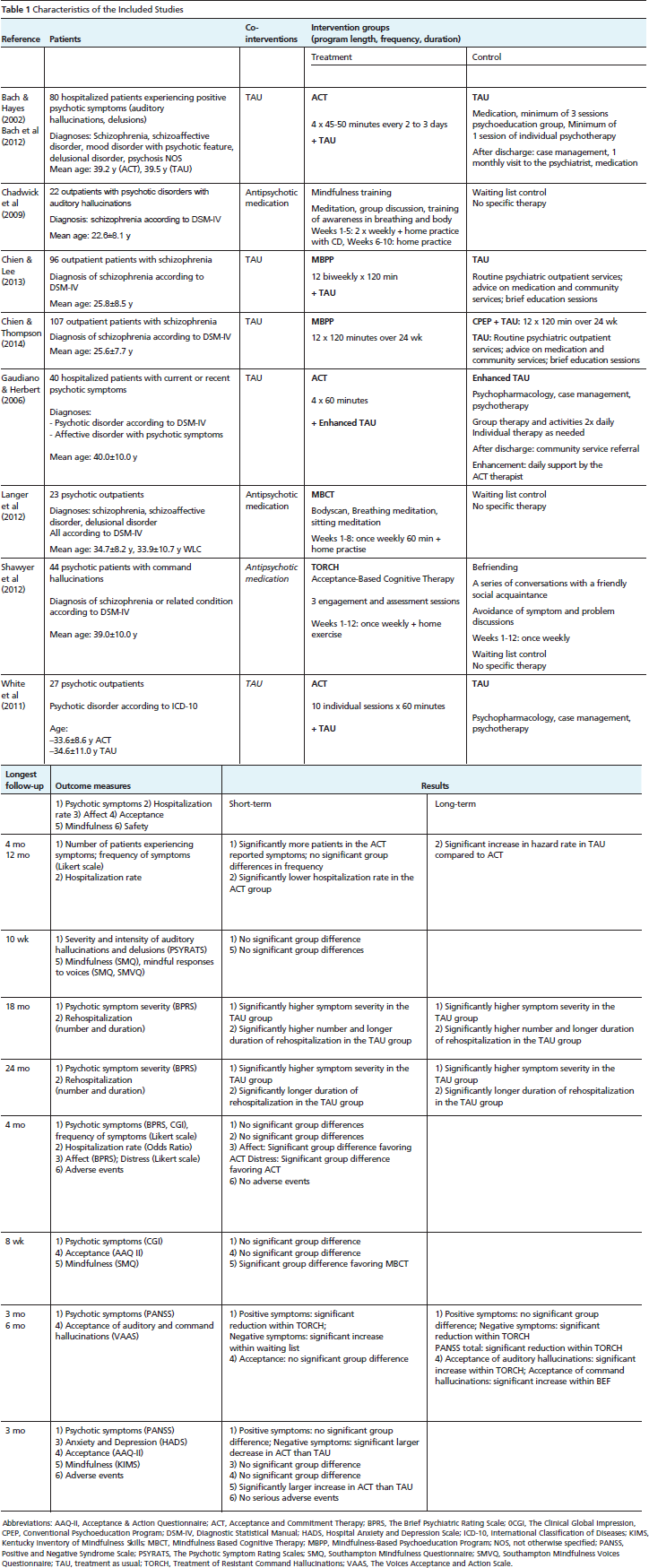
Abbreviations: AAQ-II, Acceptance & Action Questionnaire; ACT, Acceptance and Commitment Therapy; BPRS, The Brief Psychiatric Rating Scale; 0CGI, The Clinical Global Impression, CPEP, Conventional Psychoeducation Program; DSM-IV, Diagnostic Statistical Manual; HADS, Hospital Anxiety and Depression Scale; ICD-10, International Classification of Diseases; KIMS, Kentucky Inventory of Mindfulness Skills; MBCT, Mindfulness Based Cognitive Therapy; MBPP, Mindfulness-Based Psychoeducation Program; NOS, not otherwise specified; PANSS, Positive and Negative Syndrome Scale; PSYRATS, The Psychotic Symptom Rating Scales; SMQ, Southampton Mindfulness Questionnaire; SMVQ, Southampton Mindfulness Voices Questionnaire; TAU, treatment as usual; TORCH, Treatment of Resistant Command Hallucinations; VAAS, The Voices Acceptance and Action Scale.
Setting and Participant Characteristics
Of the 8 RCTs that were included, 2 originated from North America,37,40 3 from Europe,39,41,43 2 from Asia,44,45 and 1 from Australia. 42 Patients were recruited from psychiatric hospitals,37,40 outpatient clinics,44,45 mental health services,42,43 or patient associations. 41 One RCT did not state the setting from which patients were recruited. 39
Patients in 5 RCTs were diagnosed with psychosis or affective disorder with psychotic symptoms according to DSM-IV3942,44,45 or ICD-10, 43 while patients in 1 RCT had a hospital-supplied diagnosis where the diagnostic method was not specified. 37 Between 48.1% and 100% of included patients were diagnosed with schizophrenia. Mean time since diagnosis ranged from 2.6 years to 17.7 years. Patients’ mean age ranged from 25.6 years to 41.6 years; between 22.2% and 45.0% (median: 36.3%) of patients in each study were female.
Intervention Characteristics
Four RCTs used mainly acceptance-based interventions.37,40,42,43 Three of those used modifications of the ACT treatment manual 14 that was modified for patients with psychosis. ACT was offered as 4 individual treatment sessions of 45 to 50 minutes each, 37 10 individual sessions of 60 minutes each, 43 or as a varying number of individual sessions depending on the individual length of hospital stay. 40 All ACT interventions included standard acceptance and mindfulness exercises as outlined in the Hayes et al (1999) protocol 14 ; 1 RCT also included a mindfulness breathing exercise. 43 The fourth RCT used “treatment of resistant command hallucinations” (TORCH), an acceptance-based cognitive behavioral therapy intervention for command hallucinations. 42 Fifteen individual weekly sessions of 50 minutes each and 2 follow-up sessions consisting of belief modification and acceptance-based interventions that were based on ACT were offered. Additional ACT exercises and mindfulness-based exercises were used. Audiotaped mindfulness-based exercises aimed to cultivate a non-judgmental response towards positive psychotic symptoms while ACT exercises and metaphors aimed to implement a detached acceptance of psychotic symptoms. Given that TORCH is a relatively novel intervention, it cannot be regarded as widely accepted.
Four RCTs used mainly mindfulness-based interventions,39,41 1 of those being explicitly based on MBCT. 41 Two interventions used mindfulness meditation and awareness exercises such as body scan and mindful breathing during 10 39 or 8 41 weekly group sessions of 60 minutes each. Cognitive and metacognitive elements were incorporated, and mindfulness exercises were adapted for patients with psychosis. The remaining 2 RCTs used 12 biweekly sessions (120 minutes each) of a not widely accepted mindfulness-based psychoeducation program that combined MBSR with psychoeducation.44,45
In 7 RCTs, the intervention was combined with treatment as usual and compared with treatment as usual alone as the control intervention. Treatment as usual consisted of individual psychopharmacology, case management, and psychotherapy in 5 RCTs37,40,43–45; patients in 2 RCTs were wait-listed and treatment was not specified.39,41 One RCT used befriending as a control intervention, a fully manualized attention control intervention without therapeutic component that was matched with the experimental intervention for contact time and attention. 42
Only 2 RCTs reported on the use of antipsychotic medication during the trial period and reported that compliance to medication was comparable between groups.37,45
Outcome Measures
Severity of symptoms of psychosis was assessed by 7 RCTs using the Brief Psychiatric Rating Scale,40,44,45 the Positive and Negative Syndrome Scale,42,43 the Clinical Global Impression Scale,40,41 or the Psychiatric Symptom Rating Scale. 39 Hospitalization was assessed by 4 RCTs as number of hospitalized patients in a predefined follow-up period37,40 or as mean duration of rehospitalization per patient.44,45 Affect was measured by 2 RCTs using the Hospital Anxiety and Depression Scale 43 or the Brief Psychiatric Rating Scale. 40 Acceptance was assessed by the Acceptance and Action Questionnaire II in 3 RCTs41–43 and by the Voices Acceptance and Action Scale in 1 RCT. 42 Mindfulness was measured by the Kentucky Inventory of Mindfulness Skills 43 or the Southampton Mindfulness Questionnaire39,41 in 3 RCTs. Safety was assessed as number of adverse events in 2 RCTs.40,43
While all RCTs reported short-term effects, only 4 RCTs reported long-term effects.38,42,44,45
Risk of Bias in Individual Studies
Six RCTs had low risk of bias,37,40,42–45 and 2 RCTs had high risk of bias39,41 (Table 2). Risk of selection bias was mixed; only 3 RCTs each reported adequate randomization or adequate allocation concealment. While no RCT reported blinding of participants or providers, all but 2 RCTs39,40 reported adequate blinding of outcome assessors. All but 1 RCT 41 adequately described cointerventions, and 5 RCTs reported acceptable intervention compliance. Attrition bias was mixed as all studies had an acceptable and described dropout rate but only 3 RCTs used an intention-to-treat analysis. Risk of reporting bias and detection bias was low in all RCTs.
Risk of Bias of the Included Studies

Higher scores indicate lower risk of bias.
Outcomes
Mindfulness- and Acceptance-based Interventions vs Treatment as Usual
Meta-analyses revealed moderate evidence for short-term effects on total psychotic symptoms and positive symptoms. Heterogeneity was low to moderate and—based on Cohen's categories—effects were of small to moderate size (Figure 2). No evidence was found for short-term effects on negative symptoms (Figure 2). Moderate evidence was found for lower hospitalization rates and for shorter duration of hospitalization in the intervention groups compared to treatment as usual (Figure 2). Regarding secondary outcomes, no evidence was found for short-term effects on affect and acceptance (Figure 3). There was moderate evidence for short-term effects on mindfulness. Heterogeneity was low and effect size was large (Figure 3).

Short-term effects of mindfulness- and acceptance-based interventions compared to treatment as usual on primary outcomes: total symptoms, positive symptoms, negative symptoms, and hospitalization.

Effects of mindfulness- and acceptance-based interventions compared to treatment as usual on secondary outcomes: affect, acceptance, and mindfulness.
Moderate evidence for long-term effects (12 to 24 months after the intervention) on total psychotic symptoms and for shorter duration of hospitalization in the long term was found in 2 RCTs (Figure 4). Further, hospitalization rate at 12 months was assessed in 1 RCT. 38 This RCT reported reduced hospitalization rates in the intervention group compared to the treatment as usual-group (Table 1).

Long-term effects of mindfulness- and acceptance-based interventions compared to treatment as usual on primary outcomes: total symptoms and hospitalization.
Mindfulness- and Acceptance-based Interventions vs Attention Control
One RCT compared an acceptance-based intervention to attention control and found no evidence for short-term or long-term (6 months after the intervention) group differences for total symptoms, positive symptoms, negative symptoms, or acceptance 42 (Table 1).
Safety
Safety data were reported in 2 RCTs. One RCT reported that no adverse events were observed 40 and the other RCT reported that no “suspected unexpected serious adverse events” were observed. 43 Two further RCTs reported patients that dropped out of the study due to health reasons: 1 patient in the treatment arm of 1 RCT died in a car accident,37,38 and 1 patient in another RCT had a heroin addiction relapse. 39
Subgroup Analyses
In studies on primarily mindfulness-based interventions, moderate evidence was found for short-term effects on total psychotic symptoms. No such effects were found in studies on primarily acceptance-based interventions (Figure 2). Patterns were reversed for positive symptoms. Subgroups were however homogeneous, and no significant subgroup differences were found. Moderate evidence for short-term effects on mindfulness was revealed in studies on acceptance-based interventions and limited evidence in studies on mindfulness-based interventions; subgroups were homogeneous and not significantly different (Figure 3). Long-term effects on total symptoms were revealed for mindfulness-based but not for acceptance-based interventions; subgroups were significantly different (Figure 4).
In subgroup analyses regarding diagnostic method, no evidence was found for short-term effects on hospitalization rate for studies with either manual-based diagnosis 40 (SMD=0.47; 95% CI=0.12–1.82; P=.28) or unclear diagnostic method37 37 (SMD=0.38; 95% CI=0.13–1.09; P=.07).
Sensitivity Analyses
Sensitivity analyses demonstrated a significant effect on total psychotic symptoms and positive symptoms in studies with low risk of bias comparing mindfulness- and acceptance-based interventions to treatment as usual, whereas no such effect was found in studies with high risk of bias. No effects were found for acceptance in studies with either low or high risk of bias while effects on mindfulness were found in both low-risk and high-risk studies. All other comparisons included only studies with low risk of bias.
Discussion
Summary of Evidence
This systematic review found moderate evidence for short- and long-term improvements of psychotic symptoms and hospitalization in patients with psychotic disorders after mindfulness- and acceptance-based interventions compared to treatment as usual. There were no significant subgroup differences between the studies on primarily acceptance-based interventions such as ACT or studies on primarily mindfulness-based interventions.
Agreement with Previous Systematic Reviews
The findings of this meta-analysis are partly in line with those of a previous one that found between-group effects on negative symptoms and rehospitalization but not on positive symptoms for mindfulness- and acceptance-based interventions in patients with psychosis. 46 While this previous meta-analysis included all available uncontrolled and controlled studies, further RCTs that were not included are now available. Differences between the 2 meta-analyses likely stem from differences in inclusion criteria and methods of analysis. A further systematic review on mindfulness-based interventions for severe mental disorders concluded that these interventions might reduce symptom-associated distress and hospitalization for individuals with psychotic disorders. 47 The main difference between the previous reviews and the present one is the inclusion of additional RCTs, presenting the most up-to-date review on the effectiveness of mindfulness- and acceptance-based interventions for psychosis in RCTs. Moreover, the previous reviews did not included a meta-analysis 47 or did not separately meta-analyze effects of mindfulness- and acceptance-based interventions on different outcomes compared to different control interventions. 46
Moreover, the results of the present review are partly comparable to those of cognitive behavior therapy (CBT), which shares many intervention components with both ACT and MBCT, for schizophrenia. These reviews reported effects on mental state but not on hospitalization when comparing CBT to treatment as usual 48 and effects on psychotic symptoms when comparing CBT to other psychological interventions. 49 However, a recent Cochrane review failed to show differences between CBT and other psychological interventions on symptoms or hospitalization in patients with schizophrenia. 50 Another systematic review that included only high-quality RCTs on CBT for early psychosis concluded that CBT can improve psychotic symptoms but did not influence relapse or rehospitalization. 51
A recent meta-analysis on yoga—which shares many similarities with mindfulness meditation and has been shown to improve cognitive function52,53—for schizophrenia found no evidence for effects on psychotic symptoms or hospitalization. 54
External and Internal Validity
Patients in the included studies were recruited from psychiatric hospitals, outpatient clinics, mental health services, and patient associations in North America, Europe, and Australia. All but 1 study 37 used clear and well-accepted diagnostic criteria, and patients with different psychotic disorders were included. The majority of patients were males and in the reproductive-age range. The results of this review are therefore applicable to the vast majority of patients with psychotic disorders in clinical practice.
Two out of 8 studies had high risk of bias.39,41 No evidence of effectiveness on primary outcomes was found in studies with high risk of bias while evidence for effects on total symptoms, positive symptoms, and hospitalization was found in studies with low risk of bias. Therefore, this evidence can be regarded as robust against potential methodological bias.
Strengths and Weaknesses
A major strength of this review is that, besides psychopathology, patient-centered outcomes were used. 55 Most of the included studies had low risk of bias and the evidence of effectiveness was robust against potential bias. While patients were recruited from different facilities and it could be argued that this would influence severity of symptoms, all significant meta-analyses were free of statistical heterogeneity, suggesting comparability between studies.
The primary limitation of this review is the small total number of eligible RCTs. As no unpublished studies were included in this review and publication bias could not be assessed, it cannot be ruled out that further unpublished RCTs exist that could add further and possibly conflicting evidence. While the included studies suggest superiority of mindfulness- and acceptance-based interventions to treatment as usual, no studies were available that included a head-to-head comparison to other active interventions. While subgroup analyses were conducted to separately analyze the effectiveness of primarily acceptance-based and primarily mindfulness-based interventions, the small number of RCTs in each subgroup limits their expressiveness. Only 2 RCTs reported data on compliance to antipsychotic medication, the possible influence of differences in compliance on trial outcomes thus could not be assessed. One might further question the comparability of primarily mindfulness-based and primarily acceptance-based interventions. As outlined above, while these approaches share many similarities, the practical techniques used in each intervention might strongly differ. Moreover, the different approaches have different therapeutic foci: eg, MBCT has been designed as an intervention for relapse prevention in major depression 16 and has been shown to effectively ameliorate recurrent depression. 56 On the other hand, ACT has a more broad focus and has been evaluated in a number of psychiatric conditions. 57 However, there is no condition yet for which effectiveness of ACT is conclusively established. 58 Therefore, the interpretations of overall effects might be less valid than those of the subgroup analyses.
The included studies used varying interventions with and without concomitant medication and varying control group conditions. These factors might weaken the conclusions of this meta-analysis.
Implications for Further Research
While psychopharmacological treatment is the most important intervention for psychosis, its effectiveness on negative symptoms is limited 6 and a considerable number of patients are therapy refractory. 7 Thus, patients may require adjunctive psychotherapeutic interventions to help them cope with symptoms that are not effectively treated with antipsychotic medication. Given the low number of available studies, definite conclusions about the effectiveness of mindfulness- and acceptance-based interventions for that end are impossible. However, in light of the preliminary evidence found in this review, further research seems warranted. Future studies should ensure rigorous methodology and reporting, mainly adequate randomization, allocation concealment, and intention-to treat analysis. 59 While blinding of participants or providers might not be possible in interventions that involve complex interactions between patients and providers and should thus not be regarded as a lack of quality of the study (while it is still a possible source of bias), adequate blinding of outcome assessors should be intended all the more in future studies. Besides comparisons with treatment as usual or attention control, head-to-head studies are needed to compare the effects of mindfulness- and acceptance-based interventions with those of more traditional approaches—eg, cognitive-behavioral interventions.
Implications for Clinical Practice
While the expressiveness of the findings of this meta-analysis is somewhat limited by the small number of included RCTs, the clearly positive findings are encouraging. No intervention-related serious adverse events were reported. While single cases of psychotic relapse after unsupervised meditation practice and even meditation-induced psychosis have been reported, 60 there seems to be little risk of relapse and aggravation of psychotic symptoms in supervised mindfulness- and acceptance-based interventions. Thus both mindfulness- and acceptance-based interventions can be recommended as additional treatments for patients with psychosis but should be closely supervised by adequately trained therapists.
Conclusions
This systematic review and meta-analysis found moderate evidence for short- and long-term effects of mindfulness- and acceptance-based interventions on psychotic symptoms, hospitalization, and mindfulness in patients with psychotic disorders. Both types of interventions can be recommended as an additional treatment for patients with psychosis.
Footnotes
Acknowledgments
This review was supported by a grant from the Rut- and Klaus-Bahlsen-Foundation. The funding source had no influence on the design or conduct of the review; the collection, management, analysis, or interpretation of the data; or in the preparation, review, or approval of the manuscript.