
Abstract
This work addresses the design of an active multi-link micro-catheter actuated by Shape Memory Alloy (SMA) micro actuators. This may be a response to one medical major demand on such devices, which will be useful for surgical explorations and interventions. In this paper, we focus on a training and design simulator dedicated to such catheters. This simulator is based on an original simulation platform (OpenMASK). The catheter is a robotic system, which is evaluated by a dynamical simulation addressing a navigation task in its environment. The design of the prototype and its mechanical model are presented. We develop an interaction model for contact. This model uses a real medical database for which distance cartography is proposed. Then we focus on an autonomous control model based on a multi-agent approach and including the behaviour description of the SMA actuators. Results of mechanical simulations including interaction with the ducts are presented. Furthermore, the interest of such a simulator is presented by applying virtual prototyping techniques for the design optimization. This optimization process is achieved by using genetic algorithms at different stages with respect to the specified task.
1. Introduction
In this paper*, we focus on a dynamical simulator dedicated to the global design, by means of virtual prototyping methods, of an active micro-catheter. These devices are fully in the scope of surgeons demand for near future, because it enables the operating gesture to be assisted (Cohn, M., Crawford, L., Wendlandt, J. & Sastry, S. S. 1995) and thus, minimises one patient hurt during intervention. Though prototypes of such systems exist for more than ten years (Lim, G., Minami, K., Yamamoto, K., Sugihara, M., Uchiyama, M. & Esashi, M. 1996), few work is dedicated to the computer aided design process of this kind of devices Dumont, G., Chapelle, F. & Bidaud, P. 2001) (Ikuta, K., Iritani, K. & Fukuyama, J. 2001). Classic flexible endoscopes are generally constituted of articulated links, actuated by four cables connected to the head of the endoscope. The motion is achieved by means of knurls that are pulled by the surgeon. A new generation of active endoscopes was developed by Olympus (Takehana, S., Ueda, Y., Gotanda, M., Sakurai, T. & Adachi, H. 1990). The head orientation is controlled through flexion modules activated by SMA actuators. However, this system does not adapt its curvature to the environments. Developments of new prototypes, aiming at improving the navigation of endoscopes in the inspected ducts, are in progress. A prototype developed in Japan (Park, K. & Esashi, M. 1999) is constituted of trays interconnected by SMA threads (Fig. 1). Piloting the length of the above-mentioned thread controls the orientation between two constitutive trays that are connected by three SMA threads.

Multilink active catheter
We propose a brief description of the real prototype and outline the interest of designing a training simulator. As this prototype has to be agile enough to crawl its way inside complex environments as human ducts, we have chosen a modular stiff poly-articulated structure presented on Fig. 2 and designed in our laboratories (Szewczyk, J., Sars, V. D., Bidaud, P. & Dumont, G. 2000) and (Kühl, C., Dumont, G., Mognol, P., Gouleau, S. & Furet, B. 2002). The chosen mechanism consists in a succession of modules related to each other by pin joints, which are alternatively oriented at 90°. This configuration allows a 3D motion of the structure.

Schematic view of the prototype
The endoscope head should contain a device allowing obtaining a multi-directional vision of the observed space. This will be achieved by using a polymer gel actuated prism. As medical device, a flexible polymer sheath should protect the whole system. Each joint is provided with two antagonist electrically commanded SMA spring-like actuators allowing to control the relative orientation. An integrated circuit controlling the electrical power supplied to the SMA realizes the command.
Fig. 3 presents our simulator, which objective is to realize virtual navigation in a patient body, modelled by a reconstruction of the digestive tract obtained by Magnetic Resonance Imaging (MRI). The feelings will be maximal by using graphic and haptic interfaces provided by the virtual reality techniques.
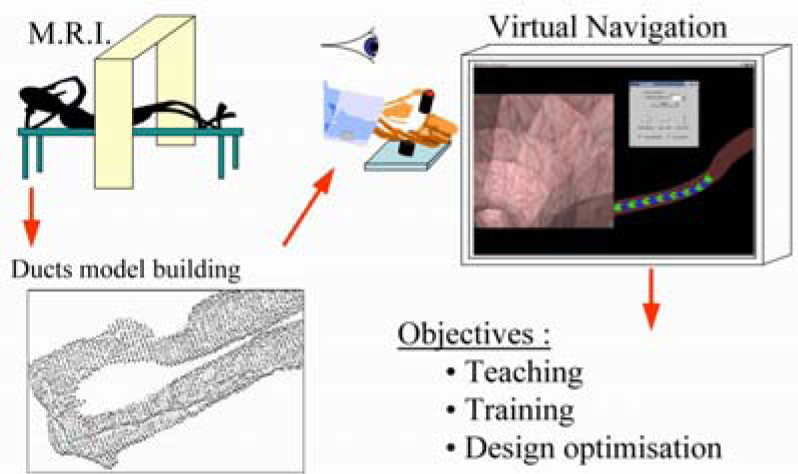
Proposed Simulator
The computational model used is the one of the real prototype simultaneously designed in our laboratories, as mentioned above. The interests for a design and training simulator are triple:
Teaching to young surgeons: the training on simulator is obviously more accessible, less expensive and less risky and should allow to experiment pathologic cases; Preoperative training: the simulator will allow the surgeon to virtually repeat the operation on the patient, before the real operation; Virtual prototyping (Dumont, G., Kühl, C. & Bidaud, P. 2002): furthermore, the simulator allows to virtually test the tool quality with respect to a given operation task. So, by optimization techniques based on genetic algorithms, we can test which is the best candidate to achieve this task, and propose an adapted endoscope.
In the following, we will present the simulator components. In order to deal with endoscope toward ducts interaction, we present the “devoxelisation” process, which leads to an interpolated distance cartography of the ducts. This database construction is used to minimize the computation time for treatment of the interactions. The contact detection algorithm, allowing determining these interactions forces between the endoscope model and the duct model is then presented. Let us notice that an important experimental work should be lead to identify the parameters of this contact model. A result will illustrate the simulation process. To minimize one patient hurt during operation, we use the control capability of the device. We will address it by a multi-agent control strategy for controlling the catheter conformation to the ducts and compare this method to the uncontrolled case. It is shown that the magnitude of contact forces decreases.
The third proposed use of the simulator is the design optimization of the prototype. To address this purpose, the simulator is coupled to genetic based algorithms. This allows showing the feasibility of an optimization process for geometric conditions, where the design is optimized with respect to accessibility conditions. We propose also an optimization process for dynamic conditions, where a dynamical simulation of the system evaluates the design during the realization of an inspection task in the environment.
2. Description of the simulator
A mechanical model of the proposed real prototype allows us to better understand its capabilities. The model is a kinematical open chain described by a Denavit and Hartenberg representation. The obtained dynamic equations (Kühl, C. 2003) are classically written as:

In this equation, q is the vector of the parameters describing the configuration, G represents the gravity effect, K represents the elasticity effect of the SMA actuators in uncontrolled configuration and F represents the forces exerted by the SMA actuators in the controlled configuration and the contact forces. These equations are resolved by using C++ libraries (Barenburg, B. 2000). The approach is based on six degree of freedom (DOF) object models and uses an iterative constraint correction method. We solve the equations by using a Runge-Kutta (2 or 4) algorithm, according to the Newton-Euler laws of motion. Then, as the joints are translated into term of geometrical constraints, an iterative constraint correction method is used by means of a Newton Raphson algorithm.
The management of the simulator is implemented on the OpenMASK† platform (Margery, D., Arnaldi, B., Chauffaut, A., Donikian, S. & Duval, T. 2002) developed at IRISA. The main objective of OpenMASK is to propose a modular simulation to be executed on various material configurations. The platform manages the synchronization and the exchanges of data between the co-operative processes insuring a “dilated real time” in its standard version. It is developed by using the specificities of the object-oriented programming. The synoptic of its organization is presented on Fig. 4.

OpenMASK: Modular Animation and Simulation Kit
Various models (Fung, Y. C. 1984) are proposed to describe the behaviour of human organs or tissues, including non-linear behaviour and relaxation. A first approach, because the interaction occurs between a stiff body imposing the motion (the links of the endoscope on one hand) and a soft body (human tissues on the other hand), is to compute the reaction force by a compliance method. This method is applicable with respect to the dynamical model and furthermore is a rapid computation method, which is in the scope of our objective to realize “real-time” simulations. The proposed method for interaction treatment consists in three steps:
As geometrical detection is obviously time consuming, the first stage consists in a pre-processing method to build, from the rough MRI (Magnetic Resonance Imaging) medical database, an interpolated distance cartography in the space which is presented, for a slice of the duct, on Fig.5; The second stage of the reaction force computation is ensured by geometric collision detection. The links of the endoscope model are represented by interaction points for which collision is tested by calculating the distances from each interaction point to each “voxel” of the human duct model. This determines the distance from the point on the devices to the duct. In case of collision, a classical compliance effort is applied to the link, which is proportional to the penetration depth and to the penetration velocity. Let dist be the penetration depth computed during the second stage,

Pre-processed Medical database (one slice)

Insertion into a medical database
3. Endoscope command
The ability to pilot the orientation of the links allows an easier introduction in the virtual duct and constitutes the major interest of using active devices.
So, we have developed a module defining a controller, which commands the mechanical model. The controller is based on the geometrical description of the connections between two neighbouring links and on the behavioural characteristics of the SMA actuators, for which a model as been proposed in (Troisfontaine, N. & Bidaud, P. 1998).
The behaviour of the controller for a 15 links catheter and for an orientation consign of 10°, illustrated on Fig. 7, shows a response time of 0.4s and a good precision. The stability is good for the links located near to the head. The links located near to the basis shows oscillations, which are due to the important inertia supported. To take benefit of the active property of the catheter, a command strategy is proposed. Its objective is to automatically adapt the endoscope curvature to the shape of the inspected ducts. In the real world, this will allow to minimise the contact between the endoscopic device and the inspected channel, in order to minimise wound during the operation. On Fig. 8, we present a simulation with a pushed device without any joint control: the applied forces onto the duct, represented by the red vectors, are very important.
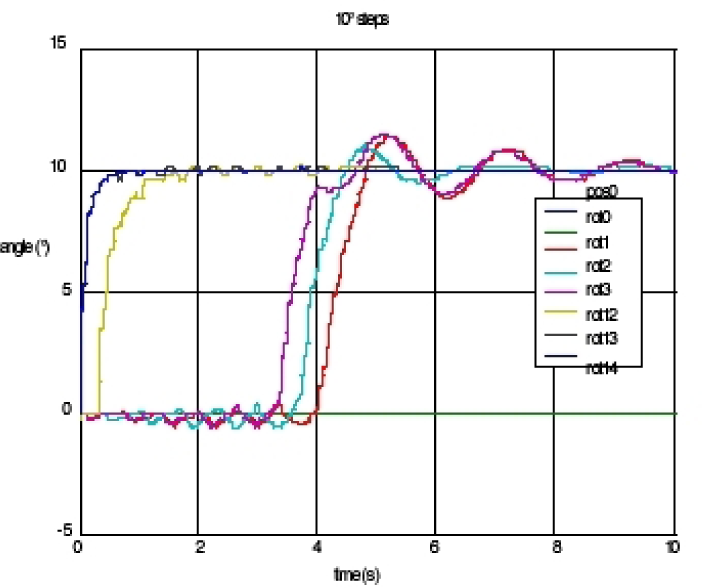
Response time

Simulation without joint control
The used command strategy is based on a multi agent approach. It consists in splitting the steering mechanism into independent sub-systems, which constitutes the agents (Duhaut, D. 1993).
This distributed modular solution is independent from the structure length and should minimise the amount of information exchanged between the agents. The principle, presented on Fig. 9 for a two dimensional model, is quite simple. If an effort is detected on one of the links, which, in real world, will be achieved by piezoelectric film sensors, an orientation consign is applied to the preceding joint so as to decrease this interaction effort, and the opposite consign is affected to the next joint. The effect is, on one hand, to minimise the contact effort and, on the other hand, to ensure an unchanged orientation of the endoscope head. Numerical tests on stability show that the agent should be constituted of at least two consecutive links in the bi-dimensional case. The three-dimensional extension consists, because of the relative orientations of the pin joints, in agents constituted of four links. An endoscope piloted with this strategy is proposed, for a three-dimensional model, on Fig. 10. This method, based on the contact detection, seems to be adapted to human ducts inspections and strongly limits the interaction efforts.

Multi-agent approach (2D principle)

Result with a multi-agent control
4. Optimization by genetic algorithms
The techniques of virtual prototyping aim at improving the quality of the developed prototypes. In order to test the product functionalities, which could not easily be tested on real prototypes, we use the above described simulation process. The quality of the model, with respect to the task to accomplish (for example: a navigation task) can be measured by an objective function (Endo, K. & Maeno, T. 2001). This function could take into account the developed energy to accomplish the task, which represents the comfort of the surgeon during the operation, and the magnitude of the developed efforts during contact phases, which represents the security of this operation. In order to minimise the objective function, which leads to a better device, we use genetic algorithms (Wall, M. 1996) that have a good solution space exploration capability and lead to acceptable design solutions. Genetic algorithms imitate the natural process of species evolution (Darwin, C. 1859): an individual survives only if it can adapt to the surrounding environment. When it reproduces, its genes are transmitted to its descent.
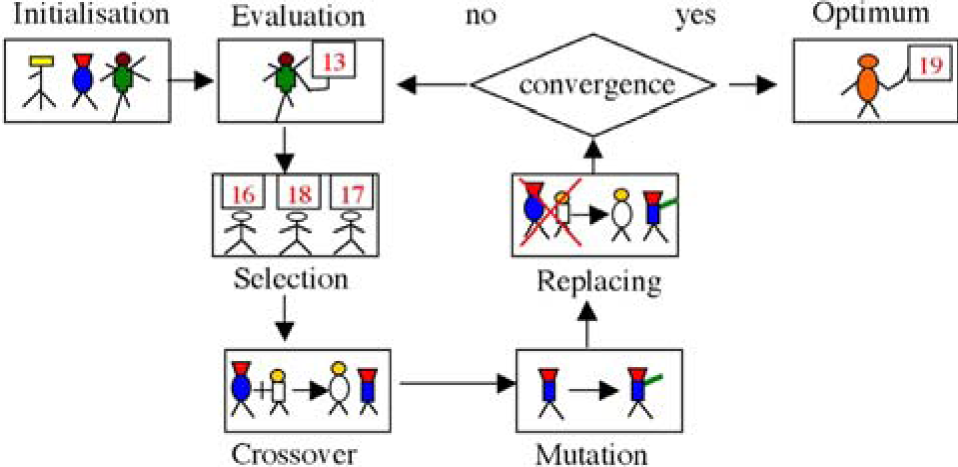
Among these genes, some mutates naturally. The whole involved process is presented on Fig.11 and the algorithm is defined as follow:
Initialisation of the population, this step is performed only once; The evaluation of each candidate is done by performing a simulation in order to evaluate the objective, or cost, function; The best candidates are selected, by using partially unpredictable selection. This allow to keep mainly the candidates with a good performance, with respect to the specified task, but furthermore to have less good candidates which could lead to good descent; Among the so obtained population, the crossover is performed in order to generate a new population being intended in replacing the first one; In order not to impoverish the genetic content of the population a non determinist mutation is performed; The obtained population constitutes the initialisation of the next algorithm step; Convergence criterion may be defined as the number of generation, which ensures that the algorithm stops but does not ensure a strict convergence. Nevertheless, this test shows good results. Another criterion may be based on the average evolution of the population quality between to steps, insuring controlled convergence with inconvenience of possibly being endless.
Genetic algorithms
As usual with optimization processes, we have to define optimization variables: for the catheter case, with the modular proposed structure, we can choose the length of each link, the number of used links. This could lead to conceive the best prototype for one given inspection task As the computation time, involved by this method, is obviously a punishing factor, leading to limit the investigation domain, we have chosen to define various complexity optimization levels:
The first level consists in a purely geometrical analysis: at this step, for which a result into a 3D-duct model is presented on Fig. 12, we use an objective function built on the length and the number of links During the progression, the endoscope should interact at least with the patient tissues, so the average line of the channel to inspect defines the trajectory to follow. For this given trajectory, the algorithm aims at defining a prototype, which presents a good following capability, with a minimum number of links. Thus the objective function is defined by: The second level is a degraded mechanical optimisation: at this stage, the good candidates, issued from the first step, presents a good conformation to the trajectory. The purpose is here to determine the actuators parameters insuring a good follow-up of trajectory. It is called a degraded mechanical simulation in the sense that the mechanical model of the device is used but no interaction with the duct is taken into account. This is the purpose of the third level; The third level should lie on a complete mechanical optimization: at this step, we dispose of models, which have the ability to follow correctly the predefined trajectory, avoiding the contact. The complete simulation is initialized with the lengths obtained during the first stage and with the mechanical and actuators parameters resulting from the second one. The interaction model is then introduced, and the objective function is the one related to the task to accomplish. It should lead to the best endoscope for this task and furthermore could take into account the mobility of the inspected duct.

Result for 3D geometrical optimisation

Improvement function
In the presented optimization result (Fig. 12), each generation is composed of 40 individuals, and the computation is carried out on 80 generations. This number is chosen as convergence criterion for the optimization process. The optimization variable is the length of each link, which can be chosen between 4 to 18mm, by step of 2mm (coded on 3 bits). The number of used links is variable. The computation time, using an 800 MHz Pentium III with 256 Mo of RAM is around 3 minutes. The optimal solution presented is a 31 segments endoscope and the maximum distance from links to the trajectory is 5 mm. This optimization stage gives satisfactory results: indeed, the procedure does not find the trivial solution which is the endoscope made up of the segments of the smallest size, which solution is the closest to the trajectory but which results in an endoscope having a great number of segments.
5. Conclusion and future works
The simulation with multi-agent controller, presented on Fig. 10, proves the validity of this approach for minimizing contacts into the ducts, furthermore it can easily be extended to the case where the ducts are not rigid but elastically, or visco-elastically deformable, as in reality (Kühl, C. 2003). A simulation result of this case is presented on Fig.14.

Sigmoid untwisting
We have developed a simulator allowing to compute the progression of a poly-articulated endoscope, based on an under development real prototype, actuated by SMA actuators with identified behaviour model. This simulator is based on a mechanical description of the device and on the interacting environment, specific to the considered patient, through a medical MRI acquisition. As mentioned in the introduction, an experimental work is to be done in order to identify the contact model parameters. Different control strategies for the actuators have been proposed, which results have been presented and which give good results to minimize the contact between the catheter model and the patient database. In order to improve the accuracy of the considered prototypes, the use of the simulator seems to be a good direction especially when coupled to optimization process. We have proposed different optimization approaches by genetic algorithms and developed some results. Geometrical optimization gives cheering results: it has been shown to predetermine endoscope segments lengths. The second stage of degraded mechanical optimization should allow identifying mechanical parameters adapted for the actuators choice. This optimization procedure will be very similar to the geometrical optimization one, last generation of which will be used to initialize this second stage. Springs and damps will be added to the already calculated lengths. They will be evaluated with criteria taking into account the displacements, the eigen frequencies and the damping in order to obtain satisfactory within the minimum of generation steps, since here time of test for each individual will be considerably increased. Then, they will be generalized to the whole system parameters, as segments diameter or thrusts value, in order to be able to propose the most powerful structure to the surgeon.
The lake of interfacing capabilities, especially in the haptic domain, needs to be examined. It is expected that such devices should improve the control over the catheter in order to define “real” tasks to accomplish in real time. This would also allow to feel the contact between the catheter and the ducts in order to produce a training simulator.