
Abstract
Continuous improvement initiatives have proliferated among manufacturing and services organizations. In this context, knowledge has been claimed to play a key role, as a significant antecedent of an organization's ability to continuously improve its performance. At the same time, attempts to implement knowledge management initiatives prove fruitless if employees are not fully motivated and engaged, and our present understanding of how to promote and facilitate such behaviours remains limited. This study introduces and empirically tests a theoretical model that links intellectual capital dimensions to employees innovative work behaviour and specifically suggests knowledge sharing behaviour among employees as a key mediator. A survey was used to collect data from 135 employees in three healthcare organizations. The results of our structural equation modelling (SEM) analysis indeed support the notion that intellectual capital is conducive to innovative behaviour by means of knowledge sharing among employees. These findings contribute to the understanding of how behavioural factors operate in organizations, highlighting the relevance of a micro-foundation of continuous improvement, and also suggesting some preliminary guidelines that managers in healthcare organizations can apply to promote employee innovative work behaviour.
1. Introduction
Ageing and recession are concerning healthcare policy makers worldwide in terms of sustainability of healthcare expenditure over the next decade. In fact, healthcare is expected to consume 20% of GDP by 2017 in many OECD countries [1]. Governments are committed worldwide to rationalize – or at least contain – healthcare expenditure, fostering technological and organizational changes. Despite these efforts, health cost per capita has continuously increased over the last decades. As a matter of fact, healthcare is affected by a cost disease [2] and consequently healthcare is unable to improve the average productivity despite the adoption of new technologies or organizational changes. This is because healthcare is heavily labour-intensive and only a radical change of healthcare professionals' behaviour can boost productivity over time. Over the last few decades, a number of researchers began to investigate how to improve performance of healthcare organizations and deliver more for less. Many of them claimed that healthcare organizations are knowledge-intensive organizations and thus improved knowledge assets dynamics could enable performance improvement [3,3]-[5]. Recently [6] found a positive relationship between intellectual capital management and above average performance in Taiwanese hospitals, and they claimed that cost-effective intellectual capital management is a trigger for performance improvement in healthcare. This result is coherent to what other researchers claimed for many private and public sector organizations [7,7]–[9]. Despite these results, the understanding of the modalities by which intellectual capital might enable performance improvement in healthcare is still “a black box”.
This paper aims to shed first light on the process that makes intellectual capital a leverage of performance improvement in healthcare organizations. In particular, this linkage has been investigated by specifically exploring the mediating effect that knowledge sharing behaviour has on the relationship between intellectual capital dimensions and innovative work behaviour.
2. Research Framework and Hypothesis Development
Intellectual capital - defined as the sum of all knowledge that organizations utilize for competitive advantage - plays a key role in innovative performances [8]. As [10] observed, “the special capabilities of organizations for creating and transferring knowledge are being identified as a central element of organizational advantage”(p. 256). The knowledge-based view of organizations strongly fits with the analysis of innovation which can be defined as the process of creating new knowledge and embedding it into products and practices [11]. Accordingly, several scholars have devoted much effort to investigate: (a) the role of intellectual capital in improving organizational performances, such as innovative and learning capabilities [8,8], and (b) how organizations can leverage intellectual capital in order to attain such improvements [13,13].
Less attention has been devoted in investigating the role of intellectual capital at the individual level of innovation. Nevertheless, new knowledge always begins with the individual [10] and understanding how intellectual capital affects individuals is central to understanding how organizations can activate the “spiral of knowledge” (ibidem, p. 3) that leads to innovation.
Accordingly, this paper aims at improving the understanding of the linkage between intellectual capital and practitioners' innovative behaviours.
Innovative work behaviour can be defined as individuals' behaviour aiming at introducing new and useful ideas, processes and products into their work environments [15]. Several contributions have stressed the importance of innovative behaviour in fostering continuous performance improvement [16,16]–[18] which contrasts with the evidence of workers “largely designed to focus on, harvest, and protect existing practices rather than pay attention to developing new ideas” [19] (p. 591).
2.1 Impact of Intellectual Capital on Innovative Behaviour
Several authors observed that “while the invention or conception of innovative ideas may be an individual activity, innovation (inventing and implementing new ideas) is a collective achievement” [19] (p. 591). Accordingly, past research points out that organizations have to support individuals' innovative behaviour through a proper management of intellectual capital [8]. Then, intellectual capital management is necessary to exploit individuals' innovative potential. Therefore we propose the following:
Hypothesis 1: Practitioners' perception of the intellectual capital of the organization positively affects their innovative work behaviour.
In order to make the most of the results from this hypothesis, the concept of intellectual capital needs to be explored. Intellectual capital is a multi-faceted concept which comprises three distinct and interrelated dimensions: human, organizational and social capital [8]. This distinction is crucial because each dimension of intellectual capital requires specific sets of human resource, information technologies and research and development investments [20]. First, human capital is the set of knowledge owned and used by individuals. Second, organizational capital represents the codified knowledge present in procedures, guidelines, databases and manuals. Last, social capital is the interactive knowledge that individuals can access through social networks.
Accordingly, we break down hypothesis 1 into the following:
Hypothesis 1a: Practitioners' perception of the human capital of the organization positively affects their innovative work behaviour.
Hypothesis 1b: Practitioners' perception of the social capital of the organization positively affects their innovative work behaviour.
Hypothesis 1c: Practitioners' perception of the organizational capital of the organization positively affects their innovative work behaviour.
Past research supports the idea that the impact of intellectual capital on organizational performance may be indirect. In fact, some authors draw a distinction between intellectual capital and knowledge management, with the first being related to “building and governing intellectual assets from strategic and enterprise governance perspectives” [21](p. 400) while the latter is more operational and “focuses on facilitating and managing knowledge-related activities such as creation, capture, transformation and use” (ibidem).
This distinction suggests that intellectual capital, in order to affect organizational performance – and, thus, innovative work behaviour – should pass through knowledge management-related activities [22].
Specifically, we identified knowledge sharing as a necessary pre-requisite for intellectual capital to be translated into innovative behaviour. Knowledge sharing is defined as the deliberate action in which health practitioners diffuse relevant information to others across and outside the organization [23]. As such, it is a decisive activity for knowledge management because it is the trigger that activates effective exchanges of knowledge between individuals. We therefore propose the following:
Hypothesis 2: Practitioners' perception of the intellectual capital of the organization indirectly affects their innovative behaviour through knowledge sharing.
This general hypothesis must be broken down into the following two:
Hypothesis 2a: The enactment of knowledge sharing has a positive impact on practitioners' innovative behaviour.
This hypothesis is supported by recent contributions which have directly linked the enactment of knowledge sharing with an improvement of individual innovative behaviour, especially in knowledge-intensive industries [24,24]. While the linkage between knowledge sharing and innovative behaviour has not been widely investigated in the literature, knowledge sharing is largely acknowledged as a critical activity for organizations to obtain competitive advantages and improve individuals' performances [11].
Hypothesis 2b: Practitioners' perception of the intellectual capital of the organization has a positive impact on knowledge sharing behaviour.
Having defined intellectual capital as the sum of knowledge residing in the individuals and in the organizations, it may seem obvious to draw a direct connection with the enactment of knowledge sharing behaviour. Such a direct linkage may suggest that an increase of knowledge stocks would “automatically” bring an increase in the level of knowledge sharing, without any kind of mediation. This assumption is largely opposed by findings from past research which identifies individuals' willingness to share as a key driver for the translation of any managerial interventions aimed at increasing knowledge stocks into actual knowledge sharing.
Despite all the positive outcomes it may bring, in fact, knowledge sharing has long been described as unnatural and impossible to mandate because of the existing information asymmetry between hospital managers and practitioners [26,26]–[28]. Accounts of failures related to mandatory solutions have led many authors to define knowledge sharing as an essentially individual behaviour which is driven by internal and external factors [29,29].
Accordingly, we investigate the linkage between intellectual capital and knowledge sharing behaviour by exploring the mechanisms through which the first generates a positive intention to share knowledge in individuals.
2.2 Theory of Planned Behaviour
In order to do so, we draw on the established theory of planned behaviour (TPB) [31]. Coherently with our needs, this theory argues that the enactment of a behaviour is primarily explained by the individual intentions. TPB postulates that intention is affected by three different constructs: attitude, subjective norm and perceived behavioural control (PBC). Specifically, attitude suggests that individuals may be willing to share because they have a positive perception of the benefits they can attain through engaging in this behaviour. On the other hand, subjective norm reflects the idea that individuals may be motivated to share in order to comply with pressures and requests coming from relevant people in their environment. Last, perceived behavioural control (PBC) posits that individuals may not be willing to share because they perceive difficulties in engaging in this behaviour and controlling its consequences. PBC is also treated as a proxy of the actual behavioural control that may inhibit individuals from sharing despite their positive intention. As such, this construct has both a direct effect on knowledge sharing (as a proxy for actual control) and an indirect one (as a measure of perception).
Through the lens of TPB, we have then the following set of knowledge sharing-related hypotheses:
Hypothesis 3a: Practitioners' intention to share knowledge positively affects their knowledge sharing behaviour.
Hypothesis 3b: Practitioners' attitude toward knowledge sharing positively affects their intention to share
Hypothesis 3c: Practitioner's subjective norm positively affects their intention to share knowledge.
Hypothesis 3d: Practitioners' perception of behavioural control positively affects their intention to share knowledge.
Hypothesis 3e: Practitioners' perception of behavioural control positively affects their knowledge sharing behaviour.
Once we define which factors affect practitioners' intention to share, it is possible to get back to Hypothesis 2b and clarify how intellectual capital can affect knowledge sharing.
2.3 Impact of Intellectual Capital on Knowledge Sharing Behaviour
Several contributions support the idea that intellectual capital may support intention to share and thus its enactment. First, human capital regards the extent of knowledge residing within individuals in a community. Scholars argue that it would improve the quality in the content of knowledge exchanges and improve sharers' “cognitive-based trust”, i.e., confidence that the shared knowledge would not get wasted or be misused by the recipients [32]. The perception of high human capital, then, may lead, on one hand, to greater expectations of benefits attainable from knowledge sharing. We therefore propose the following:
Hypothesis 4a: Practitioners' perception of the human capital of the organization positively affects their attitude towards knowledge sharing.
Social capital is the single most studied intellectual capital dimension in relation to knowledge sharing because it affects individuals and organizations in many ways. First, since social capital is strongly related to the concept of reciprocity, it may affect individuals' evaluation of the benefits attainable with knowledge sharing (and thus, attitude). In terms of social exchange theory, individuals, by sharing their knowledge, expect that they will be socially rewarded, with increased approval, status and respect [33]. Second, social capital is strongly related to the concept of relational embeddedness, that is the strength of relationships that individuals have developed over time through continuous interactions. Then, stronger social ties between individuals leads to an increasing reciprocal influence [34]. Last, past research has frequently investigated the impact of social capital-related concepts on the perception of control over knowledge sharing. The two most notable findings relate to the role of trust and social connections. Trust has been often acknowledged as “the single most important precondition for knowledge exchange” [35] (p. 239) and is specifically important in those organizations, such as hospitals, where control mechanisms cannot be fully deployed [36]. Strong ties between individuals, on the other hand, has deemed as necessary in order to transfer tacit knowledge [34] which is the most frequent form of health knowledge [37]. Consequently we propose these hypotheses:
Hypothesis 4b: Practitioners' perception of the social capital of the organization positively affects their attitude towards knowledge sharing.
Hypothesis 4c: Practitioners' perception of the social capital of the organization positively affects their perceived behavioural control.
Hypothesis 4d: Practitioners' perception of the social capital of the organization positively affects their subjective norm.
Organizational capital regards the extent and quality of knowledge embedded in codified text. Codified text may facilitate individuals because it is: (a) simpler for practitioners to transmit explicit knowledge than tacit knowledge and (b) simpler to monitor its flow for hospital managers [11]. Yet, there are several limitations. Health knowledge is mostly made of narratives and heuristics, and thus it cannot be fully translated into codified text [38]. Furthermore, codified texts are sometimes regarded as being of negligible importance if compared to the tacit knowledge that lies beneath them [39]. Codified text, in fact, may de-contextualize the tacit knowledge and, thus, reduce its value [40]. We thus propose the following:
Hypothesis 4e: Practitioners' perception of the organizational capital of the organization positively affects their perceived behavioural control.
The resulting conceptual model for our research framework is described in Figure 1.
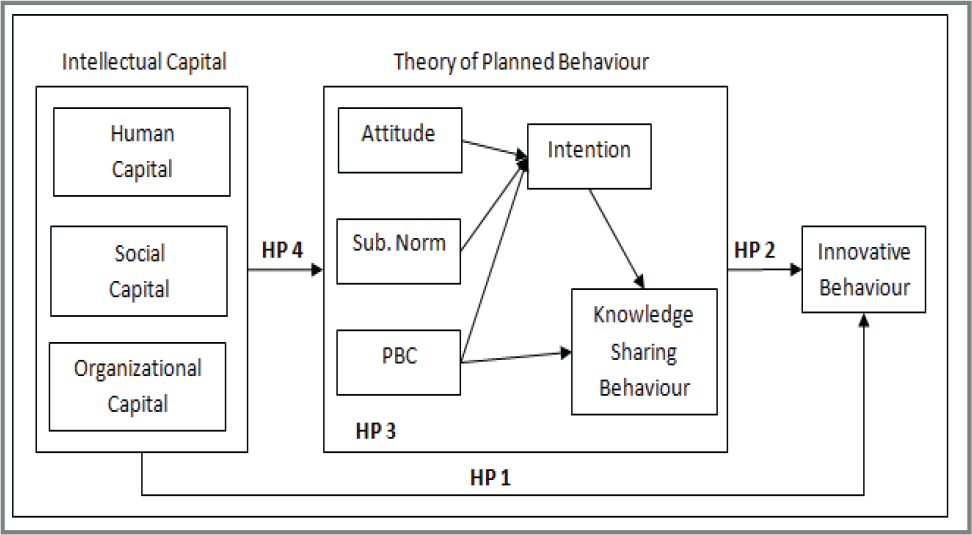
Conceptual framework
3. Methods
Data for this study were collected using a survey instrument. Since the unit of analysis was individual professionals, all data came from primary sources. Control variables were also collected from respondents, but were subsequently double-checked using secondary sources of information.
3.1 Sample
To collect data we involved three Italian hospice and palliative care organizations (H&PCOs). We decided upon palliative care as the research setting because of the necessary multidisciplinary approach needed when taking care of this kind of patient. The H&PCOs selected are largely acknowledged by peers as high quality providers. They are all located in the north-western regions of Italy and they are comparable in terms of size (number of beds and healthcare professionals) and organizational structure. In particular, all the three H&PCOs are not-for-profit organizations and provide both home-based and hospice-based care. Health professionals rotate continuously between the two types of services to promote knowledge and best practices sharing. This allowed data collected from each H&PCO to be pooled in a single dataset.
The survey was conducted from January to March 2010 by means of a self-compiled questionnaire. Professionals involved in the research included physicians, psychologists, physiotherapists, nurses and other healthcare operators. Administrative staff were not included in our survey since they do not participate in H&PCO core activities. We thus identified a total of 226 professionals to whom the questionnaires were subsequently delivered. 148 questionnaires were returned, but 13 were considered unusable and thus discarded, resulting in a 65% response rate.
3.2 Measures
Measures for our study were crafted by referring to the core conceptual attributes developed by prior research. Specifically for the measures related to the theory of planned behaviour, we followed [31]‘s recommendations and conducted a series of face-to-face interviews with personnel from one of the organizations involved to elicit the behavioural, normative and control beliefs of respondents. This allowed us to enhance our understanding of the context in which the constructs were being investigated and refine the wording of our questions.
We pilot-tested our measures with 48 individuals from the same organization to test the clarity of the questions and to assess the ability of scales in capturing the desired information. Feedback from the pilot-test was used to refine and modify the scales.
The final questionnaire included nine scales, for a total of 38 items measured on a 7-point Likert scale anchored at 1 (I totally disagree) and 7 (I totally agree).
3.2.1 Intellectual Capital Constructs
Scales measuring intellectual capital dimensions were drawn from existing literature. Human capital (HC) and organizational capital (OC) were measured drawing from [8]. The four items of the scale for human capital were used to measure the extent to which an individual perceives the stock of knowledge and knowing capability of his/her professional practice of reference. On the other hand, social capital was measured using eight items gauging the degree to which an individual perceives the overall pattern of connections of his/her network of relations and the quality of his/her personal relationships [8,8]. In doing so, we captured two important dimensions of social capital described in the literature, namely structural social capital (SSC) and affective social capital (ASC) [10,10].
3.2.2 Theory of Planned Behaviour Constructs
Constructs included in the theoretical framework of TPB were drawn from previous literature and adapted to the context under study. In particular, the four items measuring knowledge sharing behaviour (KSB) were adapted from [42] to measure the extent to which individuals engage in knowledge sharing activities in different work-related situations. Knowledge sharing intention (INT) scale was crafted drawing from [43]. The four items of the scale measure the intentional disposition of an individual to effectively and frequently share knowledge with co-workers. Moving to subjective norm (SN), the construct was measured by referring to [44]. The resulting scale comprises four items capturing the extent to which an individual believes she is expected by relevant co-workers to share knowledge and her perception of the extent to which these co-workers engage in such activity.
According to [43], the organizational dimension is one of the factors affecting the transfer of knowledge within organizational units. In our study, we followed their arguments and framed the scale measuring perceived behavioural control (PBC) to capture an individual's control over knowledge sharing as a function of organizational climate. The four items for organizational PBC were adapted from [43] and capture an individual's control over knowledge sharing as a function of organizational climate.
3.2.3 Innovative Work Behaviour Constructs
As illustrated in the conceptual model, our study investigates innovative behaviour (IWB) as a potential outcome of knowledge sharing behaviour. To assess this construct we crafted our scale drawing from [17]. The resulting four-item measure captures how frequently individuals engage in micro innovations to improve their job routine.
3.2.4 Control Variables
We included control variables, namely: age, gender, professional experience, professional experience within the specific H&PCO (both measured as the natural logarithm of years) and professional role (physician, psychologist, physiotherapist, nurse – measured as dummy variables).
3.3 Analytical Procedure
Data analysis comprised two consecutive stages. First we screened the collected data and discarded unusable questionnaires. This reduced the number of usable questionnaires to 135. The data collected were also screened for univariate and multivariate normality. Results indicate a general moderate level of skewness (maximum observed skewness: –2.39) and kurtosis (maximum observed kurtosis: 7.07). Additionally, the assumption of multivariate normality was not met (p < .01).
We then proceeded with the evaluation of the model. Given our sample size and the fact that assumptions regarding indicator distribution for the use of covariance-based SEM were not met, we opted for variance-based SEM [45]. The model was then estimated using the partial least squares (PLS) method [46], which is a variance-based structural equation modelling approach used in previous studies in operations management research and management science, the marketing field and the intellectual capital fields.
The software used for the analyses is SmartPLS 2.0 [47]. PLS is primarily intended for causal-predictive analysis and is considered better suited for explaining complex relationships [48]. As stated by Wold [46]: “PLS comes to the fore in larger models, when the importance shifts from individual variables and parameters to packages of variables and aggregate parameters”(p. 589). Wold states later (p. 590): “In large, complex models with latent variables PLS is virtually without competition”.
4. Results
4.1 Measurement Model
To assess construct reliability we calculated the composite reliability coefficients. All coefficients are higher than .80, thus providing reliability to all the scales adopted [49] (Table 1).
Composite Reliability (CR) and Discriminant Validity

N = 135. On the diagonal the square root of the AVE.
In order to consider convergent and discriminant validity of the constructs using the PLS approach, it is necessary to follow these criteria [50]: a) indicators load much higher on their hypothesized factor than on other factors (own loadings are higher than cross loadings); b) the square root of each factor's average variance extracted (AVE) is larger than its correlations with other factors. To satisfy the first criterion we used the PLS confirmatory factor analysis procedure proposed by [51]. All the items loaded well on their respective factors (see Table 2), which are much higher than cross loadings (omitted for brevity). The items of social capital loaded on two factors that, coherently with [10,10], we named as structural dimension and affective dimension of social capital.
Factor Loadings

Relative to the second criterion, Table 1 shows that the square root of all the AVEs is larger than all other cross correlations. Jointly, these findings suggest adequate convergent and discriminant validity.
To overcome the concern of common method bias in the survey design, we first included some reverse-scored items in the principal constructs to reduce acquiescence problems [52]. Subsequently, common method variance was assessed after the data were collected using Harman's one-factor test [53]. In this test, all the principal components are entered into a principal components factor analysis. Evidence for common method bias exists when a single factor emerges from the analysis or when one general factor accounts for the majority of the covariance in the interdependent and dependent. As each of the principal constructs explains roughly equal variance, the data do not indicate substantial common method bias.
4.1 Hypotheses Test
Figure 2 shows the standardized PLS path coefficients. The control variables used in this study do not show significant relations, and are therefore not shown in the figure. To assess the statistical significance of the path coefficients, which are standardized betas, a bootstrap analysis was performed. The use of this as opposed to traditional t-tests allowed the testing of the significance of parameter estimates from data that were not assumed to be multivariate normal. Table 3 summarizes our results by referring to the proposed hypotheses.
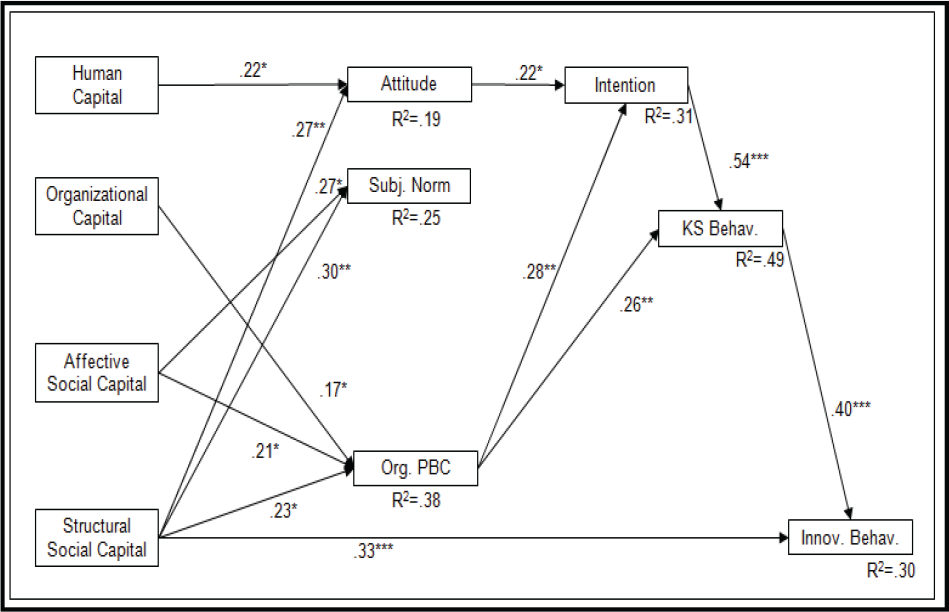
Results of the Structural Equations Model
Standardized PLS Coefficients
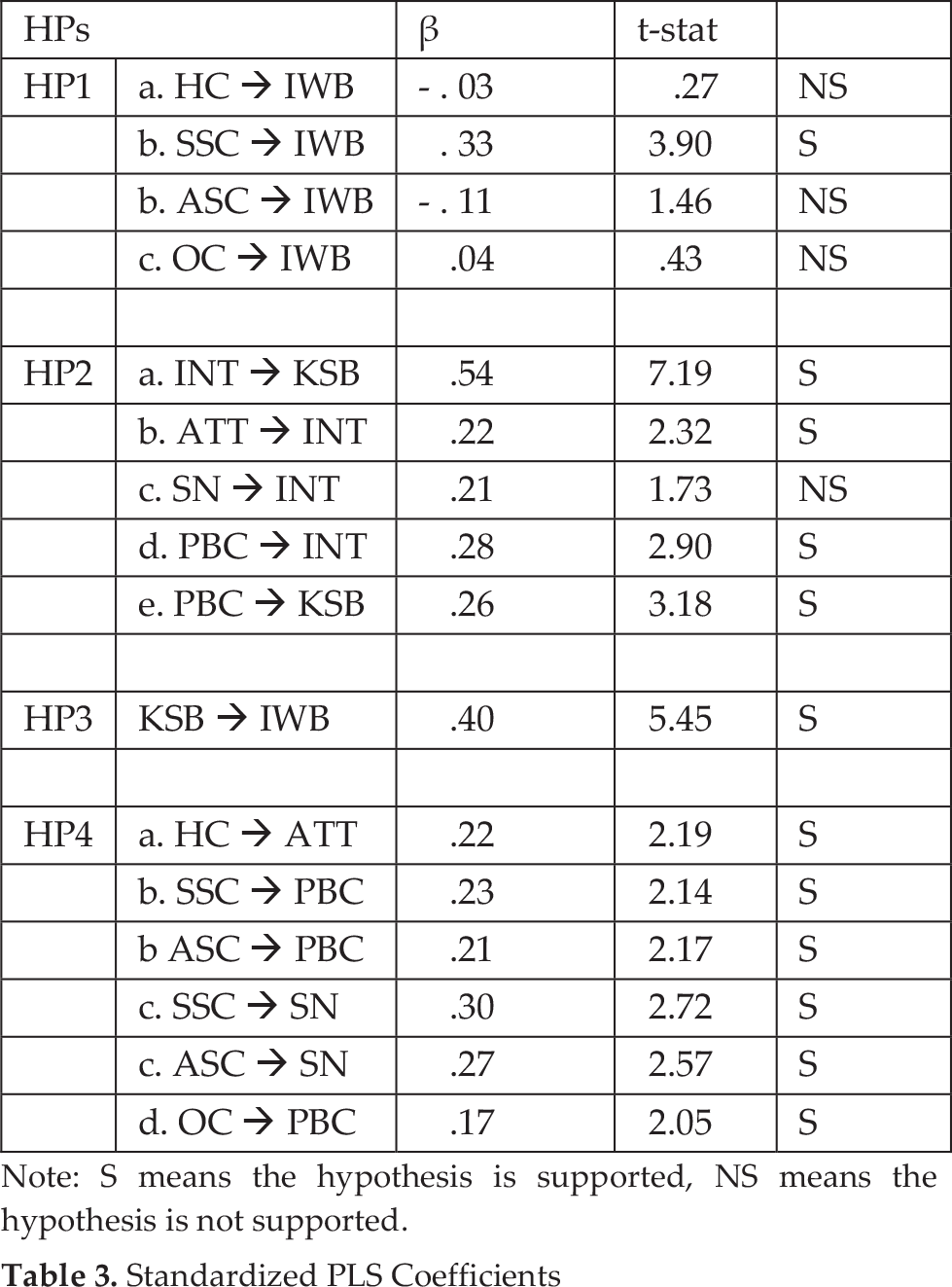
Note: S means the hypothesis is supported, NS means the hypothesis is not supported.
With regard to our first set of hypotheses based on the rationale that practitioners' perception of the intellectual capital of the organization positively influence their innovative behaviour, we found that human capital does not significantly affect innovative work behaviour directly (β = - .03, p > 0.05), therefore not providing support for Hypothesis 1a. Also, Hypothesis 1b suggesting a positive effect of social capital on innovative behaviour receive mixed support. While the structural component of social capital significantly affect innovative behaviour (β = .33, p < 0.001), the affective component does not (β = - .11, p > 0.05). Finally, organizational capital does not significantly affect innovative behaviour (β = .04, p > 0.05) providing no support for Hypothesis 1c. Hypothesis 2 that suggests a positive effect of knowledge sharing on practitioners' innovative behaviour, finds empirical support (β = .40, p < 0.001), thus confirming the relevance of knowledge sharing on individuals' innovation processes.
With regard to our hypotheses related to the theory of planned behaviour, our findings provide a support to all expected links with the exception of the relationship between subjective norm and intention to share knowledge that results to be significant at p = 0.08 (β = .21), thus not fully supporting Hypothesis 3c.
With regards to our fourth set of hypotheses that suggests a relation between intellectual capital and the antecedents of knowledge sharing behaviour, we find human capital to positively affect attitude towards knowledge sharing (β = .22, p < 0.05), thus supporting Hypothesis 4a. Both components of social capital (structural and affective) significantly affect perceived behavioural control (β = .23, p < 0.05; β = .21, p < 0.05), and subjective norm (β = .30, p < 0.01; β = .27, p < 0.05), therefore providing support for Hypothesis 4b and Hypothesis 4c. Finally, organizational capital positively influence perceived behavioural control (β = .17, p < 0.05) providing support for our Hypothesis 4d.
In conclusion, we highlight the high degree of explained variance in the two endogenous constructs knowledge sharing behaviour (R2 = .49) and innovative work behaviour (R2 = .30). Overall, our results partially support a direct effect of intellectual capital on practitioners' innovative work behaviour, as a matter of fact, the structural dimension of social capital exclusively directly affects innovative behaviour. However, our findings suggest that intellectual capital positively affects practitioners' innovative behaviour by means of the mediating role played by knowledge sharing behaviour and its antecedents.
5. Conclusions
Our research aimed at investigating the role of intellectual capital in promoting innovative behaviours among health practitioners. This issue has not attracted much attention over the years, but it is fundamental to understand organizational innovation since new knowledge always begins with individual [11]. This research has four main results that produce significant implications for theory and practice.
First, we found out that the relation between intellectual capital and innovative work behaviour is not straightforward but mediated by knowledge sharing. Then, we needed to explore the mechanisms through which the organizational wealth represented by intellectual capital actually affects individuals' willingness to generate new knowledge and introduce new ideas. Our research offers empirical support to previous insights suggesting that a significant mechanism is knowledge management because it translates the organizational potential of intellectual capital into individual efforts [21]. Indeed, we also found a direct path linking structural social capital and innovative behaviour. This result has relevant implications for hospital managers because it highlights the need to develop strong networks of relations between practitioners. This is coherent with previous contributions that posit innovative behaviour as a composite function which requires specific abilities to recognize opportunities to change and to find external support for the new idea. These requirements need innovators to be embedded into a rich network of acquaintances to gain access to external stimuli and promote initiatives.
Second, we explored the relation between intellectual capital and knowledge sharing behaviour. We found out that intellectual capital does not directly affect knowledge sharing behaviour, but its antecedents, attitude, subjective norms and perceived behavioural control. This result is coherent with our expectations that an increase of knowledge stocks (that is, intellectual capital) does not directly translate into knowledge sharing, but needs to mediated by practitioners' willingness to act upon it [26]. The main implication of this finding is that the centrality of practitioners' behaviour does not emerge only in the final act of generating new ideas but in the entire process of individual innovation. Understanding practitioners' nature and the social context that shape their perceptions, then, is a fundamental need for hospital managers before adopting any interventions. Accordingly, our third set of results related to a better understanding of the factors affecting practitioners' willingness to share knowledge. The present results are intriguing because they identify attitude and perceived organizational control as the two major drivers of practitioners' intention to share.
According to our findings, then, hospital managers should devote more time to (a) improving practitioners' perception of a causal and direct linkage between knowledge sharing efforts and clinical improvements; (b) building a facilitating organizational context. Our results show that strategies affecting the perception of control are the most significant antecedent of both knowledge sharing intention and behaviour.
Also, we investigated how intellectual capital contributes in improving practitioners' attitude and perception of control. We observed two distinct patterns linking: (a) human capital to attitude and (b) organizational and social capital to perceived behavioural control. This is an interesting result because it allows distinguishing two different ways hospital managers should confront practitioners' needs. On one hand, in order to establish positive expectations of future benefits attainable with knowledge sharing (i.e., attitude), hospital managers should facilitate the development of lively and stimulating workgroups which: (a) motivate practitioners into putting extra-efforts to keep up with peers and (b) improve practitioners' perceptions that these extra-efforts will be rewarded.
On the other, hospital managers should facilitate the enactment of knowledge sharing and improve the perception of control over its consequences. Two interventions can be enacted, regarding organizational and social capital. The presence of codified texts is a first facilitator because it allows turning tacit knowledge into explicit knowledge, thus improving its visibility and its ease of use. Even more important is the development of social capital, with a clear distinction between its affective and structural components. Our results confirm the vast literature that posits social capital as a necessary antecedent of knowledge sharing because: (a) affective capital, i.e., the presence of norms of reciprocity and trust, improves practitioners' control over the consequences of knowledge sharing (that is, no opportunistic nor obstructive reactions by the receivers); (b) structural capital, i.e., the presence of strong ties between individuals, multiply the occasions in which individuals get in touch with others and facilitate the transfer of tacit knowledge.
Based on these key results, our research suggests that hospital managers can have a significant impact on knowledge sharing and innovative work behaviour. They are activities that go beyond prescribed work behaviour and mostly represent practitioners' own propensity to initiate new activities. Several contributions detailed how such activities are mostly impossible to mandate or monitor [26] and economical incentives are not effective [43]. Similar results may suggest a limited role for hospital managers in the development of both knowledge sharing and innovative behaviour.
Still, our findings suggest that hospital managers have plenty of room in which to manoeuvre. Specifically, they should address those organizational obstacles that inhibits practitioners' intention to share or the actual possibility to engage in this behaviour. The major leverage appears to be social capital, that is the development of strong networks between practitioners that would allow them to easily communicate new ideas and experiences. This confirms the evidence that hospital managers should work through “softer” approaches regarding the culture and embeddedness of practioners rather than resorting to “hard” approaches such as mandatory requirements or economic incentives.
These findings suggest future directions for our results, namely a further exploration of the perceived behavioural control construct, through the development of an ad hoc measurement scale, and an exploration of the interventions (e.g., team working, intranets) through which hospital managers can impact on social capital.