
Abstract

Despite the increasing options for pharmacologic management of epilepsy, epilepsy surgery remains the best option for many patients with treatment resistant focal epilepsy. Anterior temporal lobectomy (ATL) has been demonstrated to be an effective treatment (1) and is the recommended treatment approach in patients with temporal lobe epilepsy (2). There has been an increasing perception, at least among some epileptologists, that there has been a decline in ATLs for patients with medial temporal lobe epilepsy (MTLE) over the past two decades. A recent study of the use of ATL in a community-based population (3) and a retrospective review of epilepsy surgery cases from nine centers on three continents (4) have demonstrated declines in the use of ATL. For the first question addressed by the Quantitative Practical Use-Driven Learning Survey in Epilepsy (Q-PULSE), panel members were surveyed on their perception of the case types and complexity through a series of six questions.
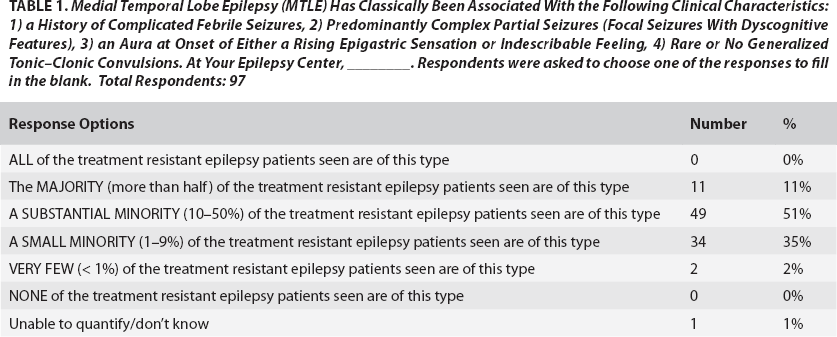
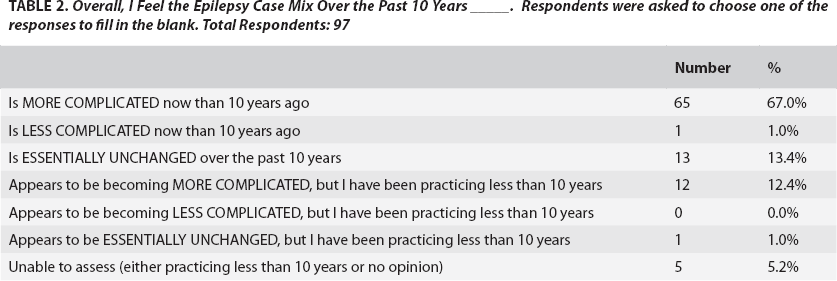
A total of 97 responses were received from the 143 members of the Q-PULSE panel who responded to the initial request to join. Many respondents (40%) have been practicing within their current metropolitan area for more than 15 years (Figure 1). The majority of respondents felt that only 10 to 50 percent of the treatment resistant patients seen in their clinic fit a classic definition of mesial temporal lobe epilepsy (5) (Table 1). The majority of respondents (64%) reported seeing fewer patients with MTLE now than 10 years ago (Figure 2). A majority of respondents (67%) felt that the overall complexity of cases was greater now than 10 years ago (Table 2).

Approximately how long have you been practicing in your current metro area (not necessarily in the same facility)? Total respondents: 97.
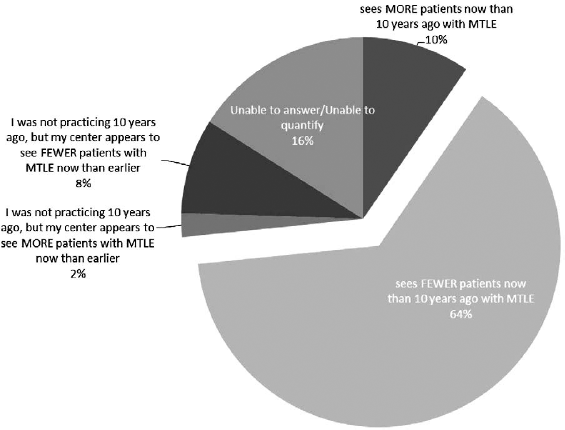
Compared with 10 years ago, my epilepsy center ______. Respondents were asked to choose one of the responses to fill in the blank. Total respondents: 94.
Medial Temporal Lobe Epilepsy (MTLE) Has Classically Been Associated With the Following Clinical Characteristics: 1) a History of Complicated Febrile Seizures, 2) Predominantly Complex Partial Seizures (Focal Seizures With Dyscognitive Features), 3) an Aura at Onset of Either a Rising Epigastric Sensation or Indescribable Feeling, 4) Rare or No Generalized Tonic–Clonic Convulsions. At Your Epilepsy Center, ________. Respondents were asked to choose one of the responses to fill in the blank. Total Respondents: 97
Overall, I Feel the Epilepsy Case Mix Over the Past 10 Years _____. Respondents were asked to choose one of the responses to fill in the blank. Total Respondents: 97
Five potential factors were identified—along with the option of writing in other factors—to explain the observed change, and the panel was asked to rank the factors from 1 to 6 in order of importance (Figure 3). Forty-one percent of respondents identified more patients being managed outside major epilepsy centers as the number one reason for the perceived change, and 24% reported that the primary factor was that the majority of potential “good” surgical candidates have already been offered surgery.
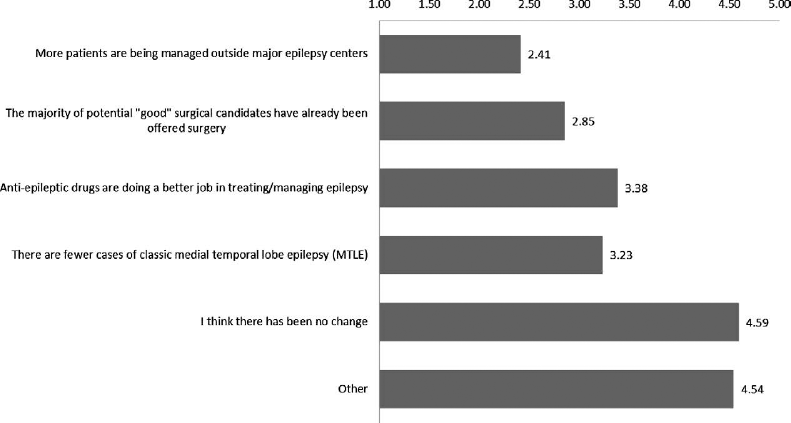
The factors listed above may or may not be contributing to changes in the epilepsy case mix. Please rank them in order (“1” being the most important factor). Total respondents: 96.
Of the 97 respondents, 88 also responded to the demographic survey to allow a more detailed analysis to be undertaken. Of these, 75 characterized themselves as in an academic center versus 13 in private practice, and 64 characterized themselves as practicing in a major metropolitan area (population >1 million) versus a smaller city. There was no difference between either practice area or practice type and whether they reported seeing fewer or more patients with MTLE (Fisher exact for practice type p = 0.6; for practice area p = 0.16).
These survey results demonstrate that there is a broad, but not universal, impression that there are fewer MTLE cases and an overall increase in case complexity seen in epilepsy centers. The data that have been reviewed and presented recently (3, 4) support this opinion. Equally importantly, this was attributed primarily to management outside of the larger epilepsy centers, and only a small number (13.5%) of respondents identified the reason for this perceived change as being fewer cases of MTLE. A shift in where patients are treated, as long as those treatments are leading to seizure control, has very different implications for future diagnostic and therapeutic research compared to a shift in the primary form of treatment resistant epilepsy seen (e.g., from MTLE to neocortical epilepsy). Clearly, additional epidemiologic studies are needed to clarify: 1) whether there are more MTLE cases being treated and managed outside of larger epilepsy centers, 2) whether there are fewer overall cases of MTLE compared to several decades ago, and 3) what clinical features or findings led to the perception of increased case complexity within epilepsy centers.
Disclaimer: The results of the Q-PULSE survey presented here represent the aggregate survey responses of epileptologists. The data assess the opinions and/or approaches to clinical issues in epilepsy care. These data are not derived from a formal clinical or scientific trial. Q-PULSE survey results should not substitute for existing clinical evidence and clinical judgment in patient care and do not represent a practice parameter or practice recommendation.