
Abstract
Purpose
Video-assisted thoracoscopic surgery (VATS) lobectomy has become an accepted procedure for the treatment of selected cases of lung cancer. The aim of this project was to establish national practical recommendations for the management of patients suitable for VATS lobectomy.
Methods
The Scientific Committee of the VATS Lobectomy Group (a branch of the Italian Society of Thoracic Surgery) identified the consensus conference as an appropriate tool for a national debate. The consensus conference was organized following indications of the Italian Department of Health: a panel of experts reviewed the literature, the jury board revised the experts’ reports, and the national conference discussed and voted on statements. The strength of recommendation for a statement was classified as weak, fair, or high when the total score ranged between 51% and 67%, 68% and 84%, or 85% and 100%, respectively.
Results
Eighty-six Italian thoracic surgeons attended the 1st Italian Consensus Conference on VATS lobectomy in Giulianova, Italy, on October 29-30, 2015. Thirty-three topics were discussed: indications, surgical strategy, perioperative management, and training were the main topics. Consensus was reached on 24 statements that were consequently recommended.
Conclusions
The Italian Consensus Conference is the first attempt to discuss VATS lobectomy-related issues in a national scientific community. Such experience determined an improvement in epistemic knowledge among the Italian thoracic surgeons and could be a suggestion for other national communities.
Introduction
The first video-assisted thoracoscopic surgery (VATS) lobectomy was reported by Roviaro et al (1) in 1992, when a 71-year-old man underwent a right lower lobectomy for a lung adenocarcinoma in Milan, Italy. A few years later, Robert McKenna Jr. (2), reporting his experience with 45 patients with clinical stage I non-small-cell lung cancer (NSCLC), greatly contributed to the VATS lobectomy diffusion. During the following 2 decades, the VATS lobectomy significantly evolved and gradually increased in acceptance. However, because of concerns regarding oncologic and surgical safety, its use has been limited to selected centers. Potential reasons for this include a nonuniformly standardized technique, the chance to achieve a radical resection, adequacy of lymphadenectomy, and its impact in terms of long-term survival for oncologic patients. Although the VATS lobectomy supporters emphasized several potential advantages, such as reduced morbidity, hospital stay, and costs, and similar survival rates, evidence in the scientific literature remained weak and limited to case series, observational studies, and meta-analyses deprived of large randomized controlled trials.
Hip replacement surgery was the focus of the first European consensus conference organized by Swedish orthopedics in 1982; the core of this conference was an open debate where the collective understanding of innovative technologies produced democratic statements on a critical issue. Starting from the early 1980s, consensus conference activity significantly increased worldwide, with focus on new medical technologies. One of the most important factors of a consensus conference is considered the type of procedure, given that the method itself legitimates the achieved statements among a national medical community.
The aim of the Italian thoracic surgeons VATS group meeting presented in this article was to provide a consensus document on management of VATS lobectomy patients.
Methods
The Italian Society of Thoracic Surgery endorsed the VATS Lobectomy Group (a branch of the national society) to produce a consensus document on the VATS lobectomy procedure as practiced in Italy. The VATS Lobectomy Group scientific committee identified experts (12 surgeons), the jury (52 surgeons), the date, and the location for the consensus conference.
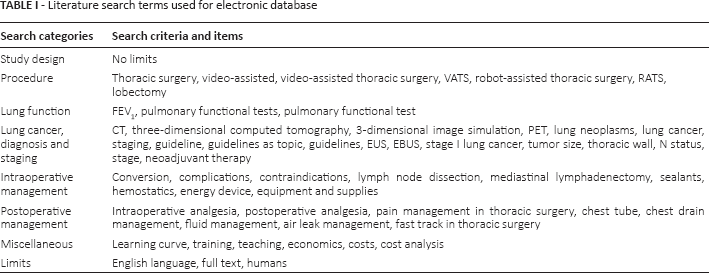
The Experts were divided into different working groups with the following topics: eligibility, lymphadenectomy and conversion, technical instruments, perioperative management, and training. The experts performed a systematic literature search on Medline/PubMed (National Library of Medicine) to obtain a comprehensive number of scientific articles limiting the results between January 1, 1995, and October 1, 2015; search terms and limits are detailed in Table I.
Literature search terms used for electronic database
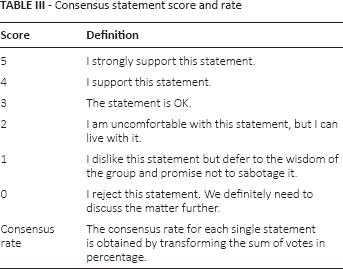
A total of 761 peer-reviewed and full-text articles were extracted from the National Center for Biotechnology Information PubMed database; 580 articles were considered not pertinent because they did not match the topics. A preliminary list of the remaining selected 181 with details of the reference in extent and a summary in English language was made available for all the members of the jury and experts 2 months in advance. Each article was also scored by the experts with a preliminary comment on the level of evidence (Tab. II) (3). In this preliminary document, experts proposed statements for the conference. The preliminary document was circulated among jury members for statement correction; recommendations based on the literature were assigned according to the US Preventive Services Task Force classification. The consensus conference was held in Giulianova, Italy, on October 29-30, 2015: the experts summarized the literature review, as resulted in the preliminary document after the jury revision, followed by questions and statements. Eighty-six delegates from 62 Italian thoracic surgery units discussed the statements, which could be directly modified according to the debates; the audience expressed its consensus by an anonymous voting system (Tab. III). The final document was reviewed by the jury and the main recommendations derived from the consensus conference were tabulated; an abstract was submitted to the Italian National Institute of Health for publication on its Diagnostic-therapeutic Paths website.
Levels of evidence
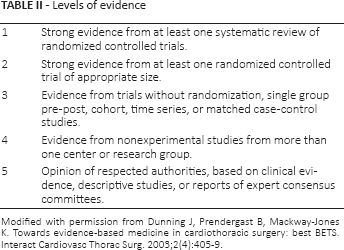
Modified with permission from Dunning J, Prendergast B, Mackway-Jones K. Towards evidence-based medicine in cardiothoracic surgery: best BETS. Interact Cardiovasc Thorac Surg. 2003;2(4):405-9.
Consensus statement score and rate
Results
Functional eligibility for VATS lobectomy
The Society of Thoracic Surgeons database was retrospectively analyzed by Ceppa and coworkers (4) in 2012. The authors detected a higher rate of pulmonary complications in the open group (21.7% vs 17.8%; p<0.0001); moreover, as the predicted postoperative FEV1 (ppoFEV1) decreased, the pulmonary complication rate increased in both groups, but the patients with open procedures and ppoFEV1 less than 60% had more pulmonary complications (p = 0.023). In 2013, Oparka and coworkers (5) published a comprehensive review specifically addressed to inquire into VATS lobectomy as an alternative to the open procedure in patients with limited pulmonary function. The authors selected 7 articles (including the article mentioned above) that collected 13,600 patients. The review concluded that VATS lobectomy resulted in a better outcome in patients with poor pulmonary function. These results were confirmed by Burt et al (6), who presented at the 93rd annual meeting of The American Association for Thoracic Surgery (Minneapolis, Minnesota, May 4-8, 2013) the analysis of 13,376 patients enrolled in the Society of Thoracic Surgeons General Thoracic database from 2009 to 2011. The authors found that a decreased predicted postoperative diffusing capacity for carbon monoxide (ppoDLCO) was an independent predictor for cardiopulmonary complications and mortality in multivariate analyses; a decreased ppoFEV1 was a predictor of complications in the open and in the VATS group, while mortality was correlated only in the open group. In addition, the authors performed 1:1 propensity matching analysis including 4,215 patients in each group: patients with ppoFEV1 <40% and open procedure had greater mortality than the propensity-matched patients who received a VATS lobectomy (4.8% vs 0.7%; p = 0.003). Similarly, the rate of cardiopulmonary complications was higher in patients with open lobectomy (21.7% vs 12.8%; p = 0.005). Finally, patients with ppoDLCO <40% and open procedure had greater mortality than matched VATS patients (5.2% vs 2.0%; p = 0.003). Additional confirmation arose from a Korean study that used propensity match analysis to validate the hypothesis that VATS lobectomy can decrease the postoperative pulmonary complication rate compared with the open procedure in patients with chronic obstructive pulmonary disease (7). The VATS group had lower postoperative pulmonary complications (1.1% vs 12.1%; p<0.01) and lower postoperative pneumonia (1.1% vs 11.0%; p = 0.01).
Preoperative mediastinal staging and VATS lobectomy
Medline search for “preoperative mediastinal staging and VATS lobectomy” did not return any specific result. There is no reason to consider that VATS lobectomy requires a different staging from open lobectomy; therefore, the European Society of Thoracic Surgeons (ESTS) guideline should be considered.
The 2014 revision of the ESTS guideline for preoperative mediastinal lymph node staging considers computed tomography (CT) and positron emission tomography (PET) the starting point for mediastinal staging. When CT and/or PET scan identify positive lymph nodes, the tissue confirmation is indicated by endobronchial ultrasound (EBUS) and/or endoscopic ultrasound (EUS) fine-needle biopsy. If negative, mediastinoscopy is indicated. Tissue confirmation is also indicated when CT and/or PET scan are negative on the mediastinum but hilar positive nodes are suspected or the tumor is larger than 3 cm or located close to the hilar structure (8).
Video-assisted thoracoscopic surgery lobectomy and lymph nodal status
In 2009, Yan and coworkers (9) published a systematic review and meta-analysis on safety and efficacy of VATS lobectomy for early-stage NSCLC. The meta-analysis considered the reported incidence of morbidity, perioperative mortality, recurrence, and 5-year mortality. The incidence of prolonged air leak (10 studies), arrhythmia (8 studies), pneumonia (6 studies), and perioperative mortality (13 studies) were similar between the 2 arms. Heterogeneity among the studies was found in length of hospital stay, chest tube time, blood loss, and operation time; therefore no indication could be drawn. The meta-analysis established that there was no difference in loco-regional recurrence between the 2 techniques (6 studies) but distant recurrences were more frequent in the open arm (Relative Risk (RR) = 0.57, p = 0.03; 5 studies). Finally, 5-year survival was better for the VATS arm (RR = 0.72, p = 0.04; 7 studies).
Two years after the publication by Yan et al. Korean researchers published a 1:1 propensity-matched study that considered 270 patients with stage I NSCLC (10). No statistical differences in postoperative complications were found between the 2 groups, but the VATS group had a significantly shorter hospital stay (p<0.05). There was no significant 3-year disease-free survival difference between the VATS and open group (85.3% vs 81.8%); similarly, the overall 3-year survival was comparable (96.6% vs 97.4%). Li and colleagues published a meta-analysis of long-term outcome after VATS or open lobectomy for stage I NSCLC in 2012 (11). Out of 213 articles, the authors selected 9 studies that included 1,362 patients; of the selected studies, only 1 was a randomized controlled trial. Five-year survival rate in the VATS group was 87.8% versus 80.2% in the open group (odds ratio 2.01, 95% confidence interval 1.44-2.78; p<0.0001).
Notwithstanding meta-analyses including studies with low level of evidence except for few small randomized trials, the third edition of the American College of Chest Physicians evidence-based clinical practice guidelines stated that VATS lobectomy is preferred over an open surgery for anatomic pulmonary resection in patients with clinical stage I NSCLC (12).
Video-assisted thoracoscopic surgery lobectomy and tumor size
In 2001, Solaini and coworkers (13) published their experience in VATS lobectomy (from 1993 to 1999) including the learning curve. The tumor size was intentionally limited to 4 cm; the authors reported a conversion rate of 10.4% but tumor size was not included among causes. Bu and colleagues (14) directly addressed the problem of a tumor larger than 5 cm in their study published in 2012. This retrospective cohort study included 46 patients treated with VATS lobectomy and 87 patients with open procedure. The 2 groups were similar in complications, lymph node dissected, drainage duration, and length of stay; operation time and amount of blood loss were significantly better in the VATS group. Disease-free interval and 3-year survival were comparable between the 2 groups.
A retrospective review of an institutional, prospective database was performed by Villamizar and colleagues in 2013 (15). Out of 916 patients who received VATS lobectomy, 296 had tumor larger than 3 cm. Univariate analysis identified tumor size >3 cm, central tumors, or clinically positive nodes as factors for increased morbidity, but multivariate analysis did not confirm tumor size as a significant risk factors for overall morbidity. The authors also stratified the patients on tumor size larger or smaller than 5 cm; the difference in morbidity rate between these groups (40% vs 32%) was not statistically significant.
Video-assisted thoracoscopic surgery lobectomy and T3 (thoracic wall)
In 2012, Berry and colleagues (16) published a review on 105 patients who underwent combined pulmonary and chest wall resection for NSCLC at the Duke University Medical Center between 2000 and 2010. Twelve patients had their operation via a hybrid thoracoscopic approach: the hilar structures were divided using VATS techniques; therefore, a limited counterincision was performed over the area of planned chest wall resection, the ribs were sectioned, and the sample retrieved via the counterincision avoiding any rib spreading. The open and the VATS groups have the same tumor size (5.4 ± 2.5 cm vs 5.6 ± 2.6 cm) and similar number of resected ribs. Thirty-four patients (37%) in the open group had resections of a Pancoast tumor, while 2 patients (17%) belonging to the VATS group had such an operation. Postoperative outcomes were similar between the 2 groups in terms of overall morbidity (VATS 42% vs open 59%; p = 0.32) and mortality (VATS 0% vs open 3.2%); the VATS group had a shorter length of stay (VATS 5.5 vs open 6 days; p = 0.03). Good outcomes achieved by the authors demonstrated that the hybrid approach to NSCLC infiltrating the thoracic wall could be performed in specialized centers.
Hybrid procedures were also proposed for the treatment of Pancoast tumors: VATS lobectomy combined with anterior approach to the apex has been described by some authors (17-18-19) and 2 articles reported VATS lobectomy combined with a posterior approach (16, 20). These reports only demonstrated the feasibility of hybrid approaches to Pancoast tumors, but it is possible that properly selected patients could receive a complex operation via minimally invasive access with potential benefit in experienced surgical centers.
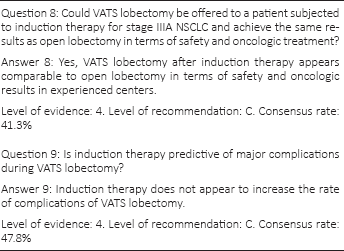
Video-assisted thoracoscopic surgery lobectomy and induction therapy
Concerns regarding surgical hilar dissection in patients who have undergone induction therapy were reported by Duke University Medical Center researchers with a retrospective study published in 2006 (21). The authors analyzed 97 consecutive patients treated between January 1, 1996, and July 1, 2005; among those patients, 12 received their lobectomy via a thoracoscopic biportal procedure. Patients who received VATS lobectomy had shorter length of stay (3.5 vs 5 days; p = 0.0024). There were no differences in major complications or operative mortality; in addition, disease-free survival and overall survival were similar between the 2 groups. The authors were aware of limitations of their study and suggested studying each patient carefully, eventually with a thoracoscopic inspection, before starting with the VATS lobectomy. In 2014, Gonzales-Rivas et al (22) reported a retrospective study that included 87 patients with early-stage NSCLC and 43 patients with advanced stage NSCLC; among them, 29 received induction therapies. The neoadjuvant cohort was not analyzed separately and a variety of surgical interventions were applied through the uniportal access. Despite this inhomogeneity, postoperative stay in the intensive care unit, length of hospital stay, and morbidity were similar between the 2 groups. Augustin and coworkers (23) published a retrospective study on 232 patients treated with anatomical VATS resections from 2009 to 2012; conversion to open surgery was the endpoint. The conversion rate was 6.5%; induction therapy (p = 0.013) as well as tumor size (p = 0.04) were independent risk factors for conversion in the multivariate analysis. Except for the length of hospital stay (11 vs 9 days; p = 0.028), there were no differences between converted and nonconverted patients in terms of drainage duration, morbidity, or mortality.
Woodard and Jablons (24) published a comprehensive nonsystematic review of surgical management of stage IIIA NSCLC in 2015. On the VATS-specific topic, the authors concluded that, lacking any randomized controlled trials, it is diffıcult to make appropriate statements on VATS versus open surgery in stage IIIa NSCLC. Nevertheless, it is possible that the VATS approach could offer a less invasive alternative to open surgery in experienced centers.
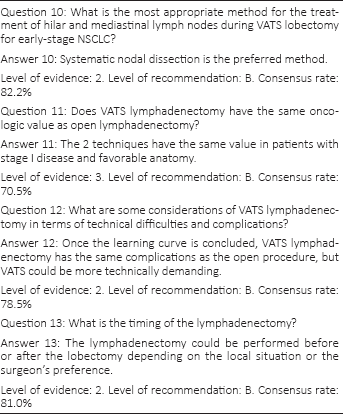
Video-assisted thoracoscopic surgery lobectomy and intraoperative lymph node staging
There is a general agreement that intraoperative nodal staging of NSCLC should be accurate; notwithstanding, the degree of mediastinal lymph node assessment during surgery is debated. Systematic nodal dissection (SND) improves nodal staging and offers better local control, removing possible micrometastases; mediastinal lymph node sampling (MLS) is associated with shorter operating time, reduced bleeding, and decreased risk of damage to mediastinal structures (25). Zhong and colleagues (26) published a comprehensive review that included several randomized and nonrandomized trials in 2008; this review pointed out weak scientific evidence that supported both techniques. Moreover, survival benefit could not be associated with any of the surgical techniques for mediastinal staging. The ESTS guidelines for intraoperative lymph node staging in NSCLC recommended systematic nodal dissection in all cases by an en bloc resection where possible. Those guidelines allowed specific exceptions for peripheral squamous T1 cancers, high-risk patients, and subjects who received induction therapy: in those cases, lobar-specific lymph node dissection is acceptable (27). The American College of Chest Physicians guidelines are more liberal recommending SND or MLS in patients undergoing resection for stage I and II NSCLC; additional extensive mediastinal dissection is not suggested for patients with clinical stage I NSCLC who have undergone SND showing intraoperative N0 status (28).
Watanabe and coworkers (29) published a retrospective study on the feasibility and safety of SND by VATS in 2005. A total of 350 patients were distributed in a VATS group or in an open group. The authors concluded that SND by VATS was not inferior to that by open thoracotomy in the number of dissected lymph nodes. In 2011, D'Amico and colleagues (30) published a similar retrospective study, which analyzed the National Comprehensive Cancer Network's NSCLC Database to compare the effectiveness of mediastinal lymph node dissection during VATS or open lobectomy. Considering the number of lymph node stations harvested, there was no difference in the value of dissection by approach. A possible alternative way to assess the completeness of lymph node dissection is the check for nodal upstaging; such analysis was published by Licht and coworkers in 2013 (31). The authors analyzed 1,513 patients enrolled in the Danish Lung Cancer Registry and detected a nodal upstaging rate of 18.6%; the upstaging for N1 was significantly higher after thoracotomy (13.1% vs 8.1%; p<0.001), and a similar result was obtained for N2 upstaging (11.5% vs 3.8%; p<0.001). However, multivariate survival analysis showed no difference in survival. A larger retrospective study was published by Boffa and colleagues (32) in 2012. The review considered 11,500 patients enrolled in the Society of Thoracic Surgery database; upstaging from N0 to N2 was similar between VATS and open surgery (4.9% and 5.0, respectively; p = 0.52). Upstaging from N0 to N1 was less frequent in the VATS group (6.7% versus 9.3%; p<0.001); this result was probably related to the enrollment bias connected to learning curves, because VATS-predominant surgeons identified a comparable number of occult nodal metastases in VATS as in open surgery.
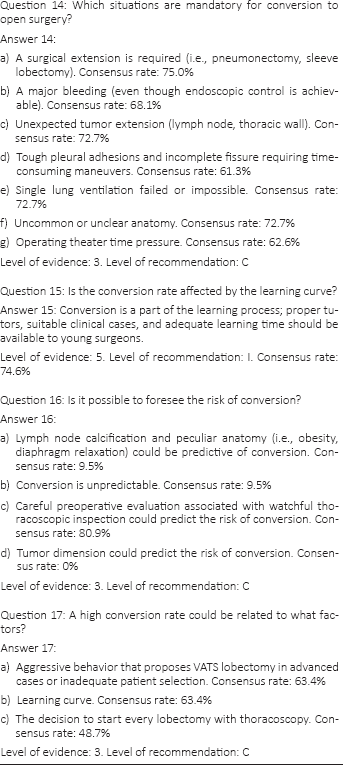
Video-assisted thoracoscopic surgery lobectomy and conversion to open surgery
In 2008, Solaini and colleagues (33) published a review of their experience with VATS including a variety of procedures. The study comprised 1,615 patients with 10.8% conversion rate; the authors stressed the opportunity to convert VATS to open surgery when patient safety was at risk. A classification of causes determining VATS lobectomy conversions was proposed by Gazala (34) in 2011. The classification, named VALT open, separated causes of conversion into vascular complications, anatomy reasons, lymph node difficulties, and technical problems. Catastrophic intraoperative complications during VATS lobectomy are also possible; Flores et al (35) presented an institutional review at the 91st meeting of The American Association for Thoracic Surgery in 2011. The authors defined catastrophic complication as an incident that results in a supplementary unexpected major surgical procedure; those dramatic complications occurred in 11 patients (1.7%) out of 633 VATS lobectomies analyzed.
A review from the Duke University Medical Center, published in 2013, underlined that the conversion rate reported in the scientific literature ranged from 2% to 23%; the rate diminished as the surgeons increased their experience (36). The authors reported their concerns with the possible morbidity and mortality increased risks in patients who undergo conversion, even though some studies described no extra danger in converted patients. Samson and coauthors (37) published a score based on lymph node calcification and positively correlated the score to their conversion rate (45 patients out of 193). The authors reported higher 30-day mortality, augmented blood loss, additional arrhythmias, longer operative time, as well as increased length of hospital stay in converted versus nonconverted patients. The morbidity and mortality rate of converted patients were similar to those undergoing planned open surgery, but the length of hospital stay was longer. Recently, the Barnes Jewish Hospital in St. Louis, Missouri, published an institutional review of patients undergoing lobectomy (38). A total of 623 patients received a planned open surgery; 604 patients had an attempted VATS procedure and 87 were converted (14.4%). During the study period, the conversion rate was related to the learning curve, considering that the rate fell from 28% in the early period to 11% in the last period. Emergent procedures occurred in 23% of the patients, requiring conversion. According to the mentioned classification, 25% of the conversions were related to vascular causes, 64% were for anatomic reasons, 9% were for lymph nodes, and 1% was associated to a technical failure of equipment. Except for male sex, no other patient characteristics or imaging issues predicted the probability of conversion. The postoperative complications rate was higher in the conversion group than in the VATS group (46 vs 23%) but the former was comparable to the open surgery group (42%); long-term survival was not affected by conversion.
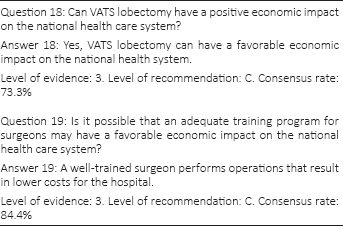
Video-assisted thoracoscopic surgery lobectomy and cost analysis
In 1998, Japanese researchers first reported a cost analysis for VATS lobectomy; the conclusion indicated higher cost for thoracoscopic versus open lobectomies (39). As experience increased and the cost analysis improved, it became evident that VATS lobectomy could be economically profitable. Casali and Walker (40) published a study on cost analysis referring to 346 patients; a VATS lobectomy cost €8,023, which was less than an open lobectomy (€8,178; p = 0.0002). Swanson and colleagues (41) compared hospital costs for VATS and open lobectomy procedures in the United States; the authors included 3,961 patients and confirmed that hospital costs were greater for open surgery versus thoracoscopy; $21,016 versus $20,316 (p = 0.027). In addition, a correlation between the surgeon's experience with VATS lobectomy and cost has been found: the cost for low-volume surgeons was $22,050 versus $18,133 for high-volume surgeons. More recently, a UK prospective study analyzed 236 VATS lobectomies, fixing the average cost at €11,368; multivariable linear regression and bootstrap analyses identified €4,270 extra cost for patients with DLCO less than 60% (42).
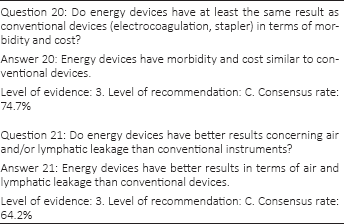
Video-assisted thoracoscopic surgery lobectomy and energy devices
Video-assisted thoracoscopic surgery lobectomy is a procedure widely dependent on technology, such as miniaturized cameras and staplers; energy devices could be useful in this type of surgery and some scientific studies evaluated this possibility.
Kovács and coworkers (43) published an institutional retrospective study on an advanced bipolar device (LigaSure; Covidien, Inc., Norfolk, NE, USA) versus stapler in wedge resection in 2009. The authors analyzed 44 VATS procedures and concluded that the tested energy device was effective and safe for pulmonary wedge resection; in addition, a cost reduction was obtained in the advanced bipolar group versus stapler group. The same instruments were studied by Bertolaccini and colleagues (44) with a prospective randomized trial published in 2014. The study reviewed fissure section during open lobectomy. The authors observed a similar operative time but the energy device group had increased postoperative air leaks (not significant) as well as a larger drainage volume (statistically significant). No difference in length of hospital stay was observed between the advanced bipolar group and the stapler group.
An energy device can also be used for vessel sealing and transection; Toishi and colleagues published a small randomized trial on VATS lobectomy in 2014 (45). A control group (traditional vessel ligation) was compared with a study group (energy device); this group was divided into 3 clusters: advanced bipolar (Enseal; Ethicon, Blue Ash, OH, USA), advanced bipolar (LigaSure; Covidien), and ultrasonic device (Harmonic ACE; Ethicon). Surprisingly, the energy devices were applied after the conventional ligation of the proximal ends of the vessels. The study group had significantly less intraoperative blood loss, surgeon stress, and postoperative drainage volume, and shorter postoperative drainage period. No differences emerged among the clusters.
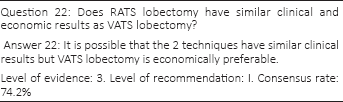
Video-assisted thoracoscopic surgery lobectomy versus robotic assisted lobectomy
A State Inpatient Databases revision was published by Kent and colleagues in 2014 (46); the study included data from 8 US states recorded for 3 years. The collected procedures were lobectomies and segmentectomies performed via open surgery in 20,238 cases, VATS in 12,427, and robotic-assisted thoracic surgery (RATS) in 430 patients. Robotic-assisted thoracic surgery was associated with significant reductions in complication rates (p = 0.003), length of hospital stay (p<0.0001), and mortality (p = 0.016) when compared with open surgery in the propensity-matched analysis. The authors concluded that RATS seems to be a suitable alternative to VATS. Mahieu and coworkers (47) reported an institutional review on VATS versus RATS lobectomy performed during the learning curve; the authors concluded that perioperative outcomes were comparable during the learning period but RATS seems to decrease the conversions rate. On the contrary, Augustin and colleagues (48) published a similar study and concluded that VATS lobectomy had shorter operative times, less blood loss, and lower costs than RATS lobectomy. Recently, Veronesi (49) published a comprehensive literature review that acknowledged that the variety of techniques and instruments used, in addition to the lack of randomized trials, made any conclusion on possible RATS advantages premature. High running costs as well as a large initial investment were the primary limitations to RATS diffusion identified by the author.
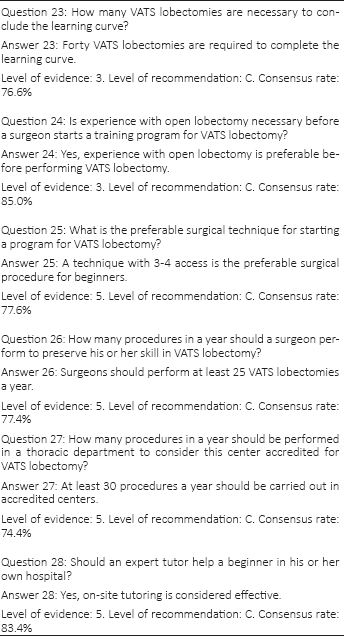
Video-assisted thoracoscopic surgery lobectomy and training
Competence in performing open major thoracic surgery has been considered mandatory before performing VATS lobectomies; nevertheless, with the diffusion of the VATS technique, especially in teaching hospitals, it will be possible that young trainees could learn open and VATS lobectomy simultaneously. The Copenhagen group addressed this issue in an article published in 2012 (50). A single trainee was monitored for 12 months; this prospective study demonstrated that the 29 VATS lobectomies performed by the trainee had the same outcome as the lobectomies completed by an expert surgeon. In 2010, the same authors published a study on the effect of a training program comprising the first 50 VATS lobectomies done by a consultant; 162 VATS lobectomies performed by a well-trained consultant were used as the control group (51). Careful selection of the patients probably justified the better outcomes of the new consultant in terms of air leak, chest tube duration, and length of hospital stay; as expected, the operation time was significantly shorter for the expert consultant.
McKenna (52) considered that the learning curve is concluded after 50 VATS lobectomies, but such a limit has high variability, ranging from 30 to 200 procedures; finally, the specific aptitude of each surgeon should be taken into account (52-53-54).
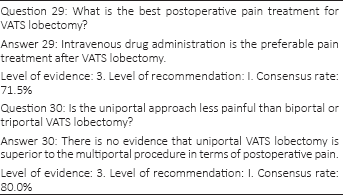
Video-assisted thoracoscopic surgery lobectomy and analgesia
Thoracic epidural analgesia is commonly considered the gold standard for postoperative pain treatment after open thoracic surgery; however, this procedure may be unsuccessful or contraindicated. Paravertebral block is also effective for analgesia in thoracotomy patients; this technique has fewer side effects than epidural analgesia (55). Intercostal nerve block is a simple but less effective regional technique that increases its efficacy when applied as preventive analgesia (56).
Several studies have described a number of analgesic techniques for VATS procedures: thoracic epidural analgesia was compared with intravenous fentanyl and nonsteroidal anti-inflammatory agents in a nonblinded randomized controlled trial; the authors failed to demonstrate differences in pain, analgesic consumption, pulmonary function, satisfaction score, and side effects between groups (57). Another nonblinded randomized controlled trial analyzed thoracic epidural analgesia versus intercostal catheter; no differences in pain scores, supplementary analgesic requests, or adverse effects were found between groups (58). In 2014, a systematic review considered 109 articles on regional analgesia for VATS; among those articles, 17 were selected for analysis. The authors concluded that general recommendations for a gold standard were impossible to be drawn (59).
Some surgeons believe that uniportal VATS lobectomy may result in less postoperative pain versus biportal or triportal procedures. A systematic review, published in 2015, collected 255 articles; among them, 10 articles were analyzed (60). Such articles were relatively small retrospective studies but no randomized trials were found. The authors stated that uniportal VATS have a minor effect on early postoperative pain but further studies are needed to elucidate this point.
Video-assisted thoracoscopic surgery lobectomy and chest tube management
In 2010, Brunelli and coworkers (61) published a randomized trial on a new chest drainage system with a digital continuous recording of air leak. The study group (84 patients with digital device) had a significant reduction in chest tube duration versus the control group (82 patients with traditional chest drainage units). The authors concluded that digital chest drainage provided objective and reproducible data diminishing interobserver variability of air leak evaluation, a key point that could result in delayed chest tube removal. A multicenter international randomized trial, which included a high percentage of patients treated with VATS lobectomy, confirmed that patients managed with digital drainage systems had shorter chest tube permanence and shorter hospital stays compared with those managed with traditional drainage (62).
Bjerregaard and colleagues (63) evaluated the efficacy of chest tube removal after VATS lobectomy with serous pleural drainage up to 500 mL/d. The authors retrospectively analyzed data recorded in a prospective national database including 599 patients in the study. The results of this study suggest that, despite drainage volumes up to 500 mL/day, early chest tube removal after VATS lobectomy is possible and safe. A small proportion of patients required a reintervention for recurrent pleura effusion (2.8%).
Discussion
The VATS Lobectomy Group was founded by members of the Italian Society of Thoracic Surgery in 2013 with the goal of promoting VATS lobectomy across the country, create a national prospective database, and share clinical data for scientific purposes.
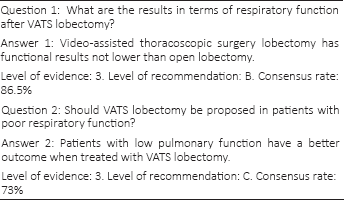
At the completion of 2 years of activity, with more than 2,300 cases enrolled, the scientific committee of the VATS Group promoted a consensus meeting in order to endorse recommendations and national guidelines. A consensus conference seemed to be the most appropriate instrument considering also that the wide range in VATS expertise among members would provide the necessary diversity in backgrounds.
The main recommendations derived from the consensus conference are presented in Table IV; it is immediately evident that the highest consensus grade was achieved by few items. According to the consensus conference, VATS lobectomy is the treatment of choice for clinical stage I NSCLC, even though the recommendation is weak (consensus rate 64.3%). Eligibility for VATS lobectomy should comprise patients with poor respiratory function (recommendation: fair, consensus grade: 73%). There was insufficient agreement among the delegates on the eligibility for patients with tumor of 5 cm or greater, thoracic wall involvement, Pancoast tumor, and induction therapy. Such unsatisfactory agreement suggests that patients with the mentioned conditions should be considered for prospective trials before definitive indication to a minimally invasive approach.
Main recommendations derived from the consensus conference
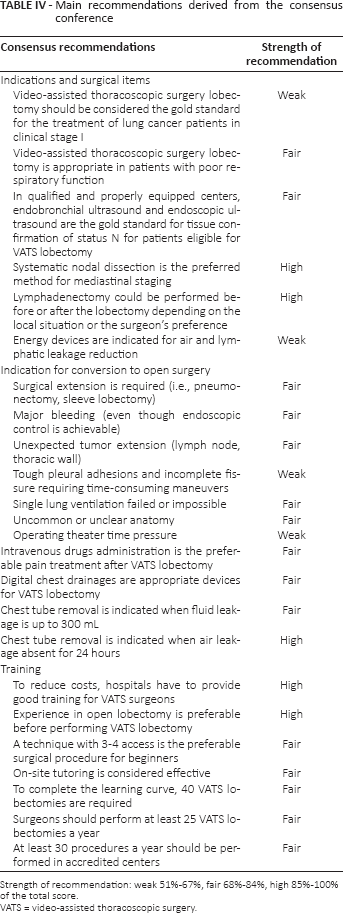
Strength of recommendation: weak 51%-67%, fair 68%-84%, high 85%-100% of the total score.
VATS = video-assisted thoracoscopic surgery.
The consensus conference recommended routine preoperative EBUS/EUS assessment of PET or CT scan positive mediastinal lymph nodes according to ESTS guidelines (recommendation: fair, consensus grade: 73.9%). The conference delegates reached overall agreement on management of lymph nodes: systematic nodal dissection is highly recommended (consensus grade: 82.2%) as well as free timing scheduling for lymphadenectomy (consensus rate: 81%). Sufficient agreement was found on the usefulness of energy device for VATS lobectomy (recommendation: weak, consensus grade: 74.7%). Table IV reports 7 more common indications for conversion judged as relevant; nevertheless, these recommendations should be considered as general rules and delegates believed that the surgeon's experience, personal skill, and local conditions have great influence on the decision to convert to open surgery. The consensus conference reached wide agreement on postoperative management: intravenous analgesia was believed sufficient, considering grade of postoperative pain and short hospital stay (recommendation: fair, consensus grade: 71.5%). The usefulness of digital drainages as well as fluid and air leakage limits for chest tube removal also found a wide agreement among the delegates.
Discussion about training was extensive and general consensus was achieved on the economic impact of a valid teaching program and the need for proficiency in open procedures beforehand (consensus grade: 84.4% and 85%, respectively). Video-assisted thoracoscopic surgery lobectomy with 3-4 port techniques and on-site tutoring in the initial phase of the learning curve were regarded as a sensible approach for beginners (recommendation: fair, consensus grade: 77.6% and 83.4%, respectively). Delegates agreed that 40 VATS lobectomies should be done by a trainee to achieve adequate competence and at least 25 procedures should be performed annually to preserve this technical know-how (recommendation: fair, consensus grade: 76.6% and 77.4%, respectively). Finally, agreement was achieved in determining 30 procedures as the lower limit for centers accredited with the VATS group (recommendation: fair, consensus grade: 74.4%).
An international panel of 55 experts on VATS lobectomy conducted a Delphi conference in 2012 (64). The expert selection was based on a literature search; moreover, several authors who have published in high-impact journals were added. The panel devised 23 consensus statements that can be considered as milestones in VATS lobectomy; the strength of those statements was evident from the absence of significant differences between the 2 rounds of questioning. The 1st Italian Consensus Conference discussed those statements in a real-life, national context; even though the differences between the international and the Italian statement are small, the second derived from an open discussion. The present consensus conference was the first attempt to collect shared recommendations on VATS lobectomy from a national surgical community.
Footnotes
Appendix
Alloisio M., Amore D., Ampollini L., Andreetti C., Aresu G., Argnani D., Baietto G., Bandiera A., Benato C., Bertani A., Bertolaccini L., Bortolotti L., Camplese P., Carbognani P., Cardillo G., Carleo F., Cavallesco G., Curcio C., Dell'Amore D., De Monte L., Denegri A., De Vico A., Di Rienzo G., Divisi D., Dolci GP., Ghisalberti M., Giovanardi M., Gonfiotti A., Gotti G., Imperatori A., Infante M., Lo Faso F., Lopez C., Magnanelli G., Maineri P., Mancuso M., Maniscalco P., Marulli G., Morelli A., Mucilli F., Muriana G., Negri GP., Nicotra S., Palleschi A., Perkmann R., Pernazza F., Poggi C., Puma F., Rinaldo A., Rizzardi G., Roncon A., Rosso L., Rotolo N., Solaini L., Stella F., Terzi A., Torre M., Vinci D., Voltolini L., Zaraca F.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.