
Abstract
A short peripheral intravenous catheter or cannula (PIVC) is frequently used to deliver chemotherapy in oncology practice. Although safe and easy to insert, PIVCs do fail, leading to personal discomfort for patients and adding substantially to treatment costs. As the procedure of peripheral catheterization is invasive, there is a need for greater consistency in the choice, insertion and management of short PIVCs, particularly in the oncology setting where there is a growing trend for patients to receive many different courses of IV treatment over a number of years, sometimes with only short remissions. This article reviews best practice with respect to PIVCs in cancer patients and considers the necessity for bundling these actions. Two care bundles, addressing both insertion and ongoing care and maintenance, are proposed. These have the potential to improve outcomes with the use of short PIVCs for vascular access in oncology practice.
Introduction
A short peripheral intravenous catheter or cannula (PIVC) is a temporary device that is usually inserted in the veins of the forearm (although other sites can be used), to administer intravenous (IV) fluids or medications. Such catheters are commonly used for venous access in most hospital settings.
The insertion of a short PIVC is probably the most widely performed invasive procedure in the acute care setting (1, 2). According to recent studies, 33%-67% of patients have a PIVC inserted during their hospitalization (3–4–5–6).
Short PIVCs are relatively safe and easy to insert. Improvements in technology have resulted in small caliber catheters that can be used for a variety of indications and are suitable to use with a variety of commonly administered medications. Yet studies indicate that the overall IV catheter failure rate (failure before the intended end date of use) lies between 35% and 50% (7–8–9–10).
The most common complications of short PIVCs are phlebitis and dislodgement, which can lead to inflammation and leakage of fluids into the extravascular tissues. If this occurs, the catheter should be removed. Extravasation and or infiltration of some infusates, especially vesicant drugs or those of a hypertonic or irritative nature, can result in tissue necrosis and compartment syndrome (11). PIVC failure may also be the result of catheter occlusion, infusate infiltration in the surrounding tissues, and insertion site or bloodstream infection. Whatever the cause, PIVC failure, by its invasive nature, can lead to personal discomfort for patients and requires additional medical treatment. PIVC failure is costly to health-care systems, due to the increase in need for medical resources and patient's additional length of hospital stay.
The incidence of local or bloodstream infections associated with peripheral catheterization is generally low, with a point incidence rate of 0.1% of inserted short PIVCs (0.5 per 1000 intravascular device [IVD] days) (12). However, infectious complications may result in considerable annual morbidity due to the high frequency with which PIVCs are used – approximately 330 million short PIVCs are sold annually in the USA, and over a billion PIVCs are inserted each year in hospitalized patients worldwide (13, 14). However, many infections remain undetected because of short PIVCs’ dwell times and early patient discharge (15). A recent estimate reported as many as 10,000 Staphylococcus aureus bacteremia from peripheral catheters annually in the USA (15). Data collected over more than 5 years in two tertiary health-care services in Australia showed a high incidence of S. aureus bacteremia episodes associated with PIVCs inserted in the emergency room and with prolonged (≥4 days) dwell times (16). The authors estimated the financial cost of each PIVC-associated S. aureus bacteremia episode to be AUS$29,500 on average. After adjustment, this gave an estimated total cost of PIVC-associated S. aureus bacteremia, at the two institutions for the study period, of AUS$4.04 million. In the UK, a hospital-acquired infection adds 3-10 days to the length of a patient's stay in hospital, and can add £4,000-£10,000 to the cost of treatment (17).
Rates of phlebitis appear to vary between 2.3% and 67% of patients, depending on the definitions used and the populations studied.
Specific actions for prevention of PIVC failure have been clearly reinforced by the recent Infusion Nurses Society (INS) standards of practice (18). Nevertheless, consistent adoption of these measures in daily clinical practice appears weak, due to insufficient information and training, economic reasons and, perhaps, insufficient evidence.
However, the use of short PIVCs is widespread in oncology patients, particularly for those receiving IV medications in either inpatient or home-care settings (although their use in home care varies between countries). Peripheral catheterization may be performed by a wide range of health-care professionals, the necessary equipment is accessible and inexpensive, and catheter insertion is generally quick and easy to perform. Nevertheless, when using a short PIVC for chemotherapy administration, particular attention should be paid to some important aspects as outlined in the INS standards of practice (18). In particular, use is discouraged for vesicant and hyperosmolar infusates; prolonged infusions (>60 minutes). The use of infusion pumps, requires the use of a newly inserted cannula and blood flow should be routinely checked during infusion. Moreover, for chemotherapy infusion, insertion in a vein of the forearm is strongly recommended, avoiding hand, wrist and bend of the elbow veins.
As the procedure of peripheral catheterization is invasive, there is a need for greater consistency in the choice, insertion and management of short PIVCs. This is particularly relevant in oncology, with the growing trend for patients to receive many different courses of IV treatment over a number of years, sometimes with only short remissions (19). In this article, we review potential best practice with respect to PIVCs in cancer patients and consider the necessity for bundling these actions in a proposed care bundle. The concept of bundling has been shown to be an efficient tool to improve central venous catheter outcomes. There are growing concerns around short PIVC failure: as the etiology of most complications is difficult to identify and may be multifactorial, a global action such as a bundle approach (or strategy) becomes essential, instead of introducing single actions and monitoring outcomes.
This review represents a call to action for the medical research community to define a bundle strategy for short PIVCs in cancer patients that might improve outcomes of this type of vascular access device. The nature of the research that would be needed to support such an approach in oncology practice is also considered.
Core interventions shown to reduce catheter failure
Clinical studies have revealed a number of core interventions that have been shown to reduce the risk of catheter failure and which should therefore be regarded as best practice.
First and foremost is the fact that PIVC survival is improved when insertion is undertaken by IV teams and other specialists (20). It is therefore essential that all staff who insert and maintain a PIVC should be adequately trained and competent in the procedure (21), and should perform the procedure often enough to maintain a high competency level.
A PIVC should only be used when clinically indicated for the patient's condition. Both the intended dwell time and the physico-chemical characteristics of the infusate (pH, osmolarity, toxicity), notably with respect to vein damage, are important considerations in determining which type of device is the most appropriate. The use of non-thrombogenic materials appears to be of importance; polyurethane is less thrombogenic than other materials commonly used for short cannulas. A PIVC of appropriate size (gauge and length) should be selected depending on the patient's veins: the diameter (gauge) is important for patients with very thin veins, while the length is important for obese patients with deep-seated veins. PIVCs ranging in size from 20 to 24 G are strongly recommended even for adult patients (18). In addition, particular consideration should be given to the vein/catheter ratio, as previously assessed for peripherally inserted central catheters (22, 23).
Prior to PIVC insertion, it is important that an appropriate insertion site has been selected (the forearm is preferred, avoiding joints) (18, 20, 24). The chosen vein for insertion should be inspected and carefully palpated (18, 24–25–26). Potential aids for improving venous access success should be considered. These may include:
Hand hygiene is essential immediately prior to PIVC insertion (32) and it is advisable that the operator wears gloves for their own protection. The patient's skin at and around the entry area should be cleansed with either 2% chlorhexidine gluconate, or in 70% isopropyl-alcohol/propanol, and the disinfectant should be allowed to dry before insertion (33, 34). The PIVC device should be inserted using the aseptic/no-touch technique. Importantly, a new PIVC should be used for each attempted insertion. The 2016 INS standards of practice stress that flushing and locking are directly linked to the reduction in complications, and they recommend the use of pre-filled flush syringes, which may reduce catheter-related blood stream infections (CRBSIs) and save clinician time (18). Thus, it is advisable that the PIVC is flushed with 0.9% sodium chloride to check patency and is also locked with 0.9% sodium chloride if no infusion therapy is started immediately (35, 36). Adequate strategies should be undertaken to guard against back flow.
The PIVC site should be secured and stabilized, and also protected with a sterile catheter dressing that is polyurethane-bordered, transparent over the insertion site (18, 37, 38) and semi-permeable (35); there should also be a place for the date of dressing to be recorded, and it should have securement tapes. To date, studies into the use of an adhesive engineered stabilization device have proven inconclusive with respect to complication rates; further studies are therefore required (39, 40).
Care and maintenance during dwell time
The question of the length of time a PIVC should remain in place, has long been contentious. PIVCs are frequently recommended to be replaced after 72-96 hours. However, such routine replacement increases health-care costs and staff workload, and requires patients to undergo repeated invasive procedures, thus adding to their discomfort. Furthermore, the effectiveness of the practice is not well established. A multicenter, randomized study has shown that PIVCs should be removed as clinically indicated, but concluded that close monitoring of catheters in use must continue, with timely treatment cessation and prompt removal in case of complications (7). Thus, it is pertinent to consider those evidence-based interventions best able to support ongoing care and maintenance of PIVCs that are still needed.
The clinical need for the PIVC should be reviewed and recorded daily. If the clinical need remains, the PIVC and the site should be assessed to ensure the stabilization of the device, that the dressing remains intact, that there are no skin changes apparent at the site (color, swelling, warmth) and that the patient is experiencing no pain at the PIVC site. Of course, hand hygiene is mandatory immediately before touching the catheter and insertion site (41) and the operator should wear sterile gloves if palpation of the site, after removing the dressing, is necessary. Any complications such as phlebitis and/or local infection should be explored further. Prior to access, the access hub should be cleaned with either 2% chlorhexidine gluconate, or in 70% alcohol, and allowed to dry spontaneously in order to achieve prompt disinfection and reduce bacterial (re-)colonization (42); this combination is more effective than 70% alcohol alone (43). In addition, the PIVC device should be flushed with 0.9% sodium chloride prior to use in order to check patency; if the PIVC is still needed, it should be locked with 0.9% sodium chloride at least every 24 hours if left in place and, again, adequate strategies should be employed to prevent flow back of blood (18, 35, 36, 44, 45). The use of pre-filled flush syringes may reduce CRBSIs and save clinician time (18, 46). The dressing should be replaced if loose, wet or soiled.
A potential role for the care bundle approach?
A care bundle is a set of evidence-based interventions that, when used together in a single protocol, significantly improve patient outcomes (47–48–49). The care bundle approach in medicine was originally developed in the USA for central venous catheters (CVCs) (50). It seems reasonable to assume that the use of a care bundle-based approach for peripheral vascular access should result in prevention of catheter failure.
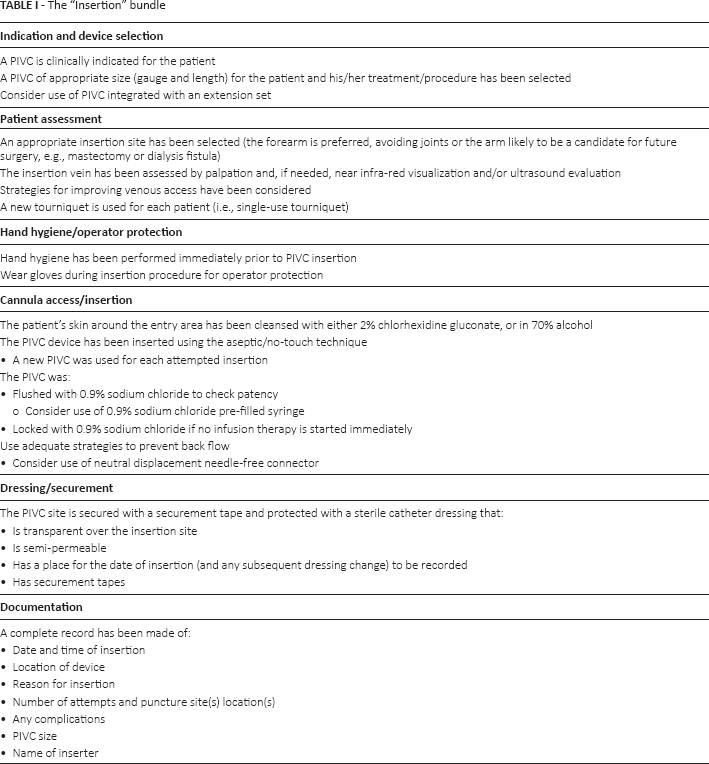
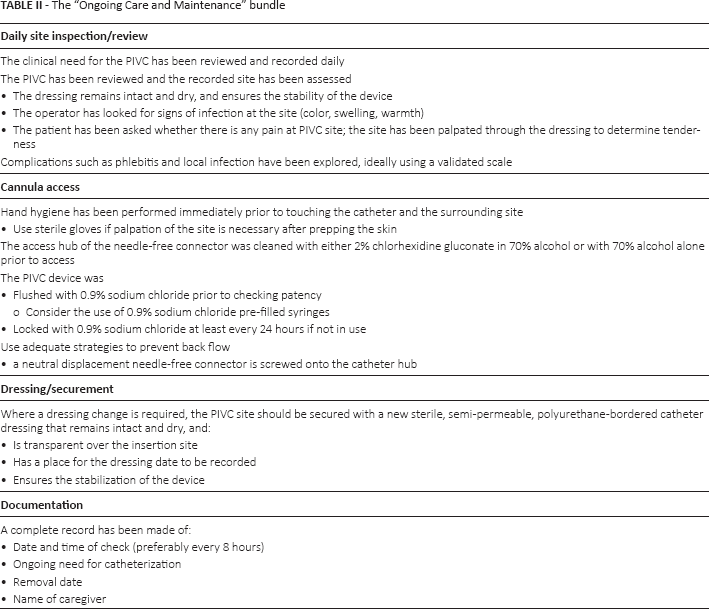
What would such a care bundle look like for oncology patients requiring chemotherapy or other medications administered via a PIVC, whether for insertion or for ongoing care and maintenance? Based on the evidence set out above, it is proposed that these would include the interventions summarized in Table I (insertion) and Table II (ongoing care and maintenance). Such care bundles should be applicable to all health-care professionals who treat adults or pediatric oncology patients, in both the acute and home-care settings – i.e., all doctors, nurses and other professionals trained in this procedure (it is recognized that the type of health-care professionals involved in PIVC insertion and care will differ from country to country).
The “Insertion” bundle
The “Ongoing Care and Maintenance” bundle
There are growing evidence-based data to support the use of central and peripheral venous catheter care bundles as a means of preventing CRBSIs and reducing patient morbidity in intensive care units (ICUs) and (pediatric) oncology units (46, 51–52–53–54–55–56–57). In a collaborative cohort study conducted predominantly in ICUs in the USA, an evidence-based care bundle intervention resulted in a large and sustained reduction (up to 66%) in rates of CRBSI that was maintained throughout the 18-month study period (58). The study intervention targeted clinicians’ use of five evidence-based procedures. These had all been recommended by the Center for Disease Control and Prevention as having the greatest effect on the rate of CRBSI and the lowest barriers to implementation (59). The recommended procedures were:
Hand washing prior to catheter insertion with either a waterless, alcohol-based product or an antibacterial soap and water with adequate rinsing
Using full-barrier precautions during the insertion of central venous catheters
Cleansing the skin with chlorhexidine 2%, in alcohol
Subclavian vein placement as the preferred site, with avoidance of the femoral site where possible
Removal of unnecessary catheters.
The value of the care bundle approach to reduce central line-associated infections in the acute care setting is recognized by guidelines from the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), the American Hospital Association (AHA), and the Association for Professionals in Infection Control and Epidemiology (APIC) (60). The US Center for Disease Control and Prevention has produced extensive evidence-based guidelines for the prevention of infection associated with PIVCs and CVCs (61). In France, the Haute Autorité de Santé has published a checklist as a tool for those inserting and managing central lines (62). In Germany, the Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) has issued recommendations concerning the insertion and maintenance of PIVC (63). In the UK, the NHS Modernisation Agency advocated the use of care bundles as they permit measurement of the actual therapeutic interventions against evidence-based guidelines, allowing the monitoring of compliance with the group of interventions, and leading to local organizational changes to improve delivery of therapy (64). This process encourages clinicians to analyze their practices and be open and honest about treatments and interventions, to enable learning and improvement within a no-blame culture. To reduce the incidence of patient harm during IV cannulation, improvements in the reliability of the process of delivery of care have been proposed. In England, the Department of Health devised the “Saving Lives” program (65) consisting of evidence-based, high-impact interventions (or care bundles) that relate to key clinical procedures or care processes that can reduce the risk of infection if performed appropriately. The interventions incorporate care bundles based on best-identified practice and care process and actions associated with quality patient care. Therefore, care bundles are now deemed to be standard practice in England (66).
There are many flow charts for diagnosis and treatment of malignant conditions. In the care bundle presented here, there is an emphasis on prevention rather than therapy: we do not address recommendations for treatment of infection, phlebitis or extravasation. The care bundle approach outlined in this article has been designed to prevent pathology in the oncology setting, where improving short PIVC outcomes may be of clinical relevance. However, this bundle may also be appropriate in other settings. US guidelines for prevention of central line-associated blood stream infections stress that most CRBSIs occur outside the ICU or in outpatients (60). Thus, infection prevention and control efforts should be targeted at vulnerable populations, including those receiving hemodialysis through catheters, intraoperative patients and oncology patients. Furthermore, besides central venous catheters, peripheral arterial catheters also carry a risk of infection (12).
Good quality evidence of clinical benefit is needed before health-care professionals are likely to adopt a care bundle for short PIVC insertion and care. Unfortunately, however, current research into the value of care bundles in PIVC is limited. Studies published to date have focused on central catheter insertion in the ICU, and have highlighted the equipment and logistical difficulties that health-care personnel may encounter (54, 56, 57). However, the literature on PIVCs is growing. One study assessed equipment availability for the more frequently undertaken insertion of PIVCs (67). A multidisciplinary team in Scotland designed and implemented a care bundle for the management of PIVCs, with the aim of reducing the incidence of PIVC-related infections (68). They audited compliance with the care bundle over a 25-week period, and were able to show that the initial compliance of 54% improved by 1.11% per week to 82% (95% confidence interval: 0.6%-1.6%; p = 0.0001). This was attributed to multiple interventions including daily assessment of PIVC necessity, weekly audit and feedback, monthly patient safety meetings to discuss issues with compliance, the introduction of new PIVC dressings and the promotion of new PIVC care plans. However, the team has not so far shown any improvement in clinical or patient-related outcomes.
Conclusion
Health-care professionals are more likely to respond enthusiastically to evidence of benefit in respect of clinically and patient-relevant endpoints rather than on process measures. Studies should therefore be geared towards showing a reduction in catheter failure rates, or a benefit in patient satisfaction, perhaps due to fewer days spent in hospital or less use of co-medication.
Footnotes
Financial support: This editorial article is based on a roundtable meeting organized and funded by Becton-Dickinson BD Company.
Conflict of interest: The authors declare no conflict of interest.