
Abstract
Objectives
Autogenous arteriovenous (AV) accesses are the preferred choice for the delivery of haemodialysis (HD). With an increase in the prevalence of end-stage renal disease and in the life expectancy of these patients, the quality and availability of superficial vessels can be limited and reduced with time. The use of prosthetic AV accesses may therefore become necessary for the delivery of HD. A new early cannulation vascular prosthesis (GORE® ACUSEAL Vascular Graft) has been introduced, developed to hinder suture line and cannulation needle bleeding. The authors report their experience with this new conduit at a London teaching hospital.
Methods
Between May 2011 and June 2013, 52 patients underwent 55 procedures where the ACUSEAL® prosthetic AV access was utilized to facilitate HD. The majority of procedures involved the placement of prosthetic brachio-axillary accesses or prosthetic axillo-axillary chest accesses.
Results
The 1-year primary and secondary patency was found to be 46% and 61%, respectively. Successful cannulation of the newly placed AV access was performed with 24 hours of surgery in 40 patients (73%). Tunnelled vascular catheters were required in only 10 (18%) patients. Six (11%) of the patients in the study suffered early complications, and 9 (16%) patients developed AV access infection.
Conclusions
These results show that, while providing patency results that compare favourably to those published for other types of regular prosthetic accesses, the conduits are amenable to very early cannulation with few cannulation-related complications. This leads to a dramatic reduction in the need for temporary or tunnelled catheters.
Introduction
Autogenous arteriovenous (AV) accesses are the preferred choice for the delivery of haemodialysis (HD), and are recognized to have better long-term patency and lower infection rates than prosthetic AV access (1––3). End-stage renal disease prevalence is increasing, as is the life expectancy of these patients (4). Therefore, both the quality and availability of superficial vessels can be limited and reduced with time, and the use of prosthetic AV accesses is becoming more necessary. In addition, the majority of patients with end-stage renal disease present late, and dialysis is initiated via central venous catheters that transfer an increased risk of infection and central venous stenosis (5). Obviating the need for the catheters by performing AV access early cannulation is advantageous (6).
Over the last two decades, authors have reported on multiple products that encourage early cannulation, with varying results (7––9––11––13–––16). A new early cannulation vascular prosthesis (GORE® ACUSEAL Vascular Graft) has been introduced, developed to hinder suture line and cannulation needle bleeding. The authors report their experience with this new graft at a London teaching hospital.
Methods
A prospective database was analysed retrospectively to identify all patients undergoing implantation of the ACUSEAL® (Gore Ltd, Flagstaff, AZ) prosthetic AV access from May 2011 to June 2013. Data on patient demographics, co-morbidities, vascular access history, further procedures and outcome were extracted from the database. This was supplemented and corroborated with data from medical records and radiographic imaging.
This graft is described by the manufacturers as a low-bleed, tri-layer vascular conduit that includes an elastomeric middle membrane between the inner and outer layers of expanded polytetrafluoroethylene (ePTFE). End-point covalently bonded heparin is reportedly anchored to the luminal surface, which imparts thromboresistant properties to the graft, while achieving sustained bioactivity (17).
The decisions to utilize prosthetic AV accesses in patients in this study were undertaken at weekly multi-disciplinary team meetings, which included vascular surgeons, nephrologists, anaesthetists, vascular technologists and specialist nurses. Native AV access was always considered first, with the use of a prosthetic AV access being proposed where this was not possible due to unsuitable or exhausted options. Patient choice was also taken into account, where patients elected for prosthetic AV access creation on the ipsilateral arm following failed native AV access, rather than the creation of a native AV access on the contralateral upper limb. Other considerations were the requirement for urgent dialysis, where the use of an early cannulation prosthetic AV access would avoid the use of tunnelled catheters. In addition, prosthetic AV accesses were utilized for the exclusion of grossly aneurysmal native AV accesses. In these cases, bypassing the aneurysm using an early cannulation prosthetic AV access avoided the use of tunnelled catheters. All patients who received a graft in our institution were already on haemodialysis through a central venous indwelling catheter, since we do not insert any early cannulation grafts on predialysis patients. These grafts being immediately ready for dialysis there is no need to insert them early. The only cases where these are inserted on a patient who does not have a central venous catheter is when we can operate on that patient just a day before their nephrologist wants to start dialysis. We therefore admit them as an inpatient to organize a dialysis shift just before surgery; they then have their catheter pulled out and go into the operating room ‘plastic free’ the next morning. We then keep them in an extra day to ensure that cannulation has been successful and that we have achieved a reasonable pump speed. Finally we ensure that the wounds are very clean and dry so as to avoid any early readmission within 30 days for which if it were to happen we would be penalized financially by our commissioners. The first cannulations are performed with 17 gauge needles and the first two or three dialysis sessions are organized at a lower pump speed (150 mL/min) to ensure that the tunnel is stable and not prone to bleeding. After these first two or three sessions cannulations are then performed as per our usual protocol and dialysis is organized at an adequate pump speed. All patients reported in this series were operated on at our institutions by only two vascular surgeons interested in vascular access formation and care.
Patients were followed for a minimum of 6 months to evaluate early cannulation success, post-operative complications and patency. Patency rates were calculated using life-table analysis. Fisher's exact test was used to compare categorical data. This review is not a prospective randomized trial or a research project, the declaration of Helsinki principles do not apply and we did not need to seek approval from our institution to write the report. As none of the patients can be identified it is not required at our institution to request permission to publish results that are part of a series. We therefore did not seek patients’ permission prior to submitting this work. No ethics committee approval according to the Declaration of Helsinki was required for this retrospective study.
Results
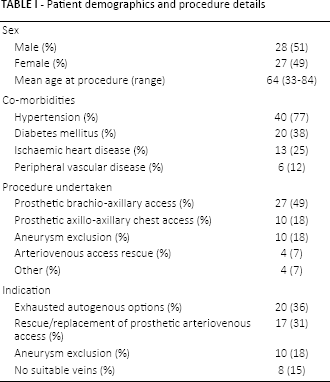
During the study period, 52 patients underwent 55 procedures where the ACUSEAL® prosthetic AV access was utilized to facilitate haemodialysis. In that period we have performed 616 access procedures (graft and native creations as well as rescues), so this represented a proportion of 8.9% of all our procedures. The majority of procedures involved the placement of prosthetic brachio-axillary accesses or prosthetic axillo-axillary chest accesses. Patient demographics, indications for prosthetic AV access use and procedures undertaken are presented in Table I. The median length of hospital stay was 3 days (range 2-30 days). The median patient follow-up was 533 days (range 7-963 days).
Patient demographics and procedure details
Complications and mortality
Six (11%) of the patients in the study suffered early complications. Of these, early AV access thrombosis occurred in three patients (5%), one of these occurring following a period of hypotension following gastrointestinal bleeding. Peri-anastomotic haematoma evacuation was required in two patients (4%). In one of these patients access function was lost, and the other suffered nerve injury secondary to pressure effects. A further patient required evacuation of a haematoma due to extravasation during cannulation, with prophylactic fasciotomy being performed. This was due to an insufficient pressure held after de-cannulation by the dialysis nurse in charge who waited only for 5 minutes once the needles had been removed. We reinforced to all our personnel the importance of pressing for at least 10 to 15 min after de-cannulation specifically when dealing with a newly inserted graft. Five patients (9%) died during the study period, four of whom had functioning AV accesses. The remaining patient presented (130 days following placement of the graft) moribund with systemic sepsis, and was managed with palliation.
Nine (16%) patients developed AV access infection, with five (9%) of these occurring within 30 days of implantation. In these patients who developed early infection, one AV access thrombosed, one suffered anastomotic dehiscence and two developed systemic sepsis. All of these prosthetic AV accesses were explanted. A further patient was successfully treated with antimicrobial therapy, washout and soft tissue cover. In the four patients who developed late infection of the AV access (median time to infection, 103 days), three developed systemic sepsis and in the remaining angioaccess thrombosed. In three of these patients, the prosthesis was explanted, with the remaining patient palliated as described above.
None of the patients in this study developed dialysis access-induced ischaemia. One patient required surgical repair of a mid-graft pseudoaneurysm, which occurred 420 days following initial placement.
Early cannulation
Successful cannulation of the newly placed AV access was performed with 24 hours of surgery in 40 patients (73%). A further six patients (11%) were cannulated within 1 week of surgery. Early cannulation did not take place as decided by the access nurse because these patients had a swollen arm or were in pain and not keen to have dialysis through their graft so early after surgery. The renal function in four patients (7%) did not deteriorate as expected, and cannulation was not required within the study period. One patient (2%) underwent successful cannulation 2 weeks following surgery, with the remaining four angioaccesses (7%) suffering early failure as described above.
Use of tunnelled catheters
In 11 patients (20%), prosthetic AV accesses were placed prior to the onset of haemodialysis, with these patients commencing dialysis with a working AV access, thus never requiring placement of a tunnelled catheter. The 10 (18%) patients undergoing aneurysm exclusion did not require tunnelled line use. Tunnelled lines were placed in 10 (18%) patients. In nine (16%) cases, these were placed as bridging catheters for continued dialysis prior to placement of the prosthetic AV access. A further patient (2%) required placement of a tunnelled line due to cannulation issues with the newly placed prosthetic AV access. The median duration these catheters remained in situ following surgery was 2 days (range 0-15 days).
Patency and reintervention
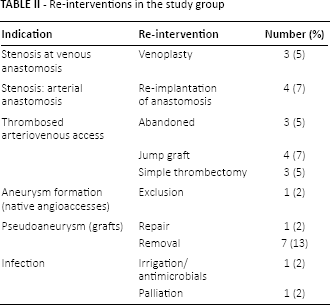
The 1-year primary and secondary patency in this study is 46% and 61%, respectively. No significant difference was noted in primary patency between prosthetic brachio-axillary accesses and prosthetic axillo-axillary chest accesses (40% vs 25%, p = 0.29, Fisher's exact test). The indications for re-intervention and procedures performed are presented in Table II.
Re-interventions in the study group
Discussion
This series of early cannulation ePTFE AV accesses shows clearly that, while providing patency results that compare favourably to those published for other types of regular prosthetic accesses, the conduits are amenable to very early cannulation with few cannulation-related complications. This leads to a dramatic reduction in the need for temporary or tunnelled catheters.
In our series all the catheters used except one were removed immediately following surgery, which is certainly something new and potentially very beneficial to these patients.
A total of nine patients suffered prosthetic AV infection during the study period: five during the immediate post-operative period and four during follow-up. This compares favourably with what is available on the topic in the recent literature (17) and may indicate that reducing the use of central venous catheters reduces the number of patients developing serious infective complications. None of these patients suffered from endocarditis or discitis, with just a single patient dying as a result of sepsis. This also supports favourably the extra cost that is necessary to purchase these grafts instead of our previous ones which could not be cannulated early. The reduction in inpatient admissions for infection, catheter insertions or complications due to these catheters more than offsets the extra cost borne by the use of these grafts.
The patency rates of these prosthetic AV accesses are satisfactory (Tab. III) and although we have not proven yet that they give better long-term results than standard PTFE accesses, one question will soon need to be asked: if patency rates are comparable if not better and when considering the dramatic reduction for central venous catheters should our patients only receive early cannulation AV prostheses?
Patency results with prosthetic arteriovenous accesses
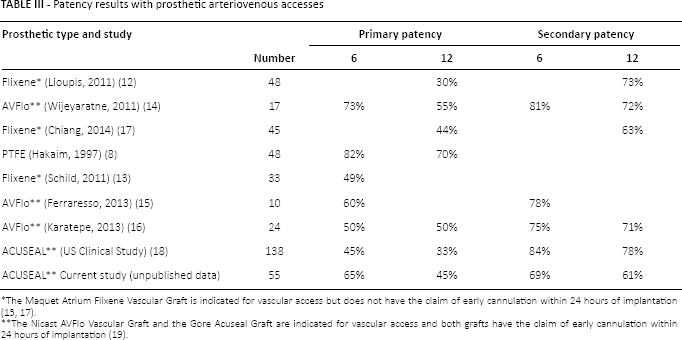
The Maquet Atrium Flixene Vascular Graft is indicated for vascular access but does not have the claim of early cannulation within 24 hours of implantation (13, 17).
The Nicast AVFlo Vascular Graft and the Gore Acuseal Graft are indicated for vascular access and both grafts have the claim of early cannulation within 24 hours of implantation (19).
These conduits are thicker which theoretically renders their handling a bit more complicated (Fig. 1), with particular reference to performing the venous anastomosis, yet the results we have found seem to contradict that fact, certainly for primary failure as well as 1-year patency rates. The company might envisage mitigating the potential handling problem at the venous end by applying their hybrid technique to the ACUSEAL® graft and thus allow a self-expandable stent anastomosis at the venous end (nitinol-reinforced section).
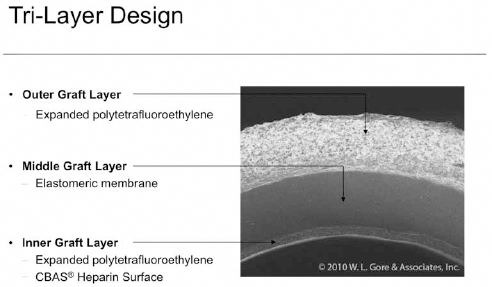
Transverse magnified view of an Acuseal Graft. Courtesy of W.L. Gore & Associates, Inc.
Seventy-three percent of our prosthetic AV accesses were cannulated within 24 hours and 11% within a week of implantation. Four (7%) patients saw their renal function improve and therefore did not need the AV access to be cannulated. We have therefore honed down our protocol and we now only operate on patients for whom the nephrologist has indicated the need for starting haemodialysis within 24 hours. This is likely to significantly reduce the number of patients receiving AV prostheses prior to requirement for their use.
For our patients already dialysed through a central venous catheter, the admission to our unit occurs the night before surgery. They undergo one final episode of dialysis via the catheter following which the catheter is removed, with the patient undergoing the implantation of the prosthetic AV access catheter-free. This potentially reduces the risk of infection but certainly mitigates the risk of procrastination when making the decision to remove the catheter. Regular ePTFE allows cannulation after a couple of weeks. Unfortunately in our experience in many cases cannulations get delayed for obscure reasons mainly because, we think, these patients are dialysed in satellite units where there is no surgical presence to push and influence on that matter.
The surgical technique is similar to that used for implantation of standard ePTFE AV accesses. Two small incisions are made at the elbow level just to expose a minimal segment of the brachial artery, a bit longer in the armpit where a longer segment of the axillary vein is to be exposed so as to allow a long venous anastomosis (up to 40 mm). The variant we use is when making the subcutaneous tunnel we avoid the use of a hollow tunnelling device and rather use a vascular clamp so as to reduce significantly the amount of dead space between the subcutaneous tissue and the graft and therefore aim to reduce the risk of haemorrhage surrounding the prosthesis during cannulation. There are 6 mm tunnellers available but we certainly feel that a clamp will make a much smaller tunnel tightly inhabited by the graft.
Conclusion
The Acuseal graft has shown patency rates comparable to those reported of standard PTFE grafts used for angioaccess. Their main advantage when compared to these standard grafts is that they could be cannulated almost immediately, thus potentially reducing significantly the need for central venous catheter insertions and their complications. They should potentially be considered as a new first choice when a graft is indicated for haemodialysis.
Footnotes
Financial support: None.
Conflict of interest: E. Chemla is a consultant for Gore Ltd.