
Abstract
Background
High-risk patients with stage II colon cancer may benefit from adjuvant chemotherapy, but identifying this patient population can be difficult. We assessed the prognosis value for predicting tumor progression in patients with stage II colon cancer, of a panel of 2 biomarkers for colon cancer: tumor budding and preoperative carcinoembryonic antigen (CEA).
Methods
Consecutive patients (N = 134) with stage II colon cancer who underwent curative surgery from 2000 to 2007 were included. Multivariate analysis was used to evaluate the association of CEA and tumor budding grade with 5-year disease-free survival (DFS). The prognostic accuracy of CEA, tumor budding grade and the combination of both (CEA-budding panel) was determined.
Results
The study found that both CEA and tumor budding grade were associated with 5-year DFS. The prognostic accuracy for disease progression was higher for the CEA-budding panel (82.1%) than either CEA (70.9%) or tumor budding grade (72.4%) alone.
Conclusions
The findings indicate that the combination of CEA levels and tumor budding grade has greater prognostic value for identifying patients with stage II colon cancer who are at high-risk for disease progression, than either marker alone.
Introduction
It is well-established that the oncological outcome for patients with stage II colon cancer is favorable, with the 5-year survival rate ranging from 60% to 85% compared with 25% to 60% percent for stage III disease (1, 2). However, patients with stage II colon cancer who are at high risk for disease progression are difficult to identify and remain an important but controversial problem. Studies indicate that only stage II disease patients with “high-risk” factors for disease progression will benefit from adjuvant chemotherapy (1, 3-7).
Features of high-risk patients with stage II colon cancer include bowel obstruction, perforation, T4 stage, resection of fewer than 12 lymph nodes, poor histological differentiation, lymphovascular invasion and lack of expression of the CDX transcription factors (3, 4, 8-12). However, the prognostic efficiency and accuracy of these variables are not optimal (13, 14). Thus, more robust and reliable prognostic indexes would be useful to select the subset of stage II colon cancer patients at high risk of tumor progression.
Tumor budding and carcinoembryonic antigen (CEA) serum levels have been found to be prognostic markers for colon cancer (15-28). Budding refers to isolated or small clusters of cancer cells that are present ahead of the invasive margin of the neoplasm, and are thought to be a key step in the metastatic process (29). The purpose of this study was to evaluate the prognostic accuracy of a panel that combined CEA and tumor budding (referred to as the CEA-budding panel) for identifying patients with stage II colon cancer at high risk for tumor progression.
Material and methods
This retrospective study evaluated consecutive patients with stage II colon cancer who underwent curative resection at Peking University Cancer Hospital between January 2000 and December 2007. The study was performed in accordance with the Declaration of Helsinki, and the Institutional Review Board of the hospital approved the protocol. All patients gave their written informed consent.
Study population
The patients included had stage II colon cancer and complete clinical and pathology data. Follow-up data were obtained from the institutional registration and follow-up database. Patients who received adjuvant therapy (either preoperative or postoperative) or had ulcerative colitis, familial adenomatous polyposis, hereditary nonpolyposis colorectal cancer-associated cancers or pure neuroendocrine tumors were excluded. Patients who underwent emergency surgery because of complete bowel obstruction or perforation were also excluded.
Study design
Patients were followed regularly for 5 years post surgery, with routine physical examination, serum CEA measurements and surveillance by colonoscopy, X-ray, ultrasonography and computer tomography (CT) scans. The primary endpoint (event) was tumor progression, including the presence of local recurrences and metachronous distant metastasis. Patients were treated as censored if they outlived the 5-year follow-up without tumor progression.
Pathology assessment
For each case, standard pathology analysis was performed by one of the authors using light microscopy to evaluate sections of formalin-fixed and paraffin-embedded specimens stained with hematoxylin-eosin. Each colon tumor was staged as defined by the American Joint Committee on Cancer's (AJCC) Cancer Staging Manual, 7th edition (30). Pathology features such as histological differentiation, depth of tumor invasion and lymphovascular invasion (LVI) were documented. The number of retrieved lymph nodes was also recorded. Macroscopic margins were assessed at surgery, and microscopic margins were assessed by histopathology to ensure R0 resection.
Estimation of tumor budding
Sections of invasive tumor margins from specimens were selected for microscopic examination. The presence of tumor budding was determined using the criteria proposed by Ueno et al (15), wherein budding is defined as an isolated single cancer cell or a cluster composed of fewer than 5 undifferentiated cancer cells appearing to bud from a large cancer gland at the invasive front. For budding quantification, at least 5 consecutive tumor slides were reviewed (Fig. 1). Every slide was initially scanned at low power magnification (×100) to identify areas with the highest density of budding (Fig. 2). Three areas per tumor with the highest budding density were then identified, and the number of buds in each area was counted at higher magnification (×200, field of view = 0.94985 mm2). The highest number of tumor buds among these 3 areas was recorded as the number of buds per field view (intensity). Using previously reported grading criteria (15, 17-20), tumor budding was classified into low-grade or high-grade based on the budding intensity; no buds or a budding intensity between 1 and 9 were termed low-grade, while intensities ≥10 were termed high-grade. All slides were interpreted for tumor budding by the same pathologist, who was blinded to the corresponding clinical and pathology outcomes.
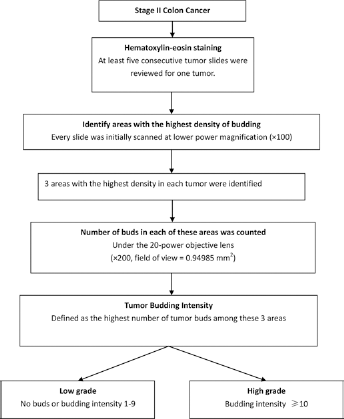
Flow chart for evaluation of tumor budding.
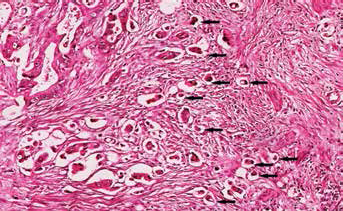
Example of a colon cancer section showing high-grade tumor budding characterized by large amounts of isolated cancer cells (arrows) or small clusters of cells ahead of the invasive front.
Serum CEA measurements
Serum CEA levels were measured with Elecsys CEA electrochemiluminescence assay on a Modular Analytics E170 system (Roche Diagnostics GmbH, Tokyo, Japan) with a reference range of 5.0 ng/mL. Serum CEA values ≥5 ng/mL were considered abnormal.
CEA-budding panel categories
The CEA-budding panel evaluated risk using both tumor budding and CEA characteristics. Patients were categorized as high-, moderate- or low-risk. The low-risk group included patients with low-grade budding and normal serum CEA levels (<5 ng/mL). The high-risk group included patients with high-grade budding and CEA levels of ≥5 ng/mL. The moderate-risk group contained patients with low-grade budding and CEA levels ≥5 ng/mL, and patients with high-grade budding and normal CEA levels. Due to the small number of patients in the low- and moderate-risk groups, the 2 groups were combined for statistical analysis.
Statistical analysis
Categorical variables were presented as numbers and percentages. Chi-square tests were performed to detect the association of variables with budding grade. Kaplan-Meier curves with log-rank tests were performed to investigate the 5-year disease-free survival (DFS) rate for each characteristic and to compare the differences between groups for each variable. Multivariate Cox proportional hazard model with backward stepwise model selection was performed to detect which factors were associated with DFS. The prognostic values of the panel and each prognosticator were evaluated for their positive predictive value (PPV), negative predictive value (NPV) and accuracy. McNemar tests were performed to detect the association between different diagnostics.
Statistical analyses were performed by IBM SPSS statistical software version 2.2 for Windows (IBM Corp., Armond, New York, USA). And a 2-tailed p value of <0.05 indicated statistical significance.
Results
Baseline characteristics of patients
Baseline characteristics are summarized in Table I. A total of 134 patients were included in this study; 95 had low-grade budding and 39 had high-grade budding. Except for serum CEA levels, no significant difference between the low- and high-grade budding groups with respect to baseline demographics and disease characteristics was observed. A greater percentage of patients with high-grade budding had serum CEA ≥5 ng/mL than serum CEA <5 ng/mL (40.0% vs. 21.5%, respectively, p = 0.021). The study included more men than women (82 men vs. 52 women), and their mean age was 65.9 years (range 29-79). Sixty-six patients had tumors in the right colon (56 in the ascending colon and 10 at the hepatic flexure of the transverse colon), and 68 had tumors in the left colon (38 in the descending colon, 21 in the sigmoid colon and 9 at the splenic flexure of the transverse colon). In both groups, a higher number of patients had moderate histological differentiation, T3 stage cancer and no lymphovascular invasion. In the low-grade budding group, more patients had ≥12 retrieved lymph nodes, while in the high-grade budding group, a similar number of patients had <12 or ≥12 retrieved lymph nodes. Median follow-up was 66.5 months (range 18-96). Eight patients (6.0%) were lost to follow-up.
Baseline characteristics of patients
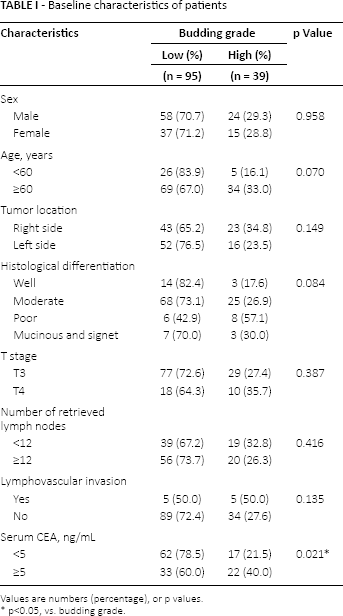
Values are numbers (percentage), or p values.
p<0.05, vs. budding grade.
Five-year DFS and multivariate analyses
Five-year DFS was significantly higher in patients with serum CEA <5 ng/mL compared with those with serum CEA ≥5 ng/mL (92.0% vs. 59.9%, respectively; p<0.001) (Tab. II). DFS was also higher in the low-grade budding group compared with the high-grade budding group (85.9% vs. 61.2%, respectively; p<0.001) (Tab. II). No other demographic or disease characteristic were significantly associated with 5-year DFS.
Results of 5-year disease-free survival (DFS) and multivariate analyses
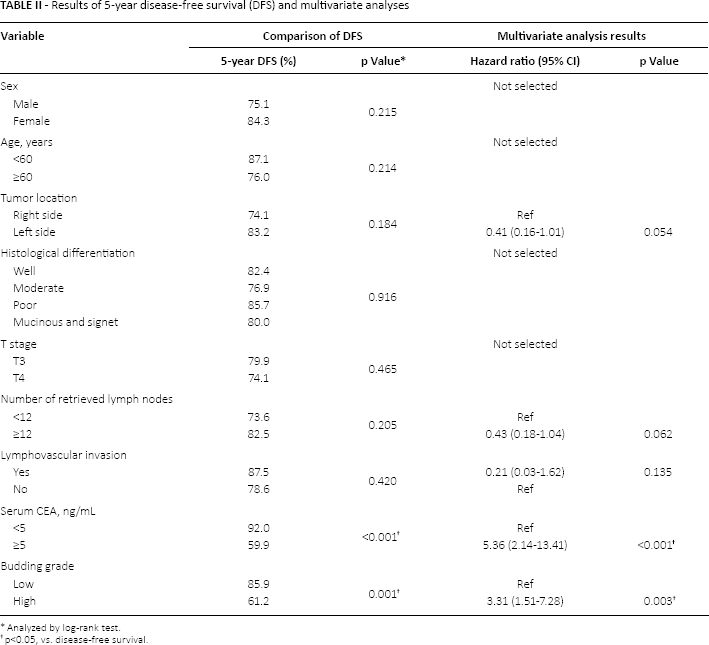
Analyzed by log-rank test.
p<0.05, vs. disease-free survival.
Multivariate analysis was performed using the following characteristics that were identified by backward stepwise model selection: tumor location, number of retrieved lymph nodes, lymphovascular invasion, serum CEA and budding grade (Tab. II). The hazard of disease progression was significantly increased in patients with serum CEA ≥5 ng/mL compared with those with serum CEA <5 ng/mL (hazard ratio [HR] = 5.36, p<0.001) and was also significantly increased in patients with high-grade budding compared with those with low-grade budding (HR = 3.31, p = 0.003) (Tab. II). No significant association of 5-year DFS with tumor location, number of retrieved lymph nodes or lymphovascular invasion was observed (Tab. II).
Kaplan-Meier analysis was used to evaluate DFS in the low-grade and high-grade budding groups and in the in low-risk, moderate-risk and high-risk groups as defined by the CEA-budding panel classification (see “Methods”). Kaplan-Meier analysis indicated that DFS was significantly longer in the low-grade budding group compared with high-grade budding group (p<0.001) (Fig. 3). The 5-year DFS rate was 85.9% in the low-grade budding group and 61.2% in the high-grade budding group (Fig. 3). Kaplan-Meier analysis also found that DFS was significantly longer in the low-risk group compared with the moderate-risk (p = 0.031) and high-risk (p<0.001) groups (Fig. 4). The moderate-risk group had longer DFS than the high-risk group (p<0.001). The 5-year DFS rate was 40.9% in the high-risk group, 78.7% in the moderate-risk group and 93.0% in the low-risk group (Fig. 4).
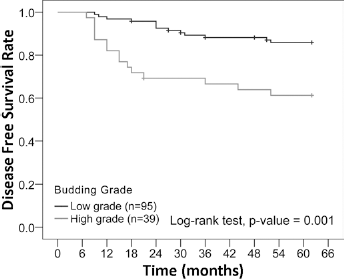
Disease-free survival between budding grades.
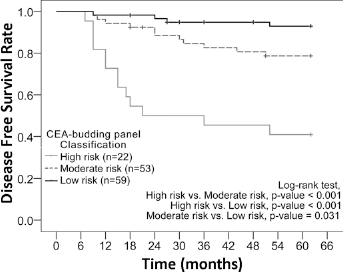
Disease-free survival between CEA-budding panel classifications. The 5-year survival rates were 40.9% in the high-risk group, 78.7% in the moderate-risk group and 93.0% in the low-risk group.
Prognostic accuracy of tumor budding, serum CEA and CEA-budding panel
The prognostic value of tumor budding, serum CEA and the CEA-budding panel for DFS was evaluated (Tab. III). Tumor budding, CEA levels and the CEA-budding panel were significantly associated with tumor progression (all p values <0.001). The 2 individual biomarkers and the CEA-budding panel had high NPVs (range 86.3%-92.4%) and moderate PPVs (range 38.5%-59.1%). The CEA-budding panel had the highest accuracy (82.1%) for indicating risk of disease progression, followed by tumor budding grade (72.4%) and serum CEA levels (70.9%).
Predictive values of tumor budding, serum CEA and CEA-budding panel
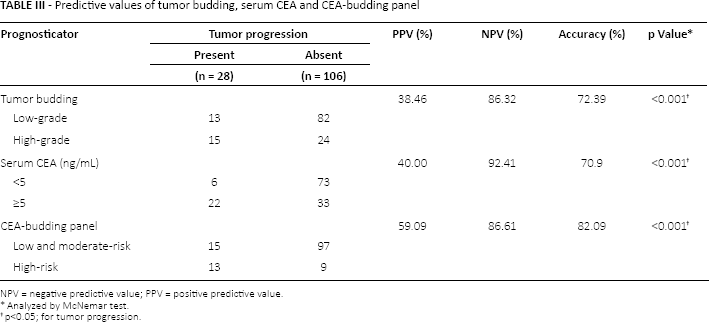
NPV = negative predictive value; PPV = positive predictive value.
Analyzed by McNemar test.
p<0.05; for tumor progression.
Discussion
This study evaluated whether combining 2 biomarkers of disease progression (CEA and budding grade) would increase the prognostic accuracy for determining the risk of disease progression in patients with stage II colon cancer who had not received adjunctive therapy. The study found that CEA and budding grade each was associated with 5-year DFS and had a prognostic accuracy of 70.9% and 72.4%, respectively. Combining both markers into a multimarker panel improved prognostic accuracy to 82.1%. Our findings indicate that combing CEA and tumor budding grade has greater prognostic accuracy than either parameter alone. Most studies have assumed that patients with stage II disease have low-grade budding tumors and have low risk of disease progression (22-26, 31). However, our results suggest that only those patients with normal serum CEA levels and low-grade budding have low risk of disease progression. The accuracy of the CEA-budding panel for predicting the risk of progression suggests that it may be useful in helping to guide treatment and management decisions.
The prognostic value of tumor budding and CEA in stage II colon cancer has been studied previously (22-26, 28). Clinically, tumor budding reflects tumor aggressiveness, as confirmed by its impact on tumor metastasis and long-term survival (15, 16, 18, 32-34). Some studies have clearly demonstrated that stage II disease with high-grade tumor budding has comparable outcomes to stage III disease (16, 23). Although tumor budding grade is an independent risk factor, its use as a prognostic indicator in colon cancer is limited by its low diagnostic accuracy (<75%), which in part, reflects its low PPV of <60% (16, 22-26). Similarly, we also found budding grade to have low prognostic accuracy (72.4%) for disease progression and low PPV (38.5%).
Recently, another study evaluated the use of multiple markers to improve the ability to identity high-risk stage II colon cancer patients (35). They used 4 pathology-determined parameters: adjacent organ involvement, histological differentiation, lymphovascular invasion and the number of lymph nodes retrieved. All 4 were found to be independent prognostic factors by multivariate analysis.
The present study was limited by the fact it was retrospective in design and consequently was subject to several biases. However, the study characterized a new tool that may improve the accuracy for determining the prognosis of patients with stage II colon cancer. It is possible that the addition of other markers may further improve prognostic accuracy.
Conclusion
In conclusion, the CEA-budding panel has high accuracy for predicting disease progression and may help identify high-risk patients with stage II colon cancer. Additional studies are needed to further test the prognostic accuracy of the CEA-budding panel in determining the risk of disease progression in patients with stage II colon cancer, and whether the CEA-budding panel should be adopted by clinicians to assess if a patient would benefit from adjuvant chemotherapy.
Footnotes
Financial support: This work was supported by Capital Heath Development Funding “Beijing Municipal Commission of Health and Family Planning” (grant no. SHOUFA-2011-2015-03).
Conflict of interest: None of the authors has any financial interest related to this study to disclose.