
Abstract
Background
Determination of the extent of involvement or pathological staging is one of the requirements for adequate evaluation of bladder cancer specimens. Therefore, the differentiation between MP and MM is essential for proper treatment and avoiding over or under staging.
Aim
The present study aimed at evaluation of diagnostic value of smoothelin and vimentin expression both singly and in combination for differentiation between MM and MP.
Methods
This study was carried out on 59 cystectomy specimens of primary bladder carcinoma and eleven cystoscopic biopsies for non-neoplastic bladder lesions (cystitis).
Results
Histologically, MM was identified clearly in 40 cases and MP was identified in all 70 examined cases. The cases were immunostained for smoothelin and vimentin. Intensity of smoothelin expression showed significant difference (P = 0.001) between MM and MP with 97.5% sensitivity and 95% specificity and the percentage of smoothelin expression was significantly higher in MP compared to MM (P = 0.001) with 95.7% sensitivity and 85% specificity (using 65% as cut-off point). Vimentin was negative in MP and showed positive expression in 32 cases (80%) of MM with a statistical significant difference (P = 0.001) providing 80% sensitivity and 100% specificity. Combined moderate to strong smoothelin and negative vimentin offered 100% sensitivity and 100% specificity towards the identification of MP.
Conclusions
Differentiation of MM from MP can be made based on histopathological criteria, which are unfortunately overlapping in many cases. Moderate to strong smoothelin expression with negative vimentin could be very helpful procedure in difficult and overlapping cases with a high diagnostic validity.
Introduction
Urinary bladder carcinoma is one of the most common malignancies in Egypt and worldwide and a significant cause of morbidity and mortality (1). In Egypt, it represents 6.94% of total cancer cases according to the national population-based cancer registry program (2).
One of the requirements for adequate evaluation of bladder cancer obtained by cold biopsy and transurethral resection specimens is the determination of extent of involvement, or pathological staging (3). The carcinoma may be limited to the epithelium (noninvasive papillary carcinoma [pTa] or carcinoma in situ [pTis]), extend into the subepithelial connective tissue or lamina propria (pT1), have invaded the detrusor muscle or muscularis propria (pT2), or extend into the perivesical soft tissues (pT3) (4).
Although this might appear relatively straightforward, there are several well-known pitfalls in the pathological staging of bladder carcinoma (3, 5) which one should be aware of to avoid both understaging and overstaging of bladder carcinoma. Overstaging caused by misdiagnosis of muscularis mucosa as muscularis propria will lead to radical surgical management (cystectomy) for a tumor that would otherwise be treated conservatively (intravesical bacille Calmette-Guérin [BCG] therapy). Understaging will lead to improper treatment, with an increased mortality rate (5, 6).
Differentiation between invasion of muscularis mucosa (MM) and of muscularis propria (MP) can be made based on histological form, histological relations or antigenic properties. MM is usually dispersed, has an interrupted layer and is usually associated with vascular plexus (7), whereas MP forms regular bundles (8); however, hyperplastic MM could be found in 17%-53% of specimens simulating thick bundles of MP (8, 9).
Despite the fact that vascular plexus is absent in MP, it can also be absent in MM, especially in transurethral resection of urinary bladder tumor (TURBT) specimens (10). Moreover, TURBT specimens of low quality and low quantity are not rare, leading to disorientation of the specimens. There are topographical variations of the MP bundles in bladder trigone and at the insertion of the ureter (8, 10). Trigonal MP extends more superficially and often shows gradual diminution of the bundle size as it extends to an almost suburothelial location.
Adipose tissues cannot be used as a landmark either, as it can be seen in between MP bundles or to extend superficially to lamina propria (11). Immunological profile seems to be a reliable tool for the differentiation of MM from MP; however, until today, data are very limited, and no widely accepted antigen has yet been identified as a sensitive marker.
Smoothelin is a cytoskeletal protein specifically expressed in differentiated smooth muscle cells and has been shown to colocalize with α-smooth muscle actin. Smoothelin has 2 isoforms, the small isoform (59 kDa), which is abundant in visceral smooth muscle, and a large smoothelin isoform (117 kDa), which is specifically expressed in vascular smooth muscle cells (12).
Vimentin is the most widely distributed intermediate filament and is expressed in virtually all mesenchymal tissues (13). Studies had shown that the smooth muscle cells of the MP rarely and weakly express vimentin, whereas smooth muscle cells of the MM show moderate or strong expression (14).
Therefore, our study aimed at evaluation of the diagnostic value of smoothelin and vimentin expression both singly and in combination, for differentiation between MM and MP.
Materials and Methods
This was a retrospective study conducted on 70 urinary bladder specimens (59 cases of primary urinary bladder carcinoma received as cystectomy specimens and 11 cystitis cases received as cystoscopic biopsies), retrieved from the archives of the Pathology Department, Faculty of Medicine, Menoufia University, spanning the period between January 2014 and January 2016. They were selected based on the presence of muscle layers either in neoplastic or nonneoplastic cases and ability to differentiate MP from MM. The rationale for using cystoscopic biopsy was to guarantee the presence of MM. Cases with overlapping features were excluded.
Several sections, 4-μm thick, were cut from each block. One was stained with routine hematoxylin and eosin to confirm the diagnosis and to evaluate the histopathological characteristics of malignant cases including tumor type, grade, stage and muscle invasion. Further evaluation and distinctions between MM and MP were assessed in each case. Other sections were cut on poly-L-lysine-coated slides to be immunostained with smoothelin and vimentin antibodies.
Evaluation of specimens (cystectomy and cystoscopic specimens) to differentiate MM from MP
MM is characterized by thin slender bundles arranged in a single layer of interrupted, wispy dispersed or continuous but often discontinuous smooth muscle fibers (3, 15). Hyperplastic patterns of MM can be (a) aggregates of hyperplastic MM with haphazard outlines distinct from that of MP, or (b) hyperplastic compact MM with parallel muscle fibers and regular outline arranged singly or in small groups that occasionally strongly resembled MP muscle but are distinguishable from it on the basis of the location in the lamina propria (LP) (8). Commonly, the LP vascular plexus is present in every section most often in association with the MM (7).
On the other hand, MP is characterized by coarse muscle bundles with rounded contours. MP shows a relatively regular interface with the LP in some cases and an irregular interface in others. A distinctive pattern is noted in the trigone where occasionally there is a gradual diminution of size of the MP muscle bundles as they extend to almost a suburothelial location (8).
Immunohistochemistry
The method used for immunostaining was the streptavidin-biotin amplified system using a Universal Dakocytomation Labelled streptavidin–Biotin-2 system, with horseradish peroxidase (LSAB-2 System, HRP Kit, Catalogue No. k0679). The slides were deparaffinized using xylene and then rehydrated in decreasing concentrations of ethanol. Antigen retrieval using microwave heating (20 minutes; 10 mmol of citrate buffer, pH 6.0) after inhibition of endogenous peroxidase activity (hydrogen peroxidase for 15 minutes) was used. The primary antibodies were mouse monoclonal antibody raised against smoothelin (CM 372 A; Biocare, USA), received as 0.1 ml concentrate and diluted with phosphate-buffered saline (PBS) to a dilution of 1:150, and mouse monoclonal antibody raised against vimentin (V9) (MS-129-P; Thermo Scientific, USA), the antibody was received as 1 ml concentrated and diluted with PBS to a dilution of 1:50. These were applied on the slides and incubated overnight at room temperature in a humidity chamber.
Finally, the detection of bound antibody was accomplished using a modified labeled avidin–biotin (LAB) reagent for 20 minutes then PBS wash. A 0.1% solution of diaminobenzidine (DAB) was used for 5 minutes as a chromogen. Slides were counterstained with Mayer's hematoxylin for 5-10 minutes. Negative control slides were prepared, by omitting the primary antibodies from the staining procedure. Tissue sections prepared from colon carcinomas were used as a positive control for smoothelin, and leiomyosarcoma samples were used as positive control for vimentin according to the supplied data sheet.
Interpretation of Immunostaining
Both smoothelin and vimentin expression were evaluated in nonneoplastic and malignant groups. For smoothelin and vimentin, cytoplasmic staining in any number of cells was required to identify them as positive. Smoothelin and vimentin expression was evaluated in both MM and MP for:
Positivity: positive versus negative. Intensity: subdivided into mild, moderate and strong. For statistical purposes, mild was included with negative cases, versus moderate and strong cases. Percentage of expression was assessed and expressed as mean, median and range.
Statistical analysis
Data were collected, tabulated and statistically analyzed using a personal computer with SPSS, version 22. The Fisher exact test and the t-test were used for evaluation of qualitative and quantitative data, respectively. Accuracy, specificity, sensitivity, positive and negative predictive values were used to assess diagnostic values of tested markers. Receiver operator characteristic (ROC) curves were used to assess the diagnostic values of quantitative data such as percentage of expression and selection of the best cutoff point.
Clinical and pathological data for the malignant cases are presented in Table I.
Clinicopathological parameters of malignant cases
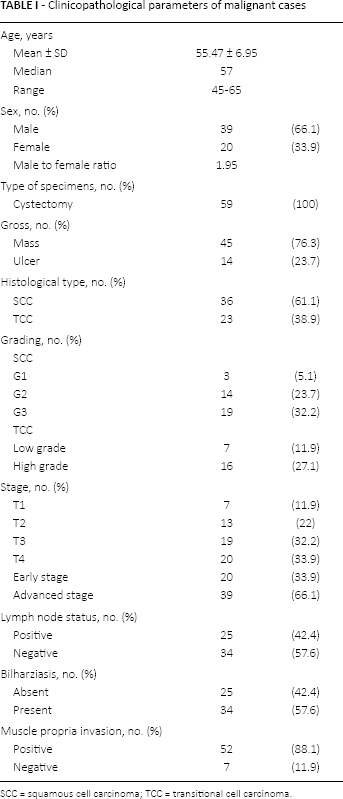
SCC = squamous cell carcinoma; TCC = transitional cell carcinoma.
Results
Histological differentiation between MM and MP
Histopathological examination identified MM in all cystoscopic biopsies (cystitis cases: 11/11) and in 29/59 of cystectomy specimens (malignant cases), with a total number of 40 cases (Fig. 1A). MM was masked by invading tumor cells in the remaining 30 cases of the malignant group (30 of 59 cases), so it was difficult to identify. The MP was identified in 70 cases (11 cystoscopic and 59 cystectomy specimens) (Fig. 1B, C).
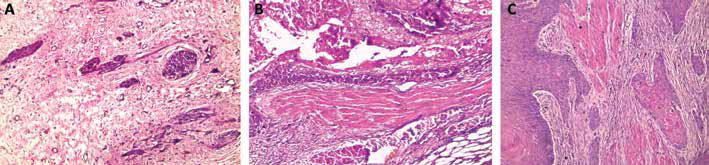
(A) Histopathology slide shows muscularis mucosa (MM) as characterized by thin bundles arranged in a single layer of interrupted and dispersed muscle surrounded by lamina propria vascular plexus (hematoxylin & eosin [H&E] stain; magnification ×200). (B) A case of invasive high-grade transitional cell carcinoma (TCC) infiltrating large coarse longitudinal muscle bundles of muscularis propria (MP) (H&E staining; magnification ×400). (C) Grade II squamous cell carcinoma infiltrating MP. MP appears as large coarse muscle bundles of regularly oriented muscle fibers with regular outline, rounded contours and closely packed, lacking vascular plexus (H&E stain; magnification ×200).
Immunohistochemical results of smoothelin expression in MM and MP
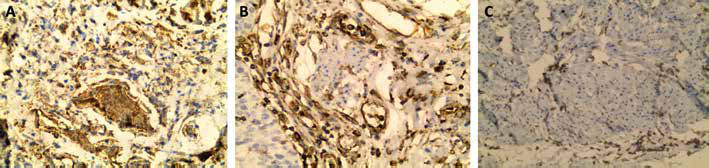
Cytoplasmic smoothelin expression was identified in 24 out of 40 available MM (11 cystoscopic and 29 cystectomy specimens) (Tab. II). The intensity of smoothelin expression in MM ranged from negative to mild in 37 cases (92.5%) (Fig. 2A) and moderate to strong in 3 cases (7.5%) (Fig. 2B). The percentage of smoothelin expression in MM ranged from 10% to 70%, with a mean ± SD of 47% ± 18.47% and a median of 50%.
Comparison between MM and MP regarding smoothelin expression
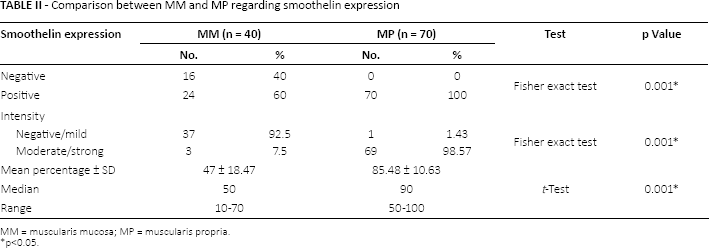
MM = muscularis mucosa; MP = muscularis propria.
p<0.05.
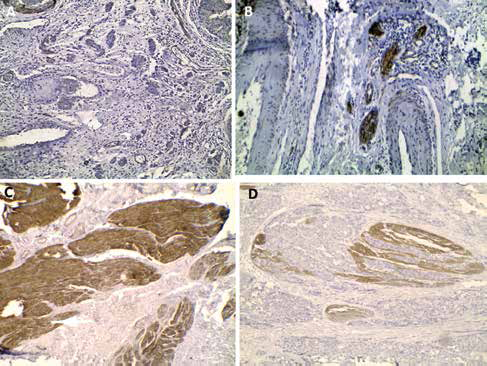
Immunohistochemistry shows muscularis mucosa (MM) with mild to negative (A) and strong (B) smoothelin expression. Muscularis propria (MP) shows moderate to strong smoothelin (C) which is masked by infiltrating transitional cell carcinoma (TCC) (D) (immunohistochemical staining; magnification ×100 for A, and ×200 for B, C and D).
All MP were positive for smoothelin, 69 showed moderate to strong smoothelin expression (Fig. 2C, D), and 1 case showed mild expression (Fig. 3A). Smoothelin expression was localized in the cytoplasm of positive cells. The percentage of smoothelin expression ranged from 50% to 100%, with a mean of 85.48% ± 10.63% and a median of 90%.
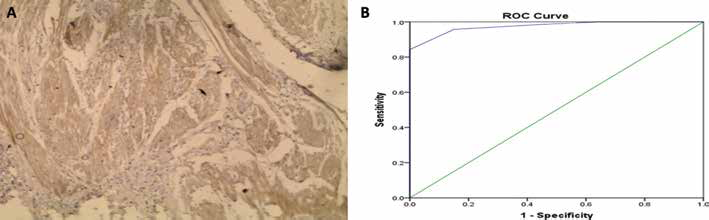
(A) Immunohistochemistry shows mild expression of smoothelin in muscularis propria (MP) (immunohistochemical staining; magnification ×200). (B) Receiver operator characteristic (ROC) curve shows 65% as a suitable cutoff point for the percentage of smoothelin expression that can discriminate between muscularis mucosa (MM) and MP.
Diagnostic validity of smoothelin expression in differentiation between MM and MP
Smoothelin was expressed in whole MP (70/70; 100%) and in 24/40 of MM (60%) with a significant difference (p = 0.001) (Tab. II). This greater positive expression in MP than in MM elicited a diagnostic value of smoothelin positivity with 100% sensitivity, 40% specificity, 74.49% positive predictive value, 100% negative predictive value and 78.18% accuracy (Tab. III).
Evaluation of diagnostic validity of smoothelin
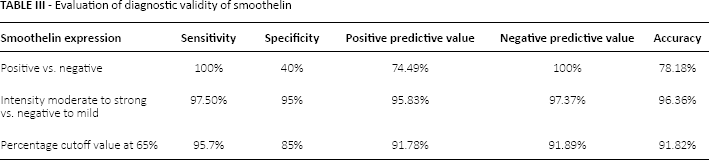
Regarding intensity of expression, moderate to strong smoothelin expression indicated MP rather than MM, with a significant difference (p = 0.001) (Tab. II). The diagnostic power of smoothelin intensity revealed 97.5% sensitivity, 95% specificity, and 95.83% positive predictive value, 97.37% negative predictive value and 96.36% accuracy (Tab. III).
Furthermore, the mean and median percentage of smoothelin expression showed significantly high values in MP compared with MM (p = 0.0001) (Tab. II). Examining the ROC curve determined 65% as a cutoff point for smoothelin percentage of expression. At this value, the diagnostic power of smoothelin percentage showed 85% specificity, 95.7% sensitivity, 91.78% positive predictive value, 91.89% negative predictive value, and 91.82% accuracy (Tab. III; Fig. 3B). (NB: The diagnostic validity of combining smoothelin percentage of expression and intensity revealed the same results as smoothelin intensity of expression.)
Immunohistochemical expression of vimentin in MM and MP
MM showed cytoplasmic expression of vimentin in 35/40 cases (87.5%); 8 of these were moderate to strong (8/40, 20%) (Fig. 4A), and 27/40 (67.5%) were mild. Five cases were negative (5/40, 12.5%) (Fig. 4B). All MP of the examined cases were negative for vimentin (Fig. 4C). This absent vimentin expression in MP was limited to smooth muscle bundles; however, moderate to strong expression was seen in the endomysial and endothelial cells interspersed between the smooth muscle fibers.
Immunohistochemistry shows prominent expression of vimentin in muscularis mucosa (MM) bundles in (A) and absence of expression in (B), while it is expressed in endothelial cells and endomysial cells. Muscularis propria (MP) lacked vimentin expression (C) (immunohistochemical staining; magnification ×200).
Diagnostic validity of vimentin in differentiation between MM and MP
Considering positive versus negative vimentin for identification of MM revealed 80% sensitivity, 100% specificity, 100% positive predictive value, 89.74% negative predictive value and 92.73% accuracy.
We could not assess the diagnostic validity of vimentin regarding intensity and percentage of expression, because vimentin was not expressed in MP.
Diagnostic validity of combined smoothelin and vimentin expression in differentiation between MM and MP
Moderate to strong smoothelin expression and negative vimentin expression showed 100% sensitivity, 100% specificity, 100% positive predictive value, 100% negative predictive value and 100% accuracy toward MP identification.
Association between smoothelin expression by MP and vimentin expression by MM and the parameters studied in urinary bladder carcinoma
There were no significant associations between smoothelin expression by MP and vimentin expression by MM and the clinicopathological parameters studied in urinary bladder carcinoma (data not shown).
Discussion
We selected our cases based on the feasibility of differentiation between MM and MP by histopathological examination, because the histopathological criteria were considered as a reference to evaluate the diagnostic value of tested markers. The diagnostically difficult cases, with overlapping criteria between MM and MP, were excluded.
In our study, smoothelin was highly expressed in MP compared with MM since moderate to strong expression was seen in 98.57% of MP and 7.5% of MM with a significant difference (p = 0.001). Furthermore, the percentage of smoothelin expression was significantly higher in MP (median 90%) compared with MM (median 50%) (p = 0.001).
Therefore, in the present study, smoothelin alone gave 100% sensitivity and 40% specificity when considering positive versus negative values, while the sensitivity decreased to 97.5% and specificity increased to 95% when considering intensity (negative to mild versus moderate to strong smoothelin). Our work agreed with that of others (16, 17) in that there was a relative difference in smoothelin expression between MM and MP, making it a promising marker for differentiation limited by overlap of moderate smoothelin expression in MM.
Expression of smoothelin in MP and not in MM can be explained by its expression in only fully differentiated contractile smooth muscles and not in proliferative smooth muscles. Several authors have suggested that smooth muscle cells can be divided into 2 phenotypes: contractile and proliferating/synthetic smooth muscle cell types (12, 18). Overlap in smoothelin expression in MM can be explained by phenotype switches between these stages of differentiation. This switch has been suggested by some researchers, but this issue is still not resolved (18).
According to our results, positive to strong smoothelin was only seen in 7.5% of MM, in contrast to the results of others (19) who demonstrated larger numbers of MM showing moderate to strong smoothelin expression (28%). On the other hand, Miyamoto et al found mild smoothelin expression in 6% of MP (19) in contrast to only 1.43% in our study. The difference in smoothelin results can be explained by type of specimens selected, given that we used specimens with a certain hematoxylin and eosin diagnosis of MM and MP, whereas others used difficult cases with overlapping features (19).
Further, the differences were demonstrated in a study conducted by Lindh et al (20) who proved that detection of smoothelin expression in the urinary bladder is strongly dependent on pretreatment conditions. They compared smoothelin expression in cystectomy specimens using 3 different pretreatment protocols:
Heat-induced epitope retrieval (HIER) in alkaline buffer, which resulted in the strongest staining, with a moderate or strong immunostaining of the MP in 100% of cases, but also increased the intensity of MM staining to moderately or strongly stained in 61% of cases; HIER in acidic buffer, which resulted in a suboptimal staining of the MP; Enzymatic pretreatment, which resulted in absent or weak staining.
Lindh et al concluded that smoothelin staining did not discriminate reliably between MP and MM with any of the tested pretreatment protocols (20).
In response to the work by Lindh et al (20), Chakravarthy et al (21) studied smoothelin expression in urinary bladder specimens using HIER in both high and in low pH (9.5 and 6.0) and enzyme antigen retrieval using proteinase K in a trial to find an optimal pretreatment protocol. Intense staining of MP was noted with high pH HIER (pH 9.5), suboptimal staining with low pH HIER (pH 6.0) and absent staining using enzyme antigen retrieval methods (proteinase K). High pH HIER, however, also resulted in moderate to intense staining of MM, which was overcome by titrating the dilution of antibody to 1:500 (21). In conclusion, by modifying their staining protocol, they overcame the problem of double staining and achieved optimal staining in concordance with several other studies (14, 21). Our results were different from those of Lindh et al (20) and others (14, 21), because we found citrate to be the optimal antigen retrieval for smoothelin staining, which was in agreement with the results of others (10, 17).
In the current study, there were no significant associations between smoothelin expression in MP (positivity, intensity and percentage) and the parameters of urinary bladder carcinoma studied.
In the gastrointestinal tract (GIT), smoothelin was differentially expressed in the MP and MM of normal GIT as it showed strong and diffuse cytoplasmic staining in both the inner circular and outer longitudinal layers of MP, whereas MM was either completely negative or only patchily and weakly stained (22). So smoothelin was claimed to be a specific and robust marker for distinction of MP and MM in GIT (23).
As regards vimentin expression, it showed 80% sensitivity and 100% specificity in the present study. A few studies have suggested a role for vimentin in differentiation between MM and MP (14, 16, 24). Loss of expression of vimentin in MP according to our results was not expected, as vimentin was positive in virtually all cells, but this absence of expression agreed with the results of others (14, 16, 24). However, Council et al (14) demonstrated positive vimentin in 1 MP. This could be explained by reexpression of vimentin in muscles during regeneration, as confirmed by Gallanti et al who found reexpression of vimentin in regenerating muscles (25).
It can also be argued that similar developmental and functional considerations may explain the differential vimentin expression patterns of the smooth muscle in these 2 compartments (14, 25).
When we combined moderate to strong smoothelin and negative vimentin, the sensitivity and specificity was raised to 100% for both in differentiating MM from MP, agreeing with the results of Council et al (14, 26). Council et al (14) found that the sensitivity of smoothelin for labeling smooth muscle cells of the MP was 100%, and its specificity was 36% when any intensity of immunoreactivity was considered positive; however, the specificity progressively increased with more intense staining cutoffs, becoming 100% when the cutoff was strong staining. Given that vimentin was only rarely expressed in the smooth muscle cells of the MP, the sensitivity of negative or weak vimentin expression for labeling such cells was 100% but the specificity was only 9%; using a negative immunoreaction as the cutoff increased the specificity to 82%, whereas the sensitivity decreased to 93%.
Conclusions
Differentiation of MM from MP can be made based on histopathological criteria, which are unfortunately overlapping in many cases. The intensity and percentage of smoothelin expression give more specificity (95% for intensity and 85% for percentage) than its mere presence or absence (40%), toward the identification of MP. Moderate to strong smoothelin expression with negative vimentin could be very helpful in difficult and overlapping cases, with a high diagnostic validity.
Footnotes
Financial support: None of the authors has any financial interest related to this study to disclose.
Conflict of interest: The authors declare they have no conflicts of interest.