
Abstract
Background
The lysosomal cysteine protease cathepsin K is involved in bone remodeling and is also expressed in the peritumoral stroma of carcinomas arising from different organs. A new generation of cathepsin K inhibitors blocking the RANKL/RANK pathway are being developed. We sought to investigate cathepsin K expression in a cohort of castration-resistant prostate carcinomas.
Methods
Sixteen cases of castration-resistant disease with at least 5 years of follow-up were selected from a cohort of 280 patients who underwent surgery. Cathepsin K was evaluated on formalin-fixed and paraffin-embedded tissue microarrays with 5 tissue spots per case. These were scored as high 2+ (≥30% of cells), low 1+ (<30% of cells) or zero (absence), distinguishing tumor cells and peritumoral stroma cells. Low (1+) and absence (0) of scoring were interpreted as negative, and high (2+) as positive.
Results
The castration-resistant group was composed of 15 acinar adenocarcinomas and 1 neuroendocrine carcinoma, and all showed at least Gleason score 8 at prostatectomy. Two out of 16 cases (12%) scored positive for cathepsin K in tumor cells; and 5 of 16 cases (31%) scored positive in peritumoral stroma cells. The neuroendocrine and acinar subtypes of carcinoma with positive immunoexpression in neoplastic cells developed bone metastases after 4 and 5 years, respectively, and subsequently died.
Conclusions
Patients affected by castration-resistant prostate carcinoma may be tested for cathepsin K, and a positive strong expression (2+) could be a useful predictive biomarker of response to targeted agents, aiding in the selection of patients eligible for these treatments.
Keywords
Introduction
Cathepsin K is a lysosomal papain-like cysteine protease highly expressed in osteoclasts involved in bone remodeling (1). Cathepsin K is also involved in the maintenance of the homeostasis of the extracellular matrix outside the bone, as suggested by its expression in skin and lung fibroblasts (2). Moreover, cathepsin K is expressed in activated reactive macrophages and in granulomatous disorders including hypersensitivity pneumonitis, sarcoidosis, Wegener granulomatosis, berylliosis and tuberculosis. In neoplasms, cathepsin K is consistently and diffusely expressed in alveolar soft part sarcoma, in a subset of renal cell carcinomas with translocation and in perivascular epithelioid cell tumors (PEComas) carcinomas (3, 4). In a broad survey of tumors, Zheng et al analyzed the expression of cathepsin K and found that 2.7% of carcinomas from various sites exhibited cathepsin K labeling (5). On the other hand, cathepsin K was commonly expressed in mesenchymal tumors including granular cell tumor, melanoma and histiocytic lesions (5). Importantly, cathepsin K has been shown to be expressed in breast carcinoma (6) and has been demonstrated to play an important role in prostate cancer progression (7).
Prostate cancer represents the most frequently diagnosed cancer in North America and is the fourth most common cause of cancer death overall and the second most common cause of cancer death in men (8). Men with recurrent locally advanced or metastatic prostate cancer usually respond to androgen deprivation therapy; however, despite this treatment, most patients experience disease progression within a median of 18-24 months (9). Castration-resistant prostate cancer is defined by disease progression despite androgen deprivation therapy, presenting as 1 or any combination of a continuous rise in serum levels of prostate-specific antigen, progression of preexisting disease or appearance of new metastases. Bone metastasis will occur in 90% of men with castrate-resistant prostate cancer and produce significant morbidity including pain, pathological fractures, spinal cord compression and bone marrow failure (10). These clinical outcomes pose a challenge to the treating clinician, particularly when a multidisciplinary approach is required.
A selective nonlysosomotropic inhibitor of cathepsin K (odanacatib) has been developed for the treatment of osteoporosis, demonstrating a manageable toxicity profile and a promising clinical efficacy (11). Interestingly, preclinical data have shown that cathepsin K inhibitors reduce bone destruction in animal models of breast cancer bone metastasis (12), leading to clinical evaluation of their antitumor effect in cancer metastatic bone diseases (13). Therefore in this study we aimed to evaluate the immunohistochemical expression in a selected cohort of patients with castrate-resistant prostate cancer to understand if there could be a rationale for administration of cathepsin K inhibitors in a subset of such patients.
Methods
Ethics statement
This study was approved by the institutional review board of the University of Verona (code Verona Database no. 89) in accordance with the Helsinki Declaration of 1975. Informed consent was obtained in writing from living patients or relatives for all tissues used in this study from the Urology Clinic.
Case selection
We collected data from 280 consecutive patients treated surgically with radical prostatectomy at our institution between February 2011 and January 2014. We reviewed the clinical data on follow-up, including the development of a castration-resistant disease. The grading groups were defined according to the Gleason score (GS) and pooled as follows: 6, 3 + 4, 4 + 3, 8, 9 and 10. We selected 16 patients who developed castration-resistant prostate carcinoma, and we retrieved slides and paraffin blocks of these cases from the archives of the University and Hospital Trust of Verona. Histological review was performed by expert urological pathologists (G.M., M.B. and E.M.). A tissue microarray (TMA) was built with 5 array cores, measuring 0.6 mm in diameter, for each case, after selecting representative areas of each tumor specimen and 2 normal prostate tissues.
Immunohistochemistry and evaluation of cathepsin K labeling
All tissue samples were fixed in formalin and embedded in paraffin according to standard methods. The TMA slides were immunolabeled with cathepsin K antibody (clone 3F9; Abcam, Cambridge, UK) using previously described methods (14). Heat-induced antigen retrieval was performed using a microwave oven and 0.01 mol/L of citrate buffer, pH 6.0, for 30 minutes. All samples were processed using a Bond Polymer Refine detection system in an automated Bond immunostainer (Vision Biosystem; Menarini, Florence, Italy). Cathepsin K immunoexpression was evaluated as high 2+ (≥30% of cells), low 1+ (<30%) or 0 (absence), distinguishing neoplastic cells and cells from the peritumoral stroma. Low (1+) and absence (0) of expression were interpreted as negative, and high (2+) as positive expression.
Results
The most frequently represented GS was 3 + 4 (38%), followed by 3 + 3 (27%) and 4 + 3 (20%). Forty-two patients (15%) had GS ≥8 prostate cancer; of these 16 developed castration-resistant disease. Histologically, 15 cases of castration-resistant prostate cancer were acinar adenocarcinomas (Fig. 1A), while 1 case was classified as neuroendocrine carcinoma (Fig. 1B). Cathepsin K was expressed in neoplastic cells in 2 out of 16 castration-resistant prostate carcinomas (score 2+), while 5 of 16 (31%) cases expressed cathepsin K in the stroma (score 2+) (Tab. I; Figs. 1 and 2). Positive cells revealed a granular brownish pattern of immunoexpression.
Clinicopathological findings in 16 patients with castration-resistant prostate carcinoma
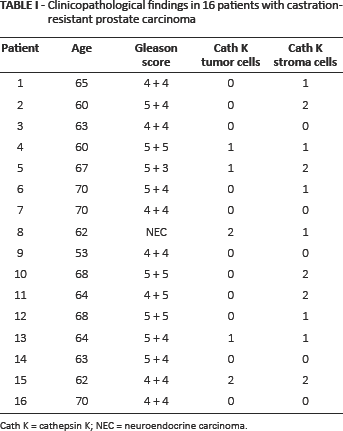
Cath K = cathepsin K; NEC = neuroendocrine carcinoma.
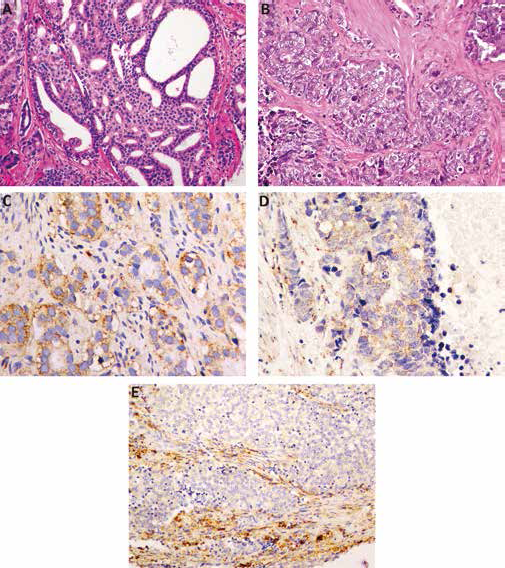
Morphological and immunophenotypical features of prostate carcinoma. (A) cribriform pattern of acinar adenocarcinoma, Gleason score 4 + 4 = 8 (HE, magnification ×20); (B) neuroendocrine carcinoma of the prostate (HE, magnification ×20); (C, D) cathepsin K immunoexpression in acinar adenocarcinoma and neuroendocrine carcinoma (magnification ×40); (E) cathepsin K immunoexpression in peritumoral stroma (magnification ×20). HE = hematoxylin and eosin.
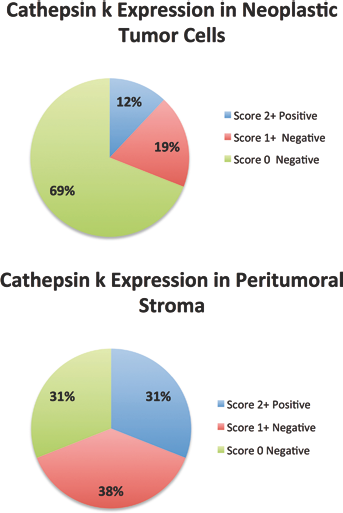
Summarized rate of cathepsin K immunoexpression in neoplastic cells and peritumoral stroma.
The 2 patients whose disease that expressed cathepsin k in the neoplastic cells (score 2+), specifically 1 acinar adenocarcinoma and 1 neuroendocrine carcinoma developed bone metastases after 5 and 4 years, respectively, and subsequently died.
Discussion
The most common site of prostate cancer metastasis is bone. Even though prostate cancer bone metastasis shows a typical osteosclerotic (blastic) phenotype, increased bone resorption is a prerequisite for the seeding of the prostate cancer cells in blastic-predominant bone metastasis. Bone metastasis causes pain, pathological fractures and nerve compression, significantly affecting the patient's quality of life. Despite substantial progress in the understanding of the biology of prostate carcinoma bone metastasis and the great efforts put in the development of new therapeutic agents, treatments so far have had only modest effects on survival and quality of life for patients with metastatic castrate-resistant prostate adenocarcinoma.
Cancer cells that metastasize to the skeleton stimulate the function of bone-degrading cells, the osteoclasts, leading to the formation of malignant lesions. This has provided the rationale for using bisphosphonates or denosumab, as inhibitors of osteoclast-mediated bone resorption in the treatment of patients with bone metastases (15, 16). Denosumab is a fully human monoclonal antibody against RANKL and prevents RANKL from activating its receptor, RANK, thus inhibiting osteoclast formation, function and survival (17). However, bisphosphonates or denosumab do not provide a life-prolonging benefit to the majority of patients with advanced cancer, and new molecules targeting osteoclast activity are therefore required (18).
Cathepsin K belongs to the family of papain-like cysteine proteases and is the principal protease involved in bone remodeling by osteoclasts; its deficiency causes a rare hereditary disease called pycnodysostosis (19); on the other hand, overexpression of cathepsin K in mice results in an accelerated turnover of metaphyseal trabecular bone, which is indicative of increased bone degradation (1). Besides its expression in osteoclasts, cathepsin K can be expressed in tumor cells as well, as is becoming evident in the literature. This is in line with the theory suggesting that cancer cells metastasizing to bone must express bone-related genes to survive in the bone microenvironment (20). Invading breast cancer cells have been demonstrated to express cathepsin K (6) and, more recently, bone marrow macrophages have been identified as the source of cathepsin K associated with prostate cancer metastasis (21). In lung cancer, the levels of cathepsin K expression in epithelial tumor cells and stromal cells were found to correlate with tumor invasiveness (22). Strong cathepsin K expression was also observed in primary melanomas and melanoma metastases (23). This evidence suggested that molecules inhibiting cathepsin K could be useful in the treatment of bone metastases because cathepsin K is not only expressed by osteoclasts but also by bone-residing cancer cells. Le Gall et al demonstrated that following intratibial injection with cathepsin K–expressing human BT474 breast cancer cells, tumor-bearing mice treated with a clinical dosing regimen of cathepsin K inhibitor (CKI; 50 mg/kg, twice daily) had osteolytic lesions that were 79% smaller than those of tumor-bearing mice treated with vehicle, and they concluded that cathepsin K inhibitor reduces breast cancer–induced osteolysis and skeletal tumor burden (12).
One of the first cathepsin K inhibitors to reach clinical development was balicatib, whose skin toxicity (rash and morphea-like skin thickening), which occurred in phase II trials for the treatment of osteoporosis and osteoarthritis, has restricted its further clinical use (NCT00170911, NCT00100607 and NCT00371670). This dermatological reaction seems to be related to the drug's accumulation in the lysosomes, leading to inhibition of cathepsin in dermal fibroblasts and impaired degradation of extracellular matrix proteins (24). To overcome the skin toxicity class side effect of cathepsin K inhibitors, a new selective nonbasic inhibitor of cathepsin K, odanacatib, has been developed which has an insignificant propensity to accumulate in lysosomes, with a minimal potential for the off-target inhibition of non-K cathepsin moieties (25). Interestingly, odanacatib has been shown to suppress bone resorption in patients with breast cancer and metastatic bone disease, suggesting that cathepsin K inhibition may be a valid treatment for this disease (13). Despite these promising results, a phase III trial of odanacatib in prostate cancer patients with metastatic bone disease has been withdrawn prior to enrollment (NCT00691899), and no further evaluation is ongoing in the oncology setting, likely owing to commercial considerations. This study did not include any assessment of cathepsin K expression either in the primary tumor or in bone metastatic tissues. Therefore, the absence of activity of odanacatib could be ascribed to an inadequate molecular selection of patients, suggesting a possible role of this compound in a better defined cohort of patients.
The fact that 2 out of 16 prostate carcinomas (12%) studied in our cohort scored positive for cathepsin K in neoplastic cells, and both those patients developed bone metastases, offers the basis for continuing the evaluation of cathepsin K expression as a predictive factor for castration-resistant prostate carcinoma as well as studying the efficacy of cathepsin K inhibitors in patients with metastatic bone disease. Moreover, in bone metastases, cancer cells could stimulate the expression of cathepsin K by intervening with fibroblasts in the peritumoral stroma that might increase the bone remodeling process and therefore play a crucial role in the growth and invasion of neoplastic cells in the bone. In this regard, Xie et al demonstrated that in squamous cell carcinoma, expression of cathepsin K by stromal fibroblasts was stimulated by the tumor cells via secretion of interleukin-1α and correlated with the invasiveness of the tumor (26, 27). In 5 out of 16 of our cases (31%), cathepsin K scored positive in the peritumoral stroma of prostate carcinomas. The relevance of this result is unclear, and further studies are needed to investigate the relationship between cathepsin K and peritumoral stroma in castration-resistant prostate carcinomas.
The main limitation of this study was the small number of cases evaluated; however, we underscore that our results represent a proof of concept of the potential role of cathepsin K in castration-resistant prostate adenocarcinoma and specifically that its expression may serve as a predictive marker for cathepsin K inhibitors.
Another limitation was that we evaluated the primary tumor and not the metastatic sites; however, one should take into account the fact that it is very difficult to obtain tissue from patients with metastatic bone disease. The use of TMAs may lead to discordant interpretations among different cases; however, the value of TMAs may be sufficient when multiple TMA spots have been used for the overall assessment (28), and notably we punched 5 different parts of the whole prostate adenocarcinoma per case.
Conclusion
This study represents a first evaluation of the expression of cathepsin K in a series of castration-resistant prostate carcinomas, providing a biological rationale for assessing the efficacy of cathepsin K inhibitors in metastatic castration-resistant prostate adenocarcinomas expressing the specific therapeutic target represented by cathepsin K. Our findings should be confirmed in a larger prospective cohort of patients with castration-resistant prostate carcinoma, to better determine the significance of cathepsin K immunoexpression.
Footnotes
Financial support: This study was supported by internal funding from the Department of Diagnostics and Public Health, University of Verona (MB, FUR 2014).
Conflict of interest: The authors declare that they have no competing financial interests.