
Abstract
Introduction
Malignant pleural mesothelioma (MPM) is a relatively rare tumor, with the epithelioid type occurring more frequently. Several biomarkers have been suggested for screening and early diagnosis of MPM. Currently, high levels of soluble mesothelin-related peptides (SMRP), plasma osteopontin (pOPN) and vimentin have been reported in patients with MPM as promising markers for diagnosis, but their clinical use in monitoring is still discussed. The aim of our study was to evaluate the usefulness of these substances as markers of the clinical response to treatment in patients suffering from epithelioid mesothelioma.
Methods
219 serum samples from 56 patients were collected during follow-up and the clinical response to therapy was recorded. Percentage differences between 2 consecutive measurements of SMRP, osteopontin and vimentin (Δ markers) by means of commercially available kits were correlated with changes in the clinical course.
Results
Δ SMRP, Δ pOPN and Δ vimentin showed statistically significant differences between the disease categories stable disease, partial response and disease progression (p = 0.0001, p = 0.035 and p = 0.0025 for SMRP, pOPN and vimentin, respectively). Moreover, contingency table analysis showed statistically significant differences between clinical response and Δ of each marker clustered into 3 groups (<-20%, between -20% and +20%, >+20%).
Conclusions
The time course of Δ SMRP and Δ vimentin was strongly associated with disease status, and so was the time course of pOPN, albeit to a lesser extent. These markers appear to be particularly effective in cases of partial response and disease progression, while their possible use in stable disease should be better investigated.
Introduction
Malignant mesothelioma is a primitive tumor arising from the surface serosal cells of the pleural, peritoneal and pericardial cavities, testicular tunica vaginalis and ovaries. Malignant pleural mesothelioma (MPM) accounts for 90%-95% of all cases, with the epithelioid type occuring most frequently (50%-67%) (1). It is a relatively rare tumor whose incidence in Western Europe is predicted to increase until 2018-2019, related to the widespread use of asbestos in the past (2). At present, no standardized therapeutic protocol is available due to the high rate of relapse and limited survival. Currently, chemotherapy can improve survival (3), whereas the role of early surgery in offering a significant chance of prolonged survival in selected cases is still discussed (4).
Several biomarkers have been suggested as tools for screening and early diagnosis of MPM, including soluble mesothelin-related protein (SMRP), plasma osteopontin (pOPN) and serum vimentin. Several studies have focused on SMRP and pOPN and their role in MPM diagnosis (5–10). Moreover, these markers were also investigated in clinical monitoring of MPM. Robinson et al (6) first observed that SMRP levels decreased after debulking surgery, which was confirmed by Wheatley-Price (11) and Hollevoet et al (12), although on a small number of cases. In contrast to mesothelin, which decreases shortly after resection, pOPN increases, probably because of its role in tissue remodeling (12). Furthermore, osteopontin levels were less closely associated with the radiological response than mesothelin. The role of vimentin in the response to treatment was never analyzed, even if vimentin has been widely used as a diagnostic immunohistochemical marker for MPM (13).
The aim of our study was therefore to evaluate changes in the levels of SMRP, pOPN and vimentin in relation to the course of the disease.
Materials and methods
Patients
This study was performed according to the Helsinki Declaration and was approved by the ethics committee of the University of Pisa.
Fifty-six MPM patients (82.1% males) were enrolled among those admitted to the University Hospital of Pisa for diagnosis and/or therapy. All patients suffered from histologically confirmed epithelioid MPM. Exclusion criteria were non-epithelioid variants of MPM and previous or current malignant diseases other than MPM.
Two hundred nineteen serum samples were obtained from all patients and stored at -80°C. In each patient blood samples were collected every time they underwent a clinical checkup during which disease was restaged. A total of 161 time segments between 2 consecutive serum collections were used to evaluate whether biomarker trends paralleled changes in disease stage (according to RECIST, see below). The aim of our research was to test the utility of some biomarkers as indicators of response to therapy through an experimental design reproducing routine clinical situations. The clinical pathway after a diagnosis of pleural mesothelioma provides, in fact, different monitoring steps, based mainly on radiological investigations, after the provision of different personalized therapeutic treatments. For this reason, the association between marker levels and treatment response was assessed in individual time segments, regardless of the patient and the type of therapeutic treatment. In our study, more time segments per patient were analyzed, with an average of about 3 per patient. In some of the patients with more than 1 time segment analyzed, clinical responses were different for different time segments.
Clinical data
For each patient, we recorded smoking status, asbestos exposure, date of diagnosis, stage according to the International Mesothelioma Interest Group (IMIG) classification (14), date of death (if any), or date of last contact with the patient. Clinical disease course was defined according to the modified response evaluation criteria in solid tumors (RECIST) (15). According to the modified RECIST, a complete response to therapy (CR) was defined as disappearance of all target lesions; a partial response (PR) was defined as reduction by almost 30% of neoplastic disease as assessed by computed tomography (CT); disease progression (DP) was defined as an approximately 20% increase in neoplastic disease or the appearance of new lesions. Patients with stable disease (SD) are not defined by previous criteria. None of the study patients showed CR. RECIST classification was performed by an operator blinded to blood test assessment.
Biomarker assay
SMRP levels were measured using a MESOMARK kit (Fujirebio Diagnostics, Inc.), a sandwich enzyme-linked immunosorbent assay (ELISA) quantitative test (16), according to the manufacturer's instructions. Briefly, patient serum samples were diluted 1:100 with the assay diluent. Next, 100 μL of blank, provided standards and samples were applied in duplicate in a microwell plate precoated with 4H3 antibody. After 1 hour of incubation on a shaking plate at room temperature, the wells were washed and OV569-HRP antibody was added for 1 hour. After a second washing step, TMB substrate solution was added to the wells for 15 minutes, then 100 μL of stop solution was added. Absorbance read at 450 nm was used to quantify the SMRP concentration in nM by comparison of the mean of the duplicate measurement with a calibration curve fitted by the CourbesRD software (Installshield Corporation, Inc.).
The Human Osteopontin Assay Kit (IBL), a commercially available ELISA kit, was used to determine the level of pOPN. Briefly, plasma samples were diluted 1:10 with EIA buffer and 100 μL of blank, standards and samples were applied in duplicate in an O-17 antibody-precoated microwell plate and incubated for 1 hour at 37°C. The plate was washed 8 times and 100 μL of labeled 10A16 antibody was added to each well. After incubation for 30 minutes at 4°C, the plate was washed 9 times and chromogen was added. The plate was incubated for 30 minutes at room temperature in the dark and stop solution was added. Adsorbance read at 450 nm was used to quantify the osteopontin concentration in ng/mL by comparison with the standard curve plotted by a graphic log-log in Microsoft Excel.
The concentration of vimentin in serum samples was detected by a competitive ELISA kit (MyBioSource, cat. MBS721933) using a monoclonal anti-VIM antibody and VIM-HRP conjugate. The assay was performed according to the manufacturer's instructions. Briefly, samples (1:10 dilution) and standards (ranging from 1 to 25 ng/mL) were incubated together with VIM-HRP conjugate in a precoated plate for 1 hour. After incubation the wells were decanted and washed 5 times. The wells were then incubated with HRP enzyme substrate, the reaction was stopped, and the color intensity was measured at 450 nm in a microplate reader. The detection limit was better than 0.1 ng/mL of sample.
All biomarkers were analyzed as percentage changes between 2 consecutive blood collections (Δ) in order to evaluate marker change. All tests were performed by a biologist who was blind to the clinical data.
Statistical analysis
All statistical analyses were performed using SPSS 19.0. Analysis of variance (ANOVA) was used to analyze differences in marker percentages between disease categories (SD, DP and PR). Data were reported as mean and standard deviation, median and 10th-90th percentiles. The chi-square test was performed to evaluate the correlation between marker change (Δ) and clinical disease course. The study population was clustered into 3 Δ groups for each marker (<-20%, between -20% and +20%, >+20%) and, only for SMRP, also 9 groups (variation of 20% from -60% to +80%). Fisher's exact test was used when the analyzed groups comprised fewer than 5 cases. A p value <0.5 was considered statistically significant. The Kaplan-Meier survival curve using the log-rank test was applied to evaluate the prognostic value of SMRP levels at time of diagnosis, using the best cutoff of 1 nM (10).
Results
The demographic and clinical data of all patients are reported in Table I. Of the 56 enrolled MPM patients, 25 had early-stage disease (stage I/II), 16 had advanced disease (stage III/IV), and 15 were incompletely staged.
Demographic and clinical data of study patients

MPM = malignant pleural mesothelioma; SD = standard deviation.
Marker changes and clinical response
SMRP
Δ SMRP showed statistically significant differences between disease categories (SD, PR, DP; p<0.0001). Eighty-two time segments from SD patients showed a Δ SMRP mean of +23.61% ± 85.20%, 30 time segments from PR patients showed a Δ SMRP mean of -20.55% ± 54.88%, and 49 time segments from DP patients showed a Δ SMRP mean of 114.73% ± 168.74%. Case distribution in SD, PR and DP is shown in Figure 1. Contingency table analysis showed statistically significant differences (p = 0.0001) between clinical response (SD, PR and DP) and Δ SMRP clustered in 3 and 9 groups as shown in Tables IIA and IIB, respectively.
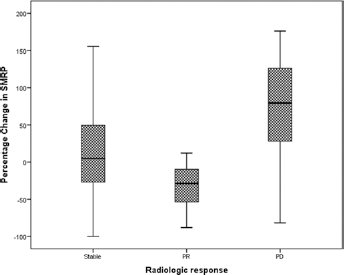
Distribution of stable disease, PR (partial response) and DP (disease progression) in relation to SMRP changes.
Clinical response and Δ SMRP clustered into 3 groups
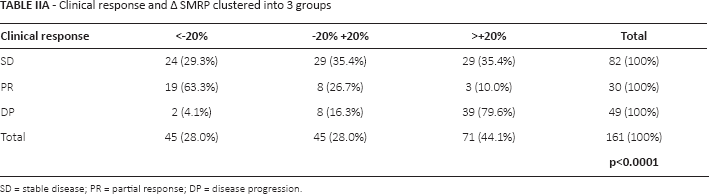
SD = stable disease; PR = partial response; DP = disease progression.
Clinical response and Δ SMRP clustered into 9 groups
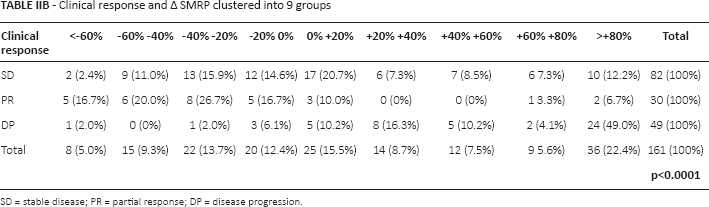
SD = stable disease; PR = partial response; DP = disease progression.
pOPN
In a subgroup of MPM patients (18 cases and 47 time segments), Δ pOPN was analyzed in the 3 different clinical course groups, showing a significant difference with a p value of 0.034 (Δ pOPN mean and standard deviation: -13.72 ± 66.23, -9.68 ± 94.41 and 133.41 ± 300.17 for SD, PR and DP, respectively), as shown in Figure 2. Plasma OPN values in PR cases decreased by almost 20% in as many as 83.3% of patients, while in DP cases these values increased only in 41.7%.
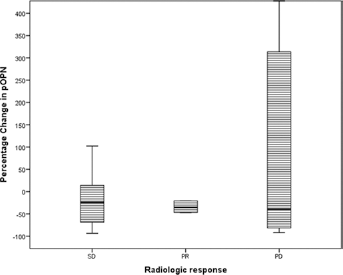
Distribution of SD (stable disease), PR (partial response) and DP (disease progression) in relation to pOPN changes.
Vimentin
In 16 MPM patients with 27 time segment changes, serum vimentin was analyzed in the 3 groups showing a significant p<0.0001 (5.11 ± 10.04, -43.63 ± 15.53 and 45.91 ± 17.51 for SD, PR and DP, respectively), as shown in Figure 3. Regarding vimentin, all PR cases decreased by almost 20%, while in DP cases vimentin increased in 60.0% of the group. Median and 10th-90th percentiles of the percentage changes are presented in supplementary Table S1 (Summary of results: clinical response and Δ markers clustered in 3 groups, with median and 10th/90th percentiles of the percentage of changes, for each line. NA was indicated in case of paucity of subjects. Available online at www.tumorijournal.com).
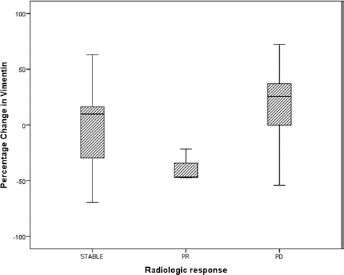
Distribution of stable disease, PR (partial response) and DP (disease progression) in relation to vimentin changes.
Discussion
MPM patients have a poor prognosis with an extremely low 5-year survival rate. There are currently no useful tools for screening and early diagnosis, while clinical monitoring is based mainly on radiological tests. Moreover, evaluation of therapy response in MPM remains difficult, especially because of the poor sensitivity and operator dependency of radiological assessment (4). In addition, in most cases relapse is characterized by a very rapid time course.
Despite the need for new markers of therapy response, up to now only SMRP has been suggested by a few authors. Among these, Hassan et al (17) also demonstrated that SMRP remained stable in patients who did not respond to chemotherapy, suggesting its use as a marker for monitoring the response to therapy. In a descriptive analysis of a series of 37 patients with epithelioid MPM, Grigoriu et al (18) showed that increased SMRP levels were associated with disease progression and poor prognosis, while stable or decreased values correlated with response to treatment irrespective of the type of therapy. Recently, Wheatley-Price et al (11), dividing MPMs in 3 groups with variations of SMRP of about 10%, showed that changes in the percentage of the marker level may play a role in the clinical evaluation of disease course. In that study, 41 nonsarcomatoid mesothelioma cases (2 peritoneal and 39 pleural) were analyzed for the accordance between SMRP level variations and response to therapy evaluated by both the RECIST and modified RECIST criteria, revealing a statistically significant association with both. The results from that study obtained by measuring SMRP in plasma matrices were very interesting, although the kit used for the experiments, MESOMARK, is strongly recommended only for serum matrix.
In our study, we analyzed serum samples strictly according to the manufacturer's instructions, using samples exclusively from epithelioid MPM cases, and we followed the modified RECIST criteria for the evaluation of change in disease status. Actually, there is a considerable body of literature demonstrating that only the epithelioid histological type is associated with increases in the serum SMRP concentration. Moreover, we considered only SMRP changes of about 20%, given the total imprecision of the MESOMARK ELISA kit ranging from 4% to 11% (16).
According to the adopted criteria for disease regression, a decrease in SMRP was observed in 63% (as many as 19 out of 30) of PR time segments. Yet it is noteworthy that regardless the extent up to 80% (24/30), the total PR segments were associated with a decrease in the SMRP concentration. Regarding the 49 time segments of DP, the trend was even more evident, given that 79.6% (as many as 39/49) had increased SMRP values over +20%. SMRP measurements ranging between -20% and +20% showed a less significant correlation with SD, since only 29 of 82 stable time segments (35.4%) fell within the expected range.
SMRP was able to detect DP cases with a sensitivity of 79.6% and a specificity of 74.4%, and to detect PR cases with a sensitivity of 63% and a specificity of 80%.
According to the SMRP results, we found that both pOPN and vimentin were significantly associated with disease course. Regarding pOPN divided into 3 groups, in 29 time segments of SD, Δ pOPN ranged between -20% and +20% in 51.7% of cases (n = 15), while the remaining 48.3% were equally distributed between an increase to more than +20% and a decrease to less than -20%. In PR time segments (n = 6), only 1 case (16.7%) increased over 20%, while the remaining 5 cases (83.3%) decreased by almost 20%. Finally, in 12 DP time segments, Δ pOPN increased in 41.7% of cases (n = 5), decreased in 50% (n = 6), and ranged between -20% and +20% in 8.3% of cases (n = 1).
When Δ vimentin was clustered into 3 groups, in 14 SD time segments, 50% (n = 7) of cases ranged between -20% and +20%, 28.6% (n = 4) decreased, and 21.4% (n = 3) increased. In the PR situation, 100% of time segments (n = 3) decreased by almost 20%. In 10 cases of DP, only 1 time segment (10%) was decreased, 3 time segments (30%) were comprised between -20% and +20%, and the remaining 60% of cases (n = 6) increased over 20%.
Despite the paucity of cases, pOPN but especially vimentin followed the disease course. As for SMRP, pOPN and vimentin were not clearly distributed in case of SD. This difficulty could be due to our choice to set Δ markers in 20% variations, since minor variations in percentage could better describe SD cases.
In conclusion, our data showed that in patients with epitheloid mesothelioma, SMRP, vimentin and (albeit to a lesser extent) pOPN change in parallel with disease status. Our results therefore suggest these substances could be useful as additional markers in monitoring the clinical course of MPM, although further studies are needed to evaluate if marker changes may also have predictive significance.
Footnotes
Abbreviations
Financial support: We thank the Buzzi Foundation for financial support.
Conflict of interest: The authors have no conflict of interest related to this article.