
Abstract
Objective
To explore the relationships of the expression of miR-145 to the clinicopathological characteristics and prognosis of patients with breast cancer complicated by type 2 diabetes mellitus (T2DM).
Methods
A total of 257 female patients with breast cancer were enrolled for our experiment, including 140 patients with simple breast cancer (control group) and 117 patients with breast cancer complicated by T2DM (observation group). Patients were treated with modified radical mastectomy supplemented with radiotherapy, chemotherapy and endocrine therapy. qRT-PCR was used for the detection of miR-145 expression in patients of both groups. Follow-up lasted 13-60 months.
Results
The relative expression of miR-145 in the observation group was significantly lower than that in the control group (p<0.05). The expression of miR-145 in patients with breast cancer complicated by T2DM was related to the history of diabetes, tumor node metastasis (TNM) stage, tumor size, lymph node metastasis (LNM), estrogen receptor (ER) status, and HER2 (all p<0.05). The median disease-free survival (DFS) was significantly longer and the 5-year DFS rate significantly higher in the high-expression group than in the low-expression group. History of diabetes, TNM stage, tumor size, LNM, ER status, and HER2 were risk factors for patients with breast cancer complicated by T2DM (all p<0.05).
Conclusions
Loss of miR-145 expression is related to the development of breast cancer complicated by T2DM, and low miR-145 expression might be an adverse prognostic factor in patients with this disease.
Keywords
Introduction
Breast cancer, the most common malignant neoplasm diagnosed in women, is a chronic disease that is associated with high morbidity and mortality (1). Patients with breast cancer are susceptible to diabetes, and 2 major risk factors for diabetes (old age and obesity) are also associated with breast cancer (2). Two meta-analyses showed a 15%-20% increased risk of breast cancer in women with diabetes, which revealed that the risk could be increasingly higher among women of postmenopausal age (3, 4). Type 2 diabetes mellitus (T2DM) accounts for 90%-95% of diabetes, and its characteristics include hyperinsulinemia in the early phase, insulin resistance, and lack of insulin caused by beta-cell decompensation in the terminal phase (5). It has been assumed that hyperinsulinemia may raise the risk of breast cancer by directly acting on breast tissue or indirectly increasing the circulating concentrations of testosterone, estrogens, and insulin-like growth factors (IGFs) (6). T2DM might adversely affect decisions on breast cancer screening together with treatment allocation, while patients with T2DM can be benefited by breast cancer screening and participation in these programs (7). Recently, a study suggested that changes in the levels of microRNAs (miRNAs) may have important functional consequences in the development of breast tumorigenesis (8).
miRNAs are endogenous small non-coding RNAs (approximately 23 nt) that regulate protein-encoding genes in animals and plants through translational repression or degradation of their target miRNAs (9). Research has suggested that miRNAs play important gene-regulatory roles in numerous key cellular functions including metabolism, proliferation, differentiation development, tumorigenesis, and apoptosis (10). MicroRNA-145 (miR-145) is a highly conserved miRNA that is downregulated in various cancer types including bladder cancer, breast cancer, ovarian cancer and prostate cancer (8, 11-12-13). Additionally, as a novel tumor suppressor miR-145 has a strong inhibitory effect on cancer cell proliferation (14). Previous studies revealed that miR-145 is a tumor-suppressing miRNA and is underexpressed in various types of tumors, and could also cause cell growth inhibition through targeting c-Myc and insulin receptor substrate-1 (IRS-1) (15, 16). In addition, miR-145 could target the pluripotency factors octamer-binding transcription factor 4 (OCT4), SRY-related high-mobility-group (HMG)-box protein-2 (SOX2) and Kruppel-like factor-4 (KLF4), and promote differentiation or repress proliferation of smooth muscle cells (17, 18). Sachdeva et al (19) proposed that low expression of miR-145 is an early event in the progression of breast cancer, and miR-145 could therefore be an early detection biomarker as well as a target for therapy. However, little research has focused on the role of miR-145 in patients with breast cancer complicated by T2DM. Therefore, in this study we aimed to explore the relationships of the expression of miR-145 to the clinicopathological characteristics and prognosis of patients with breast cancer complicated by T2DM.
Materials and methods
Ethics Statement
The study was carried out with the permission of the institutional review board of Yantai Yuhuangding Hospital. Written informed consent was obtained from all participants. Ethical approval for this study conformed to the standards of the Declaration of Helsinki (20).
Study Participants
From January 2011 to December 2014, 257 female patients with breast cancer who were treated at Yantai Yuhuangding Hospital were enrolled for our experiment. The study group included 140 patients with simple breast cancer (control group) and 117 patients with breast cancer complicated by T2DM (observation group). The inclusion criteria were 1) age >18 years and good compliance with systemic therapy; 2) primary breast cancer diagnosed by pathological examination; 3) stage I-III breast cancer according to the tumor node metastasis (TNM) staging criteria established by the American Joint Committee on Cancer and International Union Against Cancer (21); 4) patients in the observation group had to provide information about the time of T2DM diagnosis, hospital of diagnosis, history of drug use, blood glucose monitoring, and control of T2DM. The diagnostic hospital had to be at least a secondary-care hospital, and patients had to meet the diagnostic criteria proposed by the World Health Organization/International Diabetes Federation in 1999 (22): symptoms (diuresis, polydipsia and marasmus) and fasting plasma glucose ≥7.0 mmol/L, or random blood sugar ≥11.1 mmol/L, or plasma glucose ≥11.1 mmol/L with oral glucose tolerance tested for 2 hours. The exclusion criteria were 1) congenital disease, hereditary disease, autoimmune disease or cardiovascular disease; 2) type 1 diabetes, hypertension, kidney disease or other systemic diseases; 3) pregnancy and lactation; 4) heavy smoking, alcohol abuse, drug abuse or a psychiatric history.
Treatment
All patients underwent modified radical mastectomy; the resection volume comprised the breast and the subclavian and axillary lymph nodes at levels I and II. Two weeks to 6 months after surgery, patients received radiotherapy with a SX4XHA900 type electron linear accelerator (Beijing MidWest Technology Co., Ltd.); the radiation field included the lymphatic drainage areas of the chest wall on the affected side, breast, supraclavicle and internal mammary. Patients completed 4-6 cycles of chemotherapy after radiotherapy and the chemotherapy regimens included cyclophosphamide plus therarubicin plus 5-fluorouracil (CTF), cyclophosphamide plus adriamycin plus 5-fluorouracil (CAF), or taxinol plus adriamycin (TA) (Guangzhou Landbiology). Patients with positive estrogen receptors (ER) or progesterone receptors (PR) were given endocrine therapy, such as tamoxifen or aromatase inhibitors.
Quantitative Real-Time Polymerase Chain Reaction (qRT-PCR)
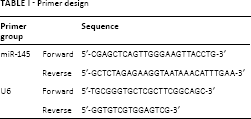
The primer design is shown in Table I. Five minutes after surgery, several epithelial breast cancer tissues measuring 1 cm3 were selected; the tissues were rinsed repeatedly with 0.9% sodium chloride solution and moisture was absorbed with dry gauze. Two tissue samples were put into sterile freezing tubes without RNA/DNA enzymes. RNAlater solution (Invitrogen) was added to the freezing tubes, which were transferred to a -20°C refrigerator for RNA extraction after storage at 4°C overnight. The preserved samples were treated with TRIzol reagent (Invitrogen) to extract total RNA. The obtained 2 μg RNA was reverse-transcribed into single-stranded cDNA with Moloney murine leukemia virus (MMLV) reverse transcriptase and Oligo (dT)15 primer. An ABI PRISM 7000 Detection System (Applied Biosystems) was used to detect the expression of miR-145. The reaction system was 20 μL, including 0.16 μL 5 μmol/L miR-145 upstream and downstream primers, respectively, 10 μL 2 × real-time PCR buffer solution (containing SYBR Green I fluorescent dye [Roche]), 2 μL cDNA template (Applied Biosystems), 0.2 μL 5 U/μL Taq DNA polymerase (MBI Fermentas) and 7.48 μL diethyl pyrocarbonate (DEPC) water. The reaction conditions were as follows: pre-denatured at 95°C for 5 minutes, denatured at 95°C for 10 seconds, annealed at 60°C for 20 seconds, extended at 72°C for 10 seconds, with a total of 40 cycles. U6 (Sigma) was taken as intrinsic parameter. The 2-ΔΔCt method was used to represent the ratio of target gene expression in the observation group and control group: ΔΔCT = ΔCt observation group - ΔCt control group, where ΔCt = CT miR-145 - CT U6 (23).
Primer design
Follow-Up
The time of surgery was set as the initial time of follow-up, and patients in the observation group were followed up using electronic medical records (inpatient medical records, outpatient review of medical records) combined with telephone calls. The follow-up time ranged from 13 to 60 months, and the median follow-up time was 44 months, with a follow-up frequency of once a month. The follow-up contents included general information, clinicopathological characteristics, local or regional recurrence, distant metastasis, and disease-related death. Local or regional recurrence refers to recurrence at the same side of the breast or regional lymph nodes shown by clinical or histological examination. Distant metastasis refers to distant tumor lesions detected by clinical and imaging examination. Disease-free survival (DFS) refers to the time from the first day after surgery to first recurrence or metastasis, and overall survival (OS) refers to the time from the first day after surgery to death or last follow-up.
Statistical Analysis
The SPSS 20.0 statistical software (SPSS Inc.) was used for statistical analysis. Measurement data were expressed as mean ± standard deviation. Comparisons between 2 groups were done with Student's t-test, and comparisons between 3 or more groups were done by means of analysis of variance (ANOVA). Enumeration data were expressed as percentages or rates, and comparisons between groups were performed using the chi-square test. Survival analysis was done by the Kaplan-Meier method and tested with the log-rank test. Multivariate analysis was carried out using the Cox regression model. P<0.05 indicated statistical difference.
Results
General Data
The comparisons of the general data between the 2 groups are presented in Table II. Mean age, body mass index (BMI) and family history of breast cancer were not statistically significant between the 2 groups.
Comparison of general data between study groups
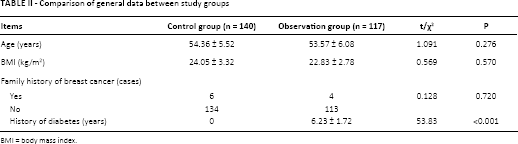
BMI = body mass index.
Comparison of the Expression of miR-145
Comparison of the expression of miR-145 in both groups is shown in Figure 1. The relative expression of miR-145 was significantly lower in the observation group (0.40 ± 0.06) than in the control group (0.68 ± 0.11).
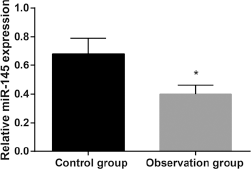
Comparison of the expression of miR-145 in the control group and observation group. *p<0.05 compared with the control group.
Relationships between miR-145 Expression and Clinicopathological Characteristics of Patients with Breast Cancer Complicated by T2DM
The relationships between miR-145 expression and clinicopathological characteristics of patients with breast cancer complicated by T2DM are shown in Table III. The expression of miR-145 in the observation group was related to the history of diabetes, TNM stage, tumor size, lymph node metastasis (LNM), ER status and HER2 status (all p<0.05), but it was unrelated to age, menstrual status, pathological type or PR status.
Relationship of microRNA-145 expression to clinicopathological characteristics of patients with breast cancer complicated by type 2 diabetes
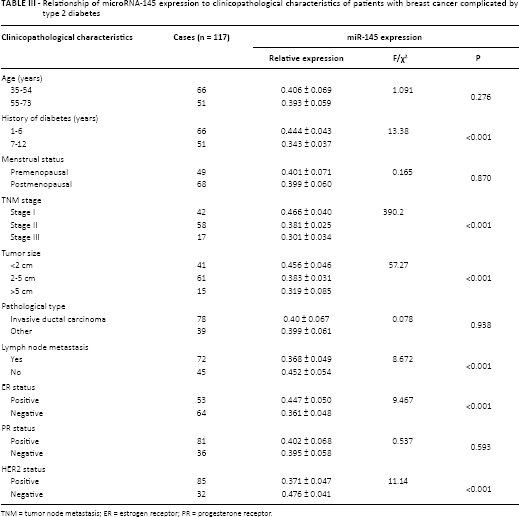
TNM = tumor node metastasis; ER = estrogen receptor; PR = progesterone receptor.
Relationships of miR-145 Expression and Its Influencing Factors to Prognosis of Patients with Breast Cancer Complicated by T2DM
The expression of miR-145 in patients with breast cancer complicated by T2DM was divided into a high-expression group and a low-expression group, taking the median value as the cutoff. The DFS and OS curves of the 2 groups are shown in Figure 2. The median DFS was significantly longer in the high-expression group (53.2 ± 26.1 months) than the low-expression group (43.4 ± 24.6 months) until the deadline of follow-up. The median OS in the high-expression group and the low-expression group was 55.3 ± 23.3 months and 53.0 ± 17.9 months, which was not significantly different. Accordingly, the 5-year DFS rate in the high-expression group (51.72%) was significantly higher than that in the low-expression group (35.59%), while the 5-year OS rates in the high- and low-expression groups were not significantly different at 65.52% and 64.41%, respectively. Multivariate Cox regression analysis for patients in the observation group is shown in Table IV. The factors: history of diabetes, TNM stage, tumor size, LNM, ER status and HER2, all affecting the expression of miR-145 in this group, were analyzed, with the selection criterion of 0.10 and the exclusion criterion of 0.15. The results showed that history of diabetes (χ2 = 5.038, p = 0.025), TNM stage (χ2 = 6.003, p = 0.014), tumor size (χ2 = 9.260, p = 0.002), LNM (χ2 = 8.884, p = 0.003) and ER status (χ2 = 10.868, p = 0.001) were risk factors affecting the survival rate of patients with breast cancer complicated by T2DM.
Multivariate Cox regression analysis for patients with breast cancer complicated by type 2 diabetes
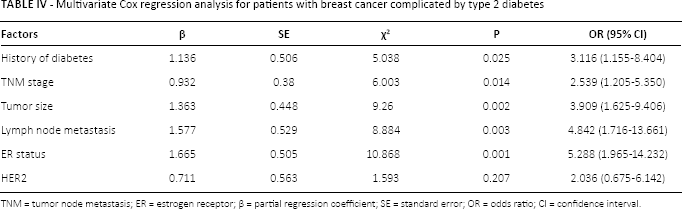
TNM = tumor node metastasis; ER = estrogen receptor; β = partial regression coefficient; SE = standard error; OR = odds ratio; CI = confidence interval.
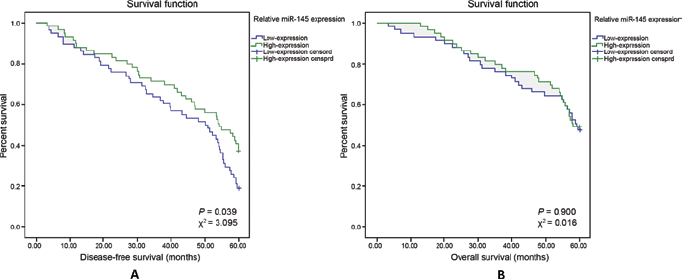
Kaplan-Meier survival curves of miR-145 in the high-expression group and low-expression group. DFS curve for miR-145 expression in both groups (
Discussion
Our study revealed that the relative expression of miR-145 was significantly lower in the observation group than in the control group, implying that low miR-145 expression may be associated with breast cancer complicated by T2DM. miR-145 is located on chromosome 5 (5q32-33), and the nearby 5q31.1 is a very important fragile site. The fragile site is a specific notch or fracture region that occurs on the metaphase chromosome after DNA synthesis is partially inhibited, and a region of unstable genome (24). Fragile sites are usually stable in somatic cells but often absent or rearranged in tumor cells. Therefore, miRNA near the fragile site is closely related to the occurrence of tumors, often accompanied by the loss of metaphase chromosome, which is lowly expressed in tumor tissue (25). A recent study has found that miR-145 inhibits not only tumor formation and growth, but also tumor cell invasion and metastasis (26). Previous studies showed that miR-145 has multiple target gene sites constituting a complex network control system, such as c-Myc, IRS-1 and BCL2/adenovirus E1B 19 kDa protein-interacting protein 3 (BNIP-3); miR-145 can further affect tumor occurrence, development and apoptosis by regulating the activities of these target gene sites (15, 16). It was reported that miR-145 was underexpressed in breast cancer, and that it targeted fascin-1 and mucin-1 in suppressing cancer cell invasion and metastasis (26). Kim et al (27) pointed out that miR-145 levels were lower in breast cancer tissues than their normal counterparts, and miR-145 decreased cell proliferation, migration and invasion of breast cancer through concurrent downregulation of multiple effectors. Recent data showed that miRNAs play a significant role in pancreatic islet development, insulin secretion and beta-cell differentiation, that they can indirectly control glucose and lipid metabolism, and are also involved in complications associated with diabetes (28). Altered miRNA levels can contribute to diabetes at early stages, or can be the result of longstanding diabetes at late stages, and miRNAs can therefore be used as biomarkers for diabetes (29). Additionally, our study suggested that the expression of miR-145 in patients with breast cancer and T2DM was related to a history of diabetes, TNM stage, tumor size, LNM, ER status, and HER2. In agreement with the results of our study, a previous study reported that miRNAs might be involved in breast cancer formation, invasion and metastasis, and that they were associated with TNM stage and prognosis; additionally, disorders in the expression of some miRNAs were related to the clinicopathological characteristics of breast cancer, such as ER status, tumor size, and vascular invasion (30).
Another important finding of our study was that the median DFS and 5-year DFS rate in the high-expression group were significantly higher than those in the low-expression group. However, no statistical difference was found in the median OS or 5-year OS rate between the high-expression group and the low-expression group, which might be explained by the fact that a relatively large number of other deaths and a relatively small sample size influenced our OS results. Therefore, our results of DFS indicate that low miR-145 expression was related to the recurrence and progression of breast cancer complicated by T2DM after treatment, implying that low expression of miR-145 might be used as an indicator of poor prognosis in patents with breast cancer complicated by T2DM, while the OS results in our study had less significance. A history of diabetes, TNM stage, tumor size, LNM, ER status, and HER2 were risk factors for patients with breast cancer complicated by T2DM. A history of T2DM increases the risk of breast cancer and may be related to stimulation of the insulin signaling pathway, changes in endogenous hormones, stimulation of IGF signaling and oxidative DNA damage (31). Therefore, we hypothesize that low miR-145 expression in breast cancer may result in a worse outcome due to T2DM through stimulating the insulin signaling pathway, changing endogenous hormones, stimulating IGF signaling and damaging the oxidation of DNA (7). Breast cancer is a highly heterogeneous malignancy, and ER exists in normal breast epithelial cells; the lack of ER might lead to the dysregulation of tumor growth and proliferation, which further results in a low differentiation grade and poor prognosis of patients (2). HER2 is a commonly used genetic marker that shows obvious amplification and/or overexpression in breast cancer; it is related to histological grade, LNM and TNM stage and is negatively correlated with ER and PR (32). Additionally, complications of diabetes as well as cardiac and cerebral vascular accidents are more likely to occur in the course of treatment for breast cancer complicated by T2DM, which can lead to poor prognosis through affecting antitumor therapy (6). All the above- mentioned factors imply that a history of diabetes, TNM stage, tumor size, LNM, ER status, and HER2 might contribute to some extent to a poor prognosis in breast cancer complicated by T2DM.
In conclusion, our study suggests that loss of miR-145 expression is related to the development of breast cancer complicated by T2DM, and low miR-145 expression is an adverse prognostic factor in patients with this disease. This provides an important basis for improving its prognosis. However, considering that a relatively small sample size and other uncontrollable factors such as a relatively large number of other deaths among patients with breast cancer complicated by T2DM after treatment influenced our results of OS, further studies with a larger sample size and a better experimental design are needed to clarify in depth the association between miR-145 expression and breast cancer complicated by T2DM.
Footnotes
Acknowledgment
We would like to acknowledge the reviewers for their helpful comments on this paper.
Financial support: None.
Conflict of interest: No potential conflicts of interest relevant to this article were reported.