
Abstract
Background
The myeloperoxidase (MPO) -463G>A (rs2333227) polymorphism has been linked with increased susceptibility to the development of various malignancies. However, the data on the association of the MPO -463G>A transition with cervical cancer remain inconsistent.
Methods
Using high resolution melting analysis we genotyped this polymorphism in women with cervical squamous cell carcinoma (SCC) (n = 476) and controls (n = 493) from a Polish Caucasian population. Logistic regression analysis was used to adjust for the effect of confounders such as age, parity, oral contraceptive use, tobacco smoking, and menopausal status, and revealed that the MPO -463G>A single nucleotide polymorphism (SNP) was associated with an increased risk of SCC.
Results
The adjusted odds ratio (OR) for patients with the A/A genotype versus G/G genotype was 0.718 (95% CI 0.531-0.972, p = 0.0316). Stratified analyses between the MPO -463G>A polymorphism and SCC risks demonstrated a protective role of the MPO -463G>A SNP in patients with a positive history of parity and negative history of tobacco smoking. In patients with a positive history of parity, the age-adjusted OR for the A/A versus G/G genotype was 0.667 (95% CI 0.479-0.929, p = 0.0164). The age-adjusted OR for patients with a negative history of tobacco smoking for the A/A versus G/G genotype was 0.491 (95% CI 0.313-0.770, p = 0.0019).
Conclusions
Our study demonstrated that the MPO -463G>A SNP may protect from SCC in women from Polish Caucasian populations.
Introduction
Cervical neoplasia is the second most frequent cancer in women worldwide (1). The development of this cancer is preceded by cervical intraepithelial neoplasia (CIN) (2, 3). CIN is due to infection with high-risk types of human papillomavirus (HPV) (2, 3). The majority of HPV infections are transient and do not result in the development of CIN (4, 5). It seems that the host genetic background as pertains to the host immune response is essential in the duration of HPV infection and subsequent cervical tumorigenesis (5). In addition to HPV, other factors increasing the risk of cervical tumorigenesis have been observed; these include cigarette smoking, multiparity, contraceptive use, age at time of first sexual encounter, social status, and environmental pollution (2, 6-7-8).
Myeloperoxidase (MPO) is secreted by different immune cells including neutrophils and monocytes. MPO belongs to the XPO subfamily of peroxidases, which produce chloride and hydrogen peroxide to form hypochlorous acid, a powerful oxidant (9, 10). Subsequently, hypochlorous acid and superoxide form hydroxyl radicals (11), a strong reactive radical species. MPO also produces free chlorine, which is a potent halogenating factor (12). The reactive radical species are used by neutrophils as cytotoxic agents to strike bacteria, fungi and viruses as well as malignant cells (13-14-15-16). However, the oxidative properties of the MPO-hydrogen peroxide-chloride complex can also be responsible for malignant transformation (16, 17).
The MPO gene in humans is located on chromosome 17q23 and contains many single nucleotide polymorphisms (SNPs) (18). One of these polymorphisms, MPO -463G>A (rs2333227), is related to changes in MPO production (19, 20). Moreover, increased expression of MPO has been linked with increased susceptibility to the development of various malignancies (21-22-23-24-25-26-27-28-29-30).
Higher MPO activity has been observed in gynecological cancers such as ovarian, endometrial and cervical cancer as compared to a group of healthy women (31). In contrast, decreased MPO activity has been identified in the peripheral blood neutrophils of women with cervical tumors, suggesting that women with a reduction or lack of MPO activity can be more susceptible to cervical tumor development (32). Additionally, there is inconsistent data on the MPO -463G>A polymorphism association with cervical cancer (33-34-35-36). The aim of our study was to evaluate the distribution of the MPO -463G>A transition in women with cervical cancer (n = 476) and controls (n = 493) from a Polish population.
Patients and Methods
Study Population
The study population consisted of 476 patients with cervical squamous cell carcinoma (SCC) assessed by stage and histological grade based on the International Federation of Gynecology and Obstetrics (FIGO). Patient data were provided from patients enrolled between August 2008 and December 2014 at the Department of Radiotherapy of the Greater Poland Cancer Center in Poznań, Poland (Tab. I). The control group consisted of 493 unrelated healthy female volunteers. The women with SCC and healthy female volunteers participating in the study were Caucasians from the Wielkopolska (Greater Poland) area of Poland. Informed consent was provided by all participating individuals. The study procedures were approved by the Local Ethical Committee of Poznań University of Medical Sciences.
Clinical and demographic characteristics of patients with squamous cell carcinoma and controls
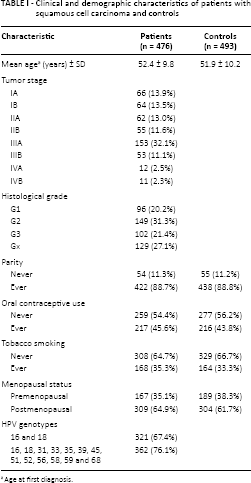
Age at first diagnosis.
Genotyping
Genotyping DNA was obtained from peripheral leukocytes using a salting out procedure. The MPO -463G>A (rs2333227) DNA fragment (132 bp) was amplified using the primers 5’ GGCTGGTCTTGAACTCCTG 3’ and 5’ GAAATCTTGGGCTGGTAGTG 3’. This polymorphism was then genotyped by high-resolution melting curve analysis (HRM) on a LightCycler 480 system (Roche Diagnostics). Of the total samples, 20% randomly selected samples were verified by a commercial sequencing service for the MPO -463G>A polymorphism.
Statistical Evaluation
The differences in genotype and allele distribution between patients and controls and their genotype deviation from the Hardy-Weinberg equilibrium were evaluated using the chi-square test. Moreover, odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Unconditional logistic regression analysis was used to adjust for the effect of confounders such as age, parity, oral contraceptive use, tobacco smoking, and menopausal status. A p value of <0.05 was considered statistically significant. Statistical analysis was conducted with Statistica version 10, 2011 (StatSoft Inc.).
Results
Prevalence of the MPO -463G>A Polymorphism in Women with SCC
The distribution of the MPO -463G>A genotypes did not display significant differences from the Hardy-Weinberg equilibrium and was equal to 0.770 and 0.538 for patients and controls, respectively. The prevalence of MPO -463G>A and adjusted analyses in patients with SCC and healthy women are summarized in Table II. The MPO -463A/A genotype frequency was 1.75-fold greater in controls than cases and was 0.07 and 0.04, respectively. However, we found an almost identical frequency of the MPO -463G>A genotype in both studied groups. The MPO -463A allele frequency was slightly higher in controls than cases, namely 0.24 and 0.21, respectively. Logistic regression analysis revealed that the MPO -463A/A genotype protects against the risk of SCC. The adjusted OR for patients with the A/A versus G/G genotype was 0.718 (95% CI 0.531-0.972, p = 0.0316). However, we did not find a statistically significant association of the A allele with SCC; the adjusted OR was 0.916 (95% CI 0.771-0.916, p = 0.0732). Moreover, there was no significant association of the MPO -463G>A SNP with tumor stage and histological grade (data not shown).
Contribution of the MPO -463G>A (rs2333227) SNP to SCC
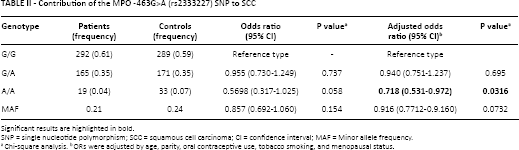
Significant results are highlighted in bold.
SNP = single nucleotide polymorphism; SCC = squamous cell carcinoma; CI = confidence interval; MAF = Minor allele frequency.
Chi-square analysis.
ORs were adjusted by age, parity, oral contraceptive use, tobacco smoking, and menopausal status.
Stratified Analyses of the MPO -463G>A Polymorphism and SCC Risk
The age-adjusted assessment of the MPO -463G>A polymorphism and SCC stratified by parity, oral contraceptive use, tobacco smoking, and menopausal status are indicated in Table III. We found a protective role of the MPO -463G>A SNP in patients with a positive history of parity and a negative history of tobacco smoking. In patients with a positive history of parity, the adjusted OR for the A/A versus G/G genotype was 0.667 (95% CI 0.479-0.929, p = 0.0164). The adjusted OR for patients with a negative history of tobacco smoking for the A/A versus G/G genotype was 0.491 (95% CI 0.313-0.770, p = 0.0019). However, there was no significant correlation of the MPO -463G>A SNP with a positive history of oral contraceptive use or with menopausal status (Tab. III). Moreover, we did not find any association between the MPO -463G>A SNP and tumor stage or histological grade (data not shown).
Stratified analyses between the distribution of MPO -463G>A (rs2333227) genotypes and SCC risks: pregnancy, oral contraceptive use, tobacco smoking, and menopausal status
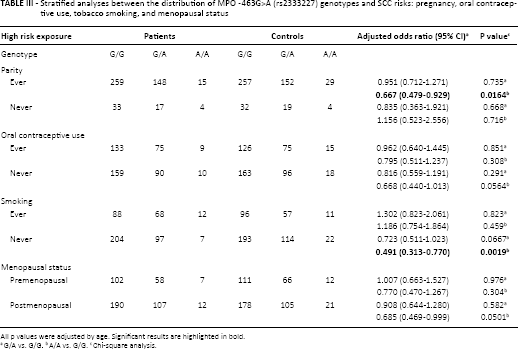
All p values were adjusted by age. Significant results are highlighted in bold.
G/A vs. G/G.
A/A vs. G/G.
Chi-square analysis.
Discussion
The MPO gene encodes an 83-kDa precursor protein that is posttranslationally processed to form 13.5-kDa and 59-kDa subunits (37, 38). These 2 subunits are combined with heme groups to yield the tetrameric enzyme. MPO is located in the lysosomes of polymorphonuclear neutrophils and monocytes, which produce microbicidal reactive oxidants functioning as part of the innate immune system (37, 38). MPO is involved in inflammation and oxidative stress at the cellular level, which accounts for cytotoxic side effects such as damage of the DNA strand, impaired DNA repair, and tumorigenesis (17, 39-40-41). Therefore, polymorphic variants of MPO genes can be related to the development of different malignancies, including cervical cancer.
We observed that the MPO -463A/A genotype had a protective effect in patients with SCC. Moreover, we found a protective effect of the MPO -463A/A genotype in the nonsmoking subgroup and patients with a positive history of parity. In contrast to our studies, Castelão et al (33) demonstrated that women with the G/G genotype had a lower risk of invasive carcinoma. Moreover, several studies did not demonstrate the MPO -463G>A polymorphism to be a risk factor for cervical carcinogenesis. Mustea et al (36) did not find an association of the MPO -463G>A SNP with cervical cancer in 149 Caucasian patients from Moldavia including 14 cases of adenocarcinoma, 4 of adenosquamous cell carcinoma, 130 of SCC, and 1 other histological type. Nishino et al (34) also did not observe any contribution of the MPO -463G>A polymorphism to CIN 3 and invasive cervical SCC in a Japanese population. Recently, Natter et al (35) did not confirm the role of MPO -463G>A in the development of CIN 1-3 in Caucasian women.
The differences between our study, the study by Castelão et al (33) and other studies may be due to the integration of different confounding factors in our study, as well as the genetic heterogeneity between the studied populations.
To date, the MPO -463A gene variant has been recognized as a protective genetic factor in the development of various malignancies. The MPO -463G/A and A/A genotypes appear to have a reduced risk of lung, gastric and ovarian carcinoma, colorectal adenomas, and acute leukemia (21-22-23, 42, 43). The presence of the MPO -463A/A genotype was associated with a decreased risk of breast and bladder cancer (24-25-26). Patients carrying the MPO -463A-allele genotypes also displayed a decreased risk of hepatoblastoma and esophageal carcinoma (44, 45). It has also been demonstrated that there is MPO -463G/G genotype overrepresentation in patients with early stage ovarian, prostate and hepatocellular carcinoma, as well as chronic lymphocytic leukemia and multiple myeloma (27-28-29-30).
The role of the MPO -463G>A transition in the expression of MPO has been documented in several studies. The MPO -463G variant contains the SP1 binding site, which activates transcription by 25-fold in transient transfection assays, while the MPO -463A allele results in several-fold less transcriptional activity (19). Reynolds et al (20) confirmed that the MPO -463G allele forms the SP1 and retinoic acid response element located in the MPO promoter. Moreover, they found that the MPO -463G/G genotype was linked to elevated MPO mRNA levels in primary myeloid leukemia cells (18, 19). In addition to these findings, Saygili et al (27) demonstrated that patients with chronic lymphocytic leukemia and multiple myeloma and the MPO -463G/G genotype had elevated serum MPO levels.
In the present study, the protective role of the MPO -463A/A genotype in cervical carcinogenesis in nonsmoker patients and patients with a positive history of parity may also be related to a lower MPO activity, which reduced DNA damage and carcinogenesis. In contrast, in the smoker group we observed no effect of the MPO -463A/A genotype, which may be due to the strong carcinogenic effect of cigarette components and the MPO -463G/G genotype. The lack of the MPO -463A/A genotype's protective effect in patients with no parity, menopausal status, and a history of contraceptive use can be due to this patient group having a large number of smokers.
We are the first to demonstrate that the MPO -463G>A SNP may protect from cervical SCC in women who are nonsmokers and have had children and are from a Polish Caucasian population; this study should be repeated in other independent ethnicities.
Footnotes
Acknowledgment
The technical assistance of Ms. Agnieszka Hertel is gratefully acknowledged.
Financial support: Supported by grant no. 502-01-01124182-07474 from Poznań University of Medical Sciences.
Conflict of interest: There are no conflicts of interest related to this study.