
Abstract
Background and Aims
Increasing evidence suggests that elevated serum levels of C-reactive protein (CRP) are associated with poor survival in many malignant tumors. However, the prognostic value of CRP in advanced gastric cancer (AGC) remains uncertain. This study was undertaken to evaluate the significance of serum CRP as a biomarker of long-term survival in patients with AGC.
Methods
The serum CRP levels of AGC patients were analyzed for clinicopathological significance. Data were collected retrospectively for 244 patients treated between October 1, 2006 and September 30, 2013. The prognostic effect of serum CRP levels was evaluated.
Results
The baseline CRP level before chemotherapy was significantly associated with overall survival. The median survival was 351 days for patients with CRP ≥10 mg/L and 370 days for patients with CRP c10 mg/L (p = 0.033). Cox analysis revealed CRP to be an independent prognostic factor for overall survival. In the 93 patients whose baseline CRP was ≥10 mg/L, a cutoff point of 22% for the CRP declining rate provided optimum sensitivity and specificity for 1-year survival based on ROC curves. A CRP declining rate >22% was found to predict longer overall survival (410 days versus 299 days; p = 0.001).
Conclusions
Elevated serum CRP baseline levels before chemotherapy were associated with reduced overall survival in patients with AGC. The CRP declining rate was also associated with overall survival. The CRP baseline concentration before chemotherapy and CRP declining rate after chemotherapy may be used as novel, widely available and real-time independent prognostic and predictive markers of AGC.
Introduction
C-reactive protein (CRP) is an acute-phase protein induced by proinflammatory cytokines such as interleukin 1 (IL-1), interleukin 6 (IL-6), and tumor necrosis factor-alpha (TNF-α). It is synthesized by hepatocytes and increases in the presence of inflammatory diseases (1). Circulating serum CRP is often measured in clinical laboratories as a marker for different acute and chronic inflammatory diseases.
There is much evidence showing that chronic inflammation plays an important role in the pathogenesis and development of various tumor types. It is well known that proinflammatory cytokines such as IL-1, IL-6 and TNF-α stimulate CRP production from the liver, which influences survival, growth, mutation, proliferation, differentiation, and migration of tumor cells (2).
Numerous studies reported that increased serum levels of CRP were associated with poor survival in many malignant tumors such as breast cancer (3), colorectal cancer (4), lung cancer (5), prostate cancer (6, 7), renal cell carcinoma (8), and pancreatic cancer (9). Similar results were found in gastric cancer (10-11-12-13). However, there have also been opposite conclusions. Some studies argued that CRP was not an independent prognostic factor for gastric cancer patients at different stages (14, 15). Due to the inconsistent results, the prognostic value of CRP in gastric cancer remains uncertain.
We conducted this retrospective study to evaluate the prognostic effect of CRP on patients with advanced gastric cancer (AGC) who underwent chemotherapy treatment in our institution. Our major goal was to provide some initial evidence to confirm that the baseline serum CRP level before chemotherapy had strong prognostic value, and to explore the predictive value of the CRP declining rate after chemotherapy in Chinese patients with AGC.
Materials and methods
Two hundred forty-four patients diagnosed with metastatic or locally recurrent gastric cancer who were registered at the Second Affiliated Hospital of Soochow University between October 1, 2006 and September 31, 2013 were studied retrospectively. All patients had a pathologically confirmed diagnosis, and staging was carried out according to the tumor node metastasis (TNM) staging system (UICC 2010). Prior palliative chemotherapy was not permitted. Prior adjuvant and/or neoadjuvant chemotherapy was allowed if relapse occurred >6 months after the end of chemotherapy. The main exclusion criteria were as follows: incomplete medical records or refusal of follow-up. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Soochow University. Written informed consent was obtained from all patients.
Chemotherapy Schedule
Patients underwent 1 of 2 treatment regimens: intravenous fluorouracil 2,600 mg/m2 by 24-hour infusion, leucovorin 200 mg/m2 and oxaliplatin 85 mg/m2, repeated every 2 weeks (FLO arm) (16), or liposomal paclitaxel 80 mg/m2 administered on days 1, 8, 15 and 22 by intravenous infusion, and S-1 given as 60 mg twice a day orally on days 1-28 for a body surface area (BSA) >1.5 m2 and 50 mg for BSA *1.5 m2, repeated every 6 weeks (L-PS arm) (17). The chemotherapy courses were repeated every 2 weeks for at least 6 cycles (FLO arm) and every 6 weeks for at least 2 cycles (L-PS arm); treatment was stopped if there was evidence of disease progression or unacceptable toxicity.
Clinicopathological Investigation
The parameters investigated in this study included age, gender, Eastern Cooperative Oncology Group performance status (ECOG-PS), histological type, lymph node metastasis, liver metastasis, and malignant ascites. Clinicopathological parameters were compared between patients with normal serum CRP values and those with an elevated value before chemotherapy.
Crp Measurement
Serum was obtained 1-2 days before each cycle of chemotherapy by peripheral venous puncture. CRP serum levels were measured by methods used in routine clinical examination. Serum levels *10 mg/L were defined as normal.
Statistical Analysis
Differences in clinicopathological parameters between groups were evaluated by the chi-square test (or Fisher's exact test where appropriate) for nominal variables, and Student's t-test for continuous variables. Overall survival was the primary endpoint of the analysis. Survival curves were computed with the Kaplan-Meier method. The hazard ratios (HR) of death and 95% confidence intervals (CI) were estimated using Cox multivariate regression analysis. All statistical tests were 2-tailed, and a p value of less than 0.05 was considered as indicating statistical significance. In addition, analyses were performed using the SPSS software, version 19.0 (IBM SPSS). To evaluate the discriminatory ability of the CRP declining rate, receiver operating characteristic (ROC) curves were generated, and the areas under the curve (AUC) were measured by a software program (MedCalc).
Results
Of the 244 patients with metastatic or locally recurrent gastric cancer included in the study, 93 (38.1%) had high serum CRP values (≥10 mg/L, H-CRP group) and 151 (61.9%) had normal values (*10 mg/L, N-CRP group). The patients ranged in age from 29 to 74 years, with a median of 61 years. Table I shows the relationship between serum CRP levels and clinicopathological characteristics of the patients. Significant differences were found in the frequency of malignant ascites: the H-CRP group had a significantly higher percentage of malignant ascites (35.5%) than the N-CRP group (17.2%) (p = 0.001). There were no significant differences between groups for any other patient characteristics.
Relationship between serum CRP levels and clinicopathological characteristics of the patients
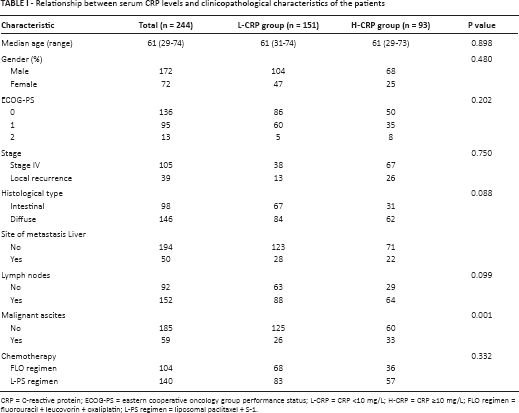
CRP = C-reactive protein; ECOG-PS = eastern cooperative oncology group performance status; L-CRP = CRP *10 mg/L; H-CRP = CRP ≥10 mg/L; FLO regimen = fluorouracil + leucovorin + oxaliplatin; L-PS regimen = liposomal paclitaxel + S-1.
The relationship between clinicopathological characteristics and cancer-specific overall survival are shown in Table II. In univariate survival analysis, age (p = 0.04), ECOG-PS (p = 0.01), CRP (p*0.01), liver metastasis (p = 0.02), malignant ascites (p = 0.01) were significantly associated with cancer-specific survival. In multivariate analysis of the significant variables, ECOG-PS (HR: 2.41; 95% CI 1.46-4.87; p*0.01), CRP (HR: 1.16; 95% CI 1.03-1.28; p*0.01), and malignant ascites (HR: 1.35; 95% CI 1.02-1.81; p = 0.04) were independently associated with cancer-specific overall survival (Tab. II).
Prognostic factors for overall survival identified by univariate and multivariate analyses
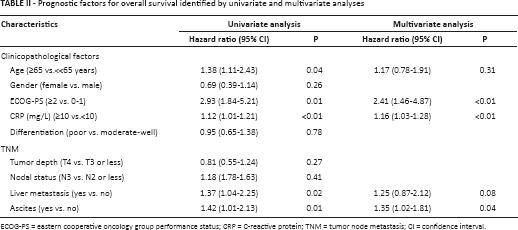
ECOG-PS = eastern cooperative oncology group performance status; CRP = C-reactive protein; TNM = tumor node metastasis; CI = confidence interval.
Association between Baseline Serum CRP Concentration and Overall Survival
The median survival time for the overall population was 359 days (95% CI 347-370). The median overall survival was significantly shorter in the H-CRP group than the N-CRP group (351 days [95% CI 335-367] versus 370 days [95% CI 351-389]; p = 0.033) (Fig. 1).
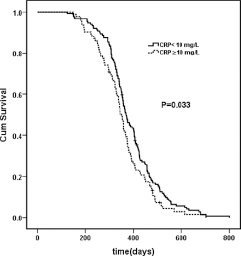
Kaplan-Meier analysis. Elevated baseline serum CRP before chemotherapy is associated with poor survival. Significance was assessed by the log-rank test.
Association between Serum CRP Concentration Declining Rate after Chemotherapy and Overall Survival
To further assess the usefulness of CRP in clinical practice, we statistically evaluated the relationship between the CRP concentration declining rate after chemotherapy and overall survival in the H-CRP group. Each of the 93 patients received systemic chemotherapy for at least 3 months. Applying ROC curve analysis, we determined a cutoff value of 22% for the CRP declining rate to be optimal to predict 1-year cancer-specific survival in patients undergoing chemotherapy. At the threshold of 22%, the sensitivity, specificity and AUC were 80.0%, 86.8% and 0.91, respectively, as shown in Figure 2. The cancer-specific survival curve of the CRP declining rate after chemotherapy (using the cutoff of 22%) calculated from the ROC curve is shown in Figure 3. The median overall survival was significantly longer in the declining rate ≥22% group than <22% group (410 days [95% CI 348-472] versus 299 days [95% CI 266-332]; p = 0.001).
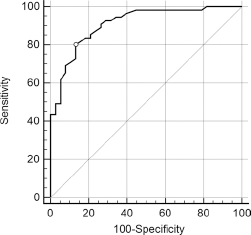
ROC curve for CRP declining rate after chemotherapy (AUC = 0.91). The figure shows the ROC curve of the CRP declining rate for 1-year cancer-specific survival.
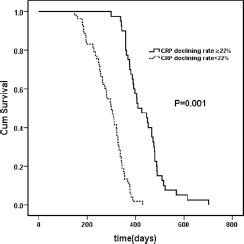
Kaplan-Meier analysis. Lower serum CRP declining rate after chemotherapy is associated with poor survival. Significance was assessed by the log-rank test.
Discussion
During routine clinical work, we usually measure the objective response of solid tumors to treatment according to the WHO criteria (18) or RECIST criteria (19). However, these criteria mainly apply to patients who present with measurable disease, which precludes a considerable number of AGC patients. So a new prognostic and predictive marker that can provide real-time information for patients with AGC is strongly needed.
CRP is an acute-phase inflammatory marker that plays an important role in the host defense reaction. Previous studies have demonstrated that elevated CRP is positively correlated with poor outcome in various solid tumors including gastric cancer (3-4-5-6-7-8-9).
The present study demonstrated that CRP was an independent prognostic factor in patients with metastatic or locally recurrent gastric cancer, along with ECOG-PS, presence of malignant ascites. An elevated baseline CRP concentration before chemotherapy was associated with shorter overall survival (351 versus 370 days; p = 0.033). The mechanism behind the relationship between elevated CRP and poor prognosis in cancer patients has not yet been clarified. The majority of studies indicated that elevated CRP levels may reflect increased concentrations of proinflammatory cytokines that create a microenvironment favoring tumor angiogenesis, proliferation, growth and metastasis (20).
Furthermore, we found that a high serum CRP declining rate after chemotherapy was associated with longer overall survival. The optimal cutoff was 22%, as defined by the ROC curve with an AUC of 0.91, the highest in this study. This cutoff value can be interpreted as a predictive marker of overall survival following chemotherapy. To our knowledge, the present study is the first to define the clinical significance of the CRP declining rate after chemotherapy in AGC. Shimura et al (21) reported that elevated CRP had no significant effect on the response rate to chemotherapy, but was significantly associated with shorter progression-free survival and poorer overall survival compared with CRP <10 mg/L. The authors suggested that chemosensitivity declines more rapidly in H-CRP patients, even if anticancer drugs are temporarily effective. Our present study showed that the CRP declining rate after chemotherapy is associated with overall survival in AGC patients. A CRP declining rate >22% predicted longer overall survival (410 days versus 299 days; p = 0.001). The CRP declining rate might be a meaningful biomarker which can be used in daily clinical routine to predict patients’ overall survival during chemotherapy. Of course, prospective studies are needed to elaborate on this result. The limitations of this study are its retrospective nature, single-center experience, and small number of patients.
In conclusion, we have shown that the baseline CRP concentration before chemotherapy may be an independent prognostic factor for overall survival in patients with AGC. Furthermore, we found that the CRP declining rate was associated with overall survival, and that the cutoff value should be set at 22% in order to determine 1-year cancer-specific survival. The baseline CRP concentration before chemotherapy and the CRP declining rate after chemotherapy may be used as novel, widely available and real-time independent prognostic and predictive markers of AGC. However, large multicenter randomized clinical trials are urgently needed to corroborate these findings.
Footnotes
Abbreviations
Acknowledgment
The authors would like to thank their collaborators for the many useful suggestions and also thank all the patients who participated in the study and their families.
Financial support: Financial support was received from the Science, Education and Health Foundation of Soochow City (KJXW2013017).
Conflict of interest: None of the authors has any financial interest related to this study to disclose.