
Abstract
Background
Diagnosis of medullary thyroid carcinoma (MTC) is still a challenge, and the measurement of calcitonin in fine-needle aspiration (FNA) washout has been recently introduced. Rarely, MTC presents as a cyst and its preoperative detection is difficult.
Methods
A 66-year-old woman was referred to us with high serum calcitonin. Ultrasound evaluation showed one cystic and one solid nodule. FNA was performed in both nodules and calcitonin, procalcitonin and CEA were measured in the aspirate fluids.
Results
The markers showed elevated levels in the FNA washout of the cyst and the patient was operated on. Final histology demonstrated MTC of the cystic nodule. Four weeks later, all serum markers were undetectable.
Conclusions
In the presence of a cystic thyroid lesion the diagnosis of MTC should be taken into account, and measuring calcitonin in FNA fluid is relevant. The determination in FNA of other markers is technically feasible but its role should be evaluated in larger series.
Introduction
Medullary thyroid carcinoma (MTC) accounts for up to 5% of thyroid cancers and 20% of these cancers occur as part of familial disorders (1). The diagnosis of MTC may be complicated for several reasons. In fact, cytology by fine-needle aspiration (FNA) has a low detection rate for MTC and the accuracy of ultrasonography is low (2). Serum calcitonin (CT) measurement is the most reliable tool in this context but has its limits, and its use is still a matter of debate (1). Specifically, no fixed CT thresholds have been proven to diagnose or exclude MTC, and different potential cutoff values may be adopted (1). Thus, a part of MTCs are diagnosed with delay or incidentally discovered after surgery with a consequently poor prognosis. Other tools to detect MTC are required and accurate markers are strongly needed for the postoperative management of these patients (1).
In the last years, serum measurement of several molecules as potential markers of MTC has been reported. Procalcitonin (ProCT) should be considered a reliable marker of this cancer in both preoperative diagnosis and postoperative management (3). Carcinoembryonic antigen (CEA) has traditionally represented a comarker of serum CT, even if with lower accuracy (1). In addition, the measurement of CT in the washout fluids of a nodule's aspiration (FNA-CT) has been reported to increase the accuracy of cytology (4). The data from these studies have been promising and the latest version of the MTC guidelines by the American Thyroid Association (ATA) has introduced this approach with grade B recommendation (see R19: “FNA findings that are inconclusive or suggestive of MTC should have calcitonin measured in the FNA washout fluid and IHC staining of the FNA sample to detect the presence of markers”) (1). To date, only CT has been reported as a thyroid nodule's washout marker, while there were no data of FNA fluid determination of ProCT and CEA. Therefore, no cases with concomitant measurement of all the above-mentioned serum and washout markers have been reported.
Here we report a case of MTC with an initial ultrasound presentation of a purely cystic lesion. The patient underwent several preoperative evaluations and postsurgical examinations. This case report has a certain interest for clinical practice because of the very uncommon initial presentation of MTC at ultrasound.
Case Report
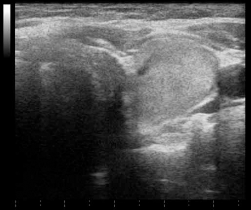
A 66-year-old woman was referred to the Ospedale Israelitico of Rome with a recent incidental finding of multinodular goiter (2 nodules) with normal thyroid function and high serum levels of CT (492 pg/mL). On physical examination both nodules were palpable, having an elastic and hard consistency in the right and left lobe, respectively. No cervical lymph nodes were palpable. The neck was painless. No particular symptoms or signs were recorded. Ultrasound evaluation showed an anechoic and almost entirely cystic lesion in the right thyroid lobe with a greatest diameter of 3.0 cm, well-defined margins, and no vascular signal (Fig. 1A), while a solid isoechoic nodule with a size of 2.5 cm, hypoechoic halo, taller-than-wide shape, and poor peripheral vascularization was present in the left lobe (Fig. 2). No suspicious neck lymph nodes were recorded. Based on these parameters, the cystic nodule was assessed as being at low risk for malignancy and the solid nodule at intermediate risk. During our visit, a blood sample was drawn for measurement of serum ProCT and CEA, and FNA of both nodules was performed. In accordance with the latest ATA guidelines (1), in addition to the cytology specimens a sample from the aspirate washout was prepared for FNA-CT measurement of both nodules.

Cystic nodule of the right thyroid lobe (3 cm) (
Solid nodule of the left thyroid lobe. Histology showed a nonmedullary lesion.
Serum evaluation showed increased levels of ProCT (1.1 ng/mL, normal range <0.1) and CEA (6.4 ng/mL, normal range <4.7). The cytology samples were read by an experienced cytopathologist (LeGu) and the reports were as follows: 1) cystic nodule of the right lobe: suspicious for malignancy “Thy 4” (Fig. 3); 2) isoechoic nodule of the left lobe: indeterminate lesion “Thy 3f”. Remarkably, the volume of the cystic lesion was strongly reduced after aspiration (Fig. 1B). The results of FNA-CT, ProCT and CEA measurement showed high values in the cystic nodule (right lobe) and very low levels in the solid lesion (left lobe), thus suggesting MTC in the cystic nodule of the right lobe and a nonmedullary lesion (i.e., follicular proliferation) in the other nodule (Tab. I).
Preoperative data of serum and washout fluid measurement, and immunochemical examinations of the cystic MTC lesion
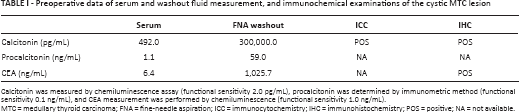
Calcitonin was measured by chemiluminescence assay (functional sensitivity 2.0 pg/mL), procalcitonin was determined by immunometric method (functional sensitivity 0.1 ng/mL), and CEA measurement was performed by chemiluminescence (functional sensitivity 1.0 ng/mL).
MTC = medullary thyroid carcinoma; FNA = fine-needle aspiration; ICC = immunocytochemistry; IHC = immunohistochemistry; POS = positive; NA = not available.
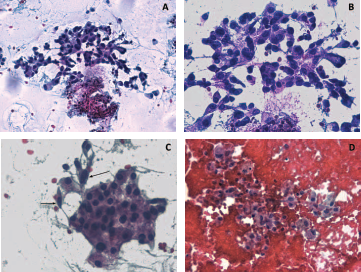
Cytology of the cystic MTC of the right thyroid lobe. Cells exhibit marked pleomorphism in size and shape; note the admixture of small round-type cells and plasmacytoid cells; the nuclei are consistently eccentric (
Accordingly, the patient underwent a total thyroidectomy and central compartment lymph node dissection. The operation was free of complications. Final histology demonstrated MTC in the right thyroid lobe (pT2) and benign follicular adenoma in the left lobe. Immunohistochemistry showed positive results for CT and CEA (not performed for ProCT).
Four weeks after surgery, serum evaluation was performed: CT (<1.0 pg/mL), ProCT (<0.1 ng/mL) and CEA (3.6 ng/mL) were undetectable. Based on these data, the patient was considered biochemically cured and referred for clinical follow-up.
Discussion
Preoperative recognition of MTC is important to better plan the surgical approach. In fact, the prognosis of these patients is influenced by initial treatment (1). While serum CT is the most reliable tool to select patients at risk of MTC, it cannot localize the cancer. In this regard, cytological examination has low accuracy (i.e., 55%-60%), and a nonnegligible rate of false negative cytologies has been reported (2).
We have described a case of MTC with a very rare cystic presentation within a multinodular goiter. A few cases of cystic MTC have been reported (5-6-7-8-9-10-11). The main details of these articles are illustrated in Table II. Twelve cases were described, of which 7 underwent preoperative biopsy. Of the latter, only 1 MTC was identified and localized before surgery (10); in that particular case the authors knew the elevated serum value of CT (169.2 pg/mL) and performed immunocytochemistry for CT, which was positive. Similarly, in the present case we showed that the measurement of CT in washout fluid of the needle after biopsy accurately detected the MTC with cystic presentation and, in addition, excluded the nonmedullary solid lesion of the left lobe. In our patient, the increased serum CT levels were essential to guide the diagnosis of MTC even if the thyroid nodules did not appear suspicious on ultrasound. The measurement of FNA-CT carried out in accordance with the ATA guidelines (1) localized the MTC lesion. A potential weakness of the specific ATA recommendation on FNA-CT might be related to the selection of patients who need FNA-CT. In fact, a universal consensus on the routine examination of serum CT in patients with thyroid nodules has not been reached. Due to the lack of the latter information and the low accuracy of ultrasound in the detection of MTC, a nonnegligible part of patients with MTC should not undergo biopsy; also, about a half of MTC might have inconclusive or false negative results at FNA cytology (2). A possible strategy could be to evaluate serum CT in patients undergoing biopsy, and to use FNA-CT only in those with elevated serum levels. This approach should improve the selection of patients at risk for MTC, allow the use of FNA-CT in the same FNA sample, and, highly relevant in clinical practice, provide useful information to the cytopathologist for careful morphological assessment and tailored application of immunocytochemistry tests, when indicated.
Main characteristics of studies reporting cystic MTC
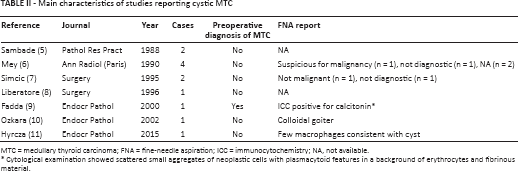
MTC = medullary thyroid carcinoma; FNA = fine-needle aspiration; ICC = immunocytochemistry; NA, not available.
Cytological examination showed scattered small aggregates of neoplastic cells with plasmacytoid features in a background of erythrocytes and fibrinous material.
As mentioned above, no studies reporting the measurement of ProCT and CEA in FNA washout fluid exist. Here we showed that these markers may be elevated in FNA fluids and the potential use of these measurements should be investigated in larger series.
In conclusion, in the presence of a cystic thyroid lesion the diagnosis of MTC should be taken into account. In this context, according to the latest ATA guidelines (1), the measurement of FNA-CT should be used to accurately diagnose MTC and avoid false negative or inconclusive cytology results. The determination of serum CT before biopsy can guide the specific diagnostic procedure and provide essential information to cytopathologists when high CT levels occur. The described case underlines the utility of this approach. Lastly, the measurement in FNA fluids of other MTC markers is technically feasible but its clinical role should be evaluated in larger studies.
Footnotes
Financial support: None.
Conflicts of interest: The authors have no conflicts of interest to declare.