
Abstract
Purpose
To identify conjugated bile acids in gallbladder bile and serum as possible biomarkers for cholesterol polyps (CPs) and adenomatous polyps (APs).
Methods
Gallbladder bile samples and serum samples were collected from 18 patients with CPs (CP group), 9 patients with APs (AP group), and 20 patients with gallstones (control group) from March to November, 2013. High performance liquid chromatography (HPLC) assay with ultraviolent detection was used to detect the concentration of 8 conjugated bile acids (glycocholic acid, GCA; taurocholic acid, TCA; glycochenodeoxycholic acid, GCDCA; taurochenodeoxycholic acid, TCDCA; glycodeoxycholic acid, GDCA; taurodeoxycholic acid, TDCA; taurolithocholic acid, TLCA; tauroursodeoxycholic acid, TUDCA) in bile samples and serum samples. The diagnostic efficacy of serum GCA, GCDCA and TCDCA was evaluated.
Results
These 8 conjugated bile acids in gallbladder bile and serum were completely identified within 10 minutes with good linearity (correlation coefficient: R>0.9900; linearity range: 3.91-500 µg/mL). Among these conjugated bile acids, the levels of gallbladder bile GCDCA and TCDCA in the CP group were significantly higher than those in the AP group (p<0.05). Furthermore, serum GCDCA and TCDCA as well as GCA were significantly higher in the AP group than the CP group (p<0.05). Serum GCDCA alone (≤12 µg/mL) had relatively better diagnostic efficacy than the other conjugated bile acids.
Conclusions
The levels of serum GCA, GCDCA and TCDCA may be valuable for differentiation of APs and CPs.
Keywords
Introduction
The term “polypoid lesion of gallbladder” (PLG) refers to any benign or malignant lesion of the mucosal surface of the gallbladder (1). The reported prevalence of this disease ranges from 0% to 27% depending on the populations and diagnoses (2). As a group, gallbladder polyps include nonneoplastic polyps (e.g., cholesterol polyps, CPs), and neoplastic polyps (e.g., adenomatous polyps, APs) (3). Generally, CPs are benign, measure 8 to 10 mm, and account for the majority (more than 70%) of gallbladder polyps (2). Conversely, APs are neoplastic polyps and have a potential risk of deterioration to gallbladder carcinoma.
Despite the development of imaging modalities such as computed tomography, magnetic resonance imaging, ultrasonography, endoscopic ultrasonography and endoscopic retrograde cholangiography, it is still difficult to distinguish nonneoplastic polyps and neoplastic polyps among PLGs, because the symptoms of PLGs are vague and nonspecific, and many lesions are even asymptomatic (4, 5). Among these methods, ultrasonography is regarded as a sensitive tool in the diagnosis of gallbladder disease (6, 7). For example, both high-resolution ultrasound and endoscopic ultrasonography were reported to have high resolution capability for >1-cm-sized PGLs, with the highest diagnostic accuracies of about 62.9% and 55.5%, respectively (8). However, the resolution capability was relatively poor for PGLs measuring less than 1 cm. Besides, patients may suffer more pain when endoscopic ultrasonography is performed. Usually, pathological examination of the gallbladder after cholecystectomy is the only way to accurately differentiate benign and malignant gallbladder disease. It is well known that an advanced stage of gallbladder cancer indicates a poor prognosis. Therefore, early and effective detection is particularly important for treatment of patients with PLGs.
Bile acids are associated with liver, biliary, and intestinal disease. They are involved in the enterohepatic circulation system and are synthesized from liver cholesterol, secreted by hepatocytes, and stored in the gallbladder. During this process, bile acid molecules convert weak acids into strong acids by conjugating with glycine or taurine, and change into negatively charged bile acid molecules (9). Previous studies have reported that CPs rather than APs were significantly associated with abnormal bile acid secretion (10). Therefore, we believe that abnormal values of conjugated bile acids in peripheral blood serum may be correlated with gallbladder diseases as well.
In the present study, we have compared 8 conjugated bile acids (glycocholic acid, GCA; taurocholic acid, TCA; glycochenodeoxycholic acid, GCDCA; taurochenodeoxycholic acid, TCDCA; glycodeoxycholic acid, GDCA; taurodeoxycholic acid, TDCA; taurolithocholic acid, TLCA; tauroursodeoxycholic acid, TUDCA) in gallbladder bile and serum between patients with CPs and APs using high-performance liquid chromatography (HPLC) in order to find several effective diagnostic markers for identification of CPs and APs. This study will provide novel insight and a convenient method in the differentiation of these 2 diseases.
Materials and methods
Experimental Apparatus and Standards
Agilent-1200 HPLC analyzer and chromatographic column (Eclipse XDB-C18 4.6 × 250 mm, 5 µm, analytical) were purchased from Agilent, USA. Solid phase extraction column (OASIS HLB) was purchased from Millipore, USA. Standard solutions of a conjugated bile acid mixture containing GCA, TCA, GCDCA, TCDCA, GDCA, TDCA, TLCA and TUDCA were obtained from Sigma, USA. Internal standard dexamethasone was from the National Institutes for Food and Drug Control, China. Chromatographic grade acetonitrile and ethanol were purchased from Honeywell, USA. The other reagents were analytically pure.
Study Participants
The study participants were chosen from a group of individuals who were diagnosed as having PLGs or gallstones by B-ultrasonic examination from March to November 2013 at the Department of Pancreatic Surgery, the First Hospital of China Medical University.
The inclusion criteria for patients with PLG were as follows: 1) polyp diameter >1.0 cm; 2) sessile coarse polyps, or polyps located at the gallbladder neck, of which the long pedicle affected gallbladder emptying; 3) rapidly growing polyps; 4) polyp-induced clinical symptoms. Excluded were patients 1) who were diagnosed with diabetes, hyperthyroidism or other metabolic diseases; 2) who had taken cholic acid drugs, nonsteroidal antiinflammatory drugs, hormones or other drugs affecting metabolic functions within the last month; 3) who had a history of liver, gallbladder or biliary tract surgery; 4) who were diagnosed with both polyps and gallstones.
As a result, a total of 47 patients who underwent cholecystectomy were selected. Eighteen patients (5 men and 13 women) aged between 21 and 73 years were diagnosed as having CPs, 9 patients (3 men and 6 women) aged between 32 and 59 years were diagnosed as having APs, and 20 patients (8 men and 12 women) aged between 24 and 83 years were diagnosed as having gallstones. They were classified as the CP group, AP group and control group (gallstone group), respectively.
Gallbladder Bile Preparation
Bile (10 mL) was extracted from the completely resected gallbladder of each patient by fine needle aspiration. After centrifugation at 15,000 rpm at 4°C for 5 minutes, the supernatant bile fluid (100 μL) was added to 900 μL 0.01% formic acid solution and 10 μg/mL of internal standard, followed by vortex mixing for 30 seconds. Prior to sample loading onto the solid phase extraction column, the Oasis HLB (1CC/10 mg) solid phase extraction column was prepared by flushing with 1 mL of each pure methanol solution, 0.01% formic acid, bile samples, 10% methanol, and pure acetonitrile (over 90% transparency). The final mixture of methanol and acetonitrile (2 mL) was collected, resuspended in acetonitrile, filtered with a 0.2-μm filter (Tianjin Heaion Technology Development Co., Ltd, China), and loaded into the vials for testing.
Serum Preparation
Venous blood (10-15 mL) was collected from each patient in the early morning on an empty stomach and was centrifuged at 4°C for 15 minutes to obtain serum. The serum samples (1.6 mL) were mixed with internal standard solution (10 μL, 1 mg/mL) and 0.01% formic acid solution (2.39 mL). The mixture (4 mL) was then vortexed for 30 seconds. Prior to sample loading onto the solid phase extraction column, the precolumn was prepared by flushing with 1 mL pure methanol solution, 0.01% formic acid solution, prepared serum sample, 5% methanol solution, 1 mL pure methanol, and 1 mL pure acetonitrile. A total of 2 mL of the final methanol and acetonitrile eluent was collected. Serum samples (4 mL per patient) were eluted in 4 extraction columns. After elution, the serum samples were evaporated to dryness at 80°C and then cooled at room temperature. They were resuspended in acetonitrile, filtered with a 0.2-μm filter, and loaded into the vials for testing.
Instruments and Chromatographic Conditions
Based on the method described by Coleman et al (11), analysis was performed on an Agilent-1200 HPLC analyzer. A mobile phase containing 10 mmol/L phosphate butter-acetonitrile (solvent A, 80:20, v/v, pH = 3.3) and pure acetonitrile (solvent B) with a flow rate of 1 mL/minute was used. The gradient elution program was as follows: 0 minutes (A:B, 80%:20%), 3 minutes (A:B, 60%:40%), 10 minutes (A:B, 60%:40%), and 15 minutes (A:B, 0%:100%). The wavelength was set at 200 nm and the column temperature was 25°C.
Linearity and Calibration
Standard solutions of a conjugated bile acid mixture (3.09-500 μg/mL, Sigma, USA) containing GCA, TCA, GCDCA, TCDCA, GDCA, TDCA, TLCA and TUDCA were prepared by adding bile samples to acetonitrile solvent (acetonitrile:water = 50%:50%). Calibration curves were constructed according to the ratio of peak areas of the solutes and that of the internal standard (10 μg/mL). For each solute, the linear equation, correlation coefficient and detection limit were analyzed.
Data Processing
The peak areas of each bile acid in serum were calculated by the Agilent software. The concentration of each bile acid was calculated after detection of the internal standard correction, and the average value of 3 detections was calculated.
Statistical Analysis
All variable data were expressed as means ± SD and analyzed by SPSS 19.0 software. One-way analysis of variance (ANOVA) was used for comparison of different groups, and a p value <0.05 was defined as significant difference.
Results
Separation Results of Conjugated Bile Acid
The chromatograms showed that, irrespective of gallbladder bile or serum, the 8 conjugated bile acids in the CP group, AP group, and control group were completely separated within 10 minutes, and there was no interference between the bile acids and the internal standard (Figs. 1-2-3).
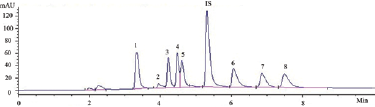
The chromatogram of standard mixture of conjugated bile acids. IS = internal standard; 1 = TCA; 2 = TUDCA; 3 = TCDCA; 4 = TDCA; 5 = GCA; 6 = TLCA; 7 = GCDCA; 8 = GDCA.
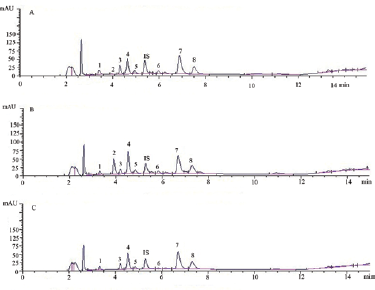
Conjugated bile acids in gallbladder bile in the CP group (
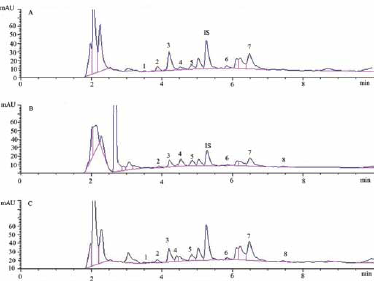
Conjugated bile acids in serum in the CP group (
Standard Curve and Linear Relationship
The regression equations of each conjugated bile acid were presented as Y = aX + b, where Y was the concentration of conjugated bile acid and X was the peak area ratio of conjugated bile acid and internal standard (Tab. I). As a result, all calibration curves of the bile acids showed good linearity with correlation coefficients (R) of more than 0.9900 and a linearity range of 3.91-500 μg/mL.
Standard curve and linear relationship of eight conjugated bile acids
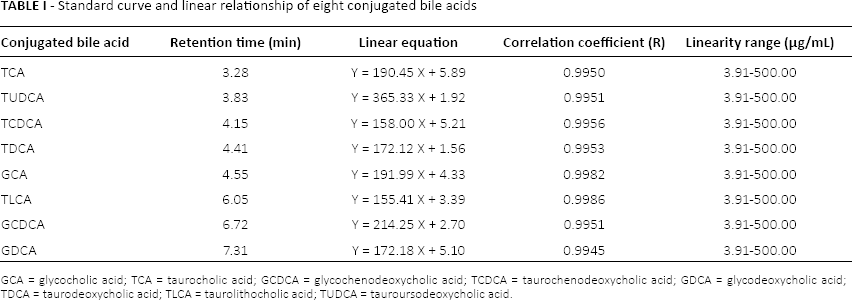
GCA = glycocholic acid; TCA = taurocholic acid; GCDCA = glycochenodeoxycholic acid; TCDCA = taurochenodeoxycholic acid; GDCA = glycodeoxycholic acid; TDCA = taurodeoxycholic acid; TLCA = taurolithocholic acid; TUDCA = tauroursodeoxycholic acid.
Conjugated Bile Acid in Gallbladder Bile Samples
Gallbladder bile samples in the CP, AP and control groups were pretreated with deproteinization for detection of the conjugated bile acid concentration. As shown in Table II, the TCDCA content was significantly higher in the CP group than in the AP and control groups. In addition, the GCDCA concentration was also significantly higher in the CP group than the control group.
Content of eight conjugated bile acids in gallbladder bile (µg/mL)
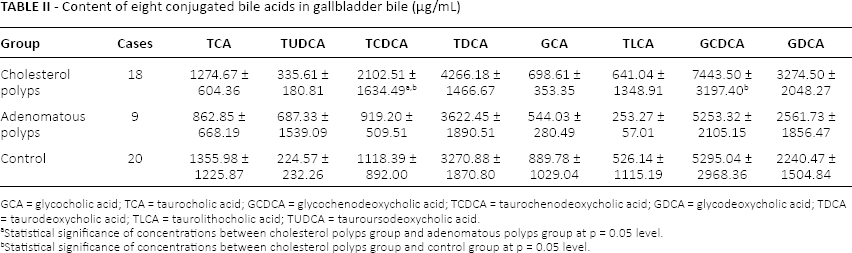
GCA = glycocholic acid; TCA = taurocholic acid; GCDCA = glycochenodeoxycholic acid; TCDCA = taurochenodeoxycholic acid; GDCA = glycodeoxycholic acid; TDCA = taurodeoxycholic acid; TLCA = taurolithocholic acid; TUDCA = tauroursodeoxycholic acid.
Statistical significance of concentrations between cholesterol polyps group and adenomatous polyps group at p = 0.05 level.
Statistical significance of concentrations between cholesterol polyps group and control group at p = 0.05 level.
Conjugated Bile Acid in Serum Samples
The concentrations of conjugated bile acids in serum samples are shown in Table III. The GCA, TCDCA, GCDCA and GDCA concentrations were significantly lower in the CP group than the AP and control groups. However, although the differences in GDCA levels were statistically significant among patients in the 3 groups, GDCA was not detected in some serum samples, nor were TCA and TUDCA.
Content of eight conjugated bile acids in serum (µg/mL)
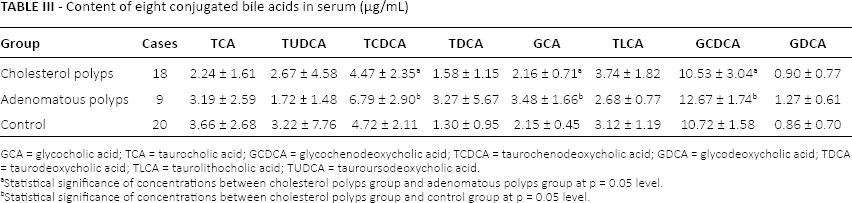
GCA = glycocholic acid; TCA = taurocholic acid; GCDCA = glycochenodeoxycholic acid; TCDCA = taurochenodeoxycholic acid; GDCA = glycodeoxycholic acid; TDCA = taurodeoxycholic acid; TLCA = taurolithocholic acid; TUDCA = tauroursodeoxycholic acid.
Statistical significance of concentrations between cholesterol polyps group and adenomatous polyps group at p = 0.05 level.
Statistical significance of concentrations between cholesterol polyps group and control group at p = 0.05 level.
Diagnostic Efficacy of GCA, TCDCA and GCDCA in Serum
In order to determine the diagnostic efficacy of GCA, TCDCA and GCDCA in PLGs, in the independent marker test we defined GCA ≤2.5 μg/mL, TCDCA ≤5 μg/mL and GCDCA ≤12 μg/mL, respectively, as indicative of the occurrence of CPs. We further estimated if the diagnostic efficacy could be improved when 2 or 3 of the markers were combined in parallel and serial tests. The diagnostic efficacy is summarized in Table IV. The sensitivity, specificity, positive predictive value and negative predictive value were 77.78%, 66.67%, 82.35% and 60%, respectively, for GCDCA, which were higher than those of GCA (66.67%, 66.67%, 80% and 50%) and TCDCA (72.22%, 66.67%, 81.25% and 54.55%). The parallel test groups had relatively higher sensitivity and negative predictive value than the serial test groups, whereas the specificity and positive predictive value were relatively low.
Summary of diagnostic efficacy of GCA, GCDCA and TCDCA (%)
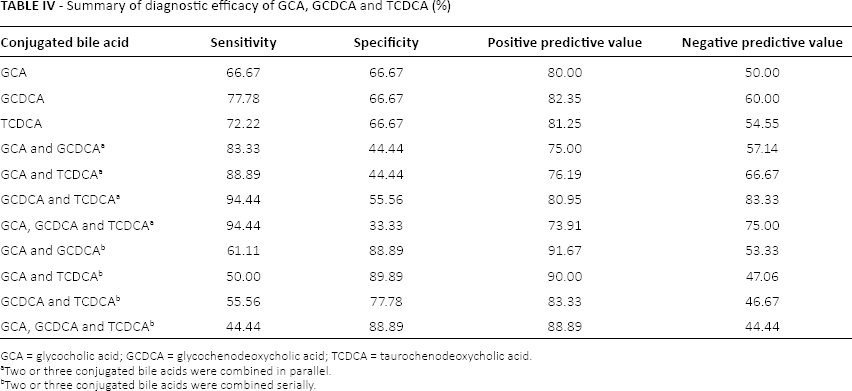
GCA = glycocholic acid; GCDCA = glycochenodeoxycholic acid; TCDCA = taurochenodeoxycholic acid.
Two or three conjugated bile acids were combined in parallel.
Two or three conjugated bile acids were combined serially.
Discussion
Preoperative identification of CPs and APs among PLGs is a key step for clinical treatment. An ambiguous identification will result in unnecessary cholecystectomy or even loss of the best treatment opportunity. The results of our study showed that the gallbladder bile GCDCA and TCDCA levels were significantly higher in CP patients than in AP patients and patients with gallstones. By contrast, these 2 conjugated bile acids as well as GCA in serum were much lower in patients with APs than those with CPs. We assumed from these results that there were significant associations between these conjugated bile acids and CPs. Moreover, these bile acids might be valuable for the diagnosis of CPs. To further assess the diagnostic efficacy of GCA, GCDCA and TCDCA, we calculated the sensitivity, specificity, positive and negative predictive values, and found that TCDCA had better diagnostic efficacy than the other markers.
Bile acid metabolism consists of 3 phases: bile acid synthesis in the liver, conjugation in the intestine and liver, and transportation in the liver, kidney and intestine. It was reported that the cholesterol 7α-hydroxylase (CYP7A1) and microsomal sterol 12α-hydroxylase (CYP8B1) affect the rate of bile acid biosynthesis and the ratio of bile acid to chenodeoxycholic acid (CDCA), respectively (12). After synthesis, most of the bile acids are conjugated to amino acids, and are prepared for efficient transportation and detoxification (13). During transportation, conjugated bile acids are secreted into bile and stored in the gallbladder. Therefore, when a gallbladder lesion occurs, the conjugated bile acid content will change correspondingly.
The formation of CPs is closely associated with dysfunction of hepatocyte secretion. It is characterized by the accumulation of triglycerides and cholesterol esters in the epithelial cells of gallbladder submucosa (10). During this process, these accumulated substances will be phagocytized by macrophages and a number of foam cells will be generated. As a result, the surface of the gallbladder mucosa will have a polyp-like appearance with swollen mucosal villi. The natural history of CPs is therefore benign, without any prominent symptoms. This suggests that cholecystectomy is unnecessary in this condition, and a wait-and-see policy is advised (14). In our study, the levels of TCDCA and GCDCA in gallbladder bile of CP patients were much higher than those in AP patients, indicating that these conjugated bile acids may be associated with CPs. In fact, TCDCA has been reported to enhance phagocytic activity (15) and thus lead to the deterioration of PLGs. A high level of TCDCA in gallbladder bile and serum indicates PLG deterioration. Besides, GCDCA is regarded as a main toxic component of bile acids in patients with PLGs (16). Experimental evidence has shown that mitochondrial dysfunction plays an important role in the pathogenesis of liver cholestasis and bile acid metabolic abnormality (17). We believe that altered GCDCA in gallbladder bile is related to the pathogenesis of CPs through the mitochondrial pathway.
There is apparently no concordance between serum and gallbladder concentrations of some bile acids. For instance, the TCDCA concentration in gallbladder bile was significantly higher in patients with CPs than in those with APs, while TCDCA was higher in serum of patients with APs. We explained this phenomenon based on 2 aspects. On the one hand, most of the bile acid is stored in the gallbladder and little will be transported to the intestinal tract. On the other hand, serum bile acid is derived from bile acid that was not absorbed by hepatocytes. Thus the enterohepatic bile acid circulation contributes to the difference of some bile acid concentrations in serum and gallbladder bile.
It is well known that obtaining gallbladder bile is painful to patients. If markers can be identified in blood, the diagnosis of CPs and APs will be convenient and simple. The present data showed a significant increase in serum GCDCA and TCDCA in patients with APs, suggesting an association between these conjugated bile acids and APs. Though the GCA content in gallbladder bile showed no significant difference between patients with CPs and APs, the GCA content in serum was found to be significantly different. In fact, a recent study has suggested the diagnostic value of GCA for intrahepatic cholestasis of pregnancy (18). However, the authors of this study did not mention the underlying pathogenetic mechanism between GCA and this disease. The reason for the decrease in serum GCA, GCDCA and TCDCA in patients with CPs is not known, which will therefore need to be clarified in future studies.
It is of great concern to enhance the diagnostic accuracy between benign polyps and malignant polyps, because the malignant APs have a poor prognosis (19). In the present study, the diagnostic efficacy was much better for GCDCA than the other markers, with sensitivity, specificity, positive and negative predictive values of 77.78%, 66.67%, 82.35% and 60%, respectively. These results suggest that GCDCA can be used as one of the diagnostic markers for PLGs. Although the GCDCA test combined with the TCDCA test increased the diagnostic rate with high sensitivity (94.44%), the low specificity (55.56%) indicated that this combination is prone to misdiagnosis. Conversely, serial GCA and GCDCA testing can significantly reduce the misdiagnosis rate due to its high specificity (88.89%). Despite the efficacy of these diagnostic schemes, patients having CPs should be observed regularly for timely treatment in case the polyps become symptomatic.
One limitation of this study is the small sample size without confounding factor samples, which might narrow the applicability of the diagnostic markers. In addition, our results showed large standard deviations for all measurements, indicating wide variation between the 2 groups of patients. Therefore, there is a need to confirm our results with more patients and expanding inclusion criteria in future clinical trials. Furthermore, it will be more convincing to include controls with no gallbladder diseases.
In conclusion, the levels of serum GCA, GCDCA and TCDCA were considerably higher in patients with APs than in patients with CPs, suggesting that the accumulation of these conjugated bile acids in serum might be valuable for the differentiation of APs and CPs. With the increasing popularity of HPLC technology, testing the levels of serum conjugated bile acids (GCA, GCDCA and TCDCA) will be simple and convenient for diagnosis of APs and CPs in patients with PLGs.
Footnotes
Financial support: Project supported by the Natural Science Foundation of Liaoning Province (2013021093).
Conflict of interest: All authors declare that they have no conflict of interests related to this work.