
Abstract
Background
Because of the numerous limitations of prostate-specific antigen (PSA), α-methylacyl-CoA racemase (AMACR) and hepsin have recently been suggested as potential biomarkers in prostate cancer (PC). This report presents a comparison study of the presence of AMACR and hepsin in urine collected before and after digital rectal examination (DRE) as a previously suggested diagnostic marker for PC.
Methods
Seventy-six urine samples (38 before and 38 after prostate massage) from patients with benign prostate hyperplasia (BPH) and 66 urine samples (33 before and 33 after prostate massage) from patients with PC were analyzed. PC was confirmed by prostate biopsy. Urinary levels of AMACR and hepsin were determined by ELISA and related to the tumor stage, Gleason score and PSA level.
Results
AMACR and hepsin levels in urine collected after prostate massage were higher only in the PC group. There were no correlations between AMACR levels, hepsin levels, tumor stage and Gleason score. AMACR and hepsin did not differentiate between BPH and PC with better true positive and false negative rates than serum PSA.
Conclusions
AMACR and hepsin were unable to diagnose PC with better true positive and false negative rates than PSA. An additional procedure combined with other markers should be applied for the reliable diagnosis of PC.
Introduction
Prostate cancer (PC) is the fifth most common cancer overall and the second most common cancer in males (1-3). In 2008, a total of 900,000 males were diagnosed with PC, accounting for 14% of cancers in males and 7% of cancers overall. Recent years have seen a considerable increase in the incidence of PC in many countries worldwide, with little change in PC-related mortality. PC is the sixth most common cause of cancer-related deaths in males worldwide. In 2008, the number of PC-related deaths was estimated at about 258,000 (4).
Digital rectal examination (DRE) is the fundamental method of prostate examination in addition to medical history. DRE is helpful in evaluating prostate volume, which is useful in the work-up of prostatitis, benign prostatic hyperplasia (BPH) and PC. Evaluation of serum levels of prostate-specific antigen (PSA) is also useful in the diagnosis of PC. PSA has been used for many years during preliminary work-up of patients over the age of 45 years, and high levels of this antigen in the serum form the grounds for further diagnostic evaluation. PSA is a proteolytic glycoprotein that liquefies semen. It is mainly produced by epithelial cells of the prostate and, in much lower quantities, by epithelial cells of the seminiferous vesicles, urinary bladder and urethra. The fact that malignant cells are not the only cells that produce PSA poses a considerable problem in using it as a PC marker. Elevated PSA is also observed in prostatitis and BPH. Evaluation of serum PSA is therefore associated with a considerable risk of obtaining false results. New, more specific biomarkers are therefore being looked for extensively to replace the currently used PSA in the diagnostic process for PC (5-7).
α-Methylacyl-CoA racemase (AMACR) belongs to the isomerase family. This enzyme is responsible for converting R-stereoisomers into S-stereoisomers and is involved in branched fatty acid beta-oxidation (8, 9). It has been demonstrated that changes in the concentration and activity of this enzyme may be associated with various pathologies, such as nervous system diseases and tumors (10-12). This peroxisomal and mitochondrial enzyme was also found to be up-regulated in PC (8, 9). To evaluate the diagnostic efficacy of AMACR, a total of 96 patients were examined by prostate needle biopsy. The AMACR result was positive in 68 out of 70 patients diagnosed with PC. Sensitivity and specificity were calculated as 97% and 100%, respectively (8). Another study has shown AMACR as a potential biomarker with the use of a noninvasive screening test in voided urine. The conclusions were based on the determination of AMACR in voided urine specimens collected from 26 men after transrectal ultrasound guided prostate biopsy for suspected malignancy (13).
The human serine protease hepsin is a cell surface serine protease that is markedly up-regulated in human PC. But the problem is that the functional significance of this up-regulation is still unknown. Overexpression of hepsin in a mouse model of PC has no impact on cell proliferation, but causes disorganization of the basement membrane and promotes primary PC progression (14). Hence, hepsin may be regarded as a novel potential immunohistochemical marker for the histopathological diagnosis of PC (15).
Few studies have been published on the use of AMACR and hepsin levels in various biological samples as potential markers of PC. We therefore conducted a study to evaluate AMACR and hepsin levels and find out whether changes of AMAR and hepsin levels in urine before and after prostate massage could be used in the routine diagnostic evaluation for PC.
Materials and Methods
Sample Collection
Urine samples were obtained from patients qualified for a surgical procedure in the Department of Urology, Jan Biziel University Hospital in Bydgoszcz, Poland. For this study, 2 main groups of patients were formed: the cancer group (n = 33) consisted of patients diagnosed with PC admitted to hospital for a radical prostatectomy (RP), and the BPH group (n = 38) consisted of patients admitted to the hospital for a transurethral resection of the prostate (TURP). Patients selected for the BPH group had negative DRE and showed no evidence of malignancy in prostatic tissue collected after TURP. All diagnosis were confirmed by histopathological examination of prostate gland tissues as part of routine hospital procedures. Prostate volume of the glands collected after RP was measured by a pathologist. In the BPH group, it was measured using transrectal ultrasound. Because the study sought to determine whether prostate massage has an effect on urine concentrations of AMACR and hepsin, only patients that had not had a prostate biopsy or other urological procedure in the past 30 day prior admission to the hospital were asked to participate in this study. Two urine samples were collected from each patient. First urine sample was collected in the early morning hours in a sterile urine container. The second sample was collected after prostate massage performed by the urologist. Prostate massage was performed by sweeping each lobe 3 times, depressing the prostate gland (0.5-1 cm) in a milking action. All samples were prepared for storage immediately after collection. Sodium azide solution was added to urine with final concentration of 1 mM in urine. Then samples were divided into smaller portions, stored at −80°C and kept in those conditions until further analysis. All actions regarding diagnostics were conducted according to the “Guidelines on the Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), Including Benign Prostatic Obstruction (BPO),” by the European Association of Urology.
Determination of human AMACR and Hepsin
For determining AMACR and hepsin levels, 2 separate ELISA kits were used. The Human AMACR ELISA Kit (EIAab Human Alpha-methylacyl-CoA racemase, Catalog No. E0993h; EIAab) Wuhan, China and the Human Serine Protease Hepsine Elisa Kit (EIAab Human Serine protease hepsin, Catalog No. E1856h; EIAab) were used for determination of AMACR and hepsin in urine. Wuhan, China Ninety-six well plates of immunoassay kit were precoated with an antibody specific to each protein. All samples and standards were transferred to the wells with a biotin-conjugated polyclonal antibody specific to AMACR and human serine protease hepsin. The pretreatment of samples and measurements were performed following the protocol provided by EIAab. Spectrophotometric measurements were performed by microplate reader set to 450 nm. Serial dilutions were prepared from a 100 ng/mL stock solution; the standard curve range was from 1.56 to 100 ng/mL for AMACR and from 0.78 to 10 ng/mL for hepsin.
Statistical Analysis
Statistical analysis and graphical presentation of results were performed using Statistica, version 10 (StatSoft, Tulsa, OK, USA) with the medical analyses package. The Mann-Whitney test was used for between-group comparisons. For statistical purposes, patients diagnosed with PC were stratified by Gleason score (scores 5-7) and by stage (pT2a, pT2b, pT2c). The diagnostic potential of AMACR, hepsin and PSA was determined using receiver operating characteristic (ROC) curves.
Ethical Approval and Signed Consent
The study was approved by the local ethics committee (Collegium Medicum Ethics Committee, #KB66/2011). All patients signed documents regarding their voluntary participation in this study. Sample collection was performed between January and June 2011.
Results
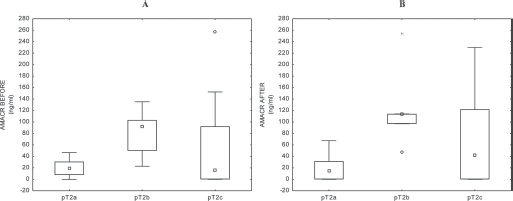
A total of 66 urine samples from patients with PC and 76 from patients with BPH were analyzed. Table I presents the characteristics of the study population, including the numbers of patients, age, serum PSA levels, tumor volume and AMACR and hepsin levels before and after prostate massage. Both study groups were characterized by a similar age: mean age was 62 and 65 years in the PC and BPH groups, respectively. Regarding the tumor state, the PC group consisted of 8 patients with pT2a tumors, 5 patients with pT2b tumors and 20 patients with pT2c tumors. The patients were also stratified by Gleason score: there were 8, 13 and 12 patients with a Gleason score of 5, 6 and 7, respectively. The mean and median serum PSA levels were lower in BPH patients than in PC patients. Serum PSA levels in the BPH group were <4 ng/mL in 22 patients, 4-10 ng/mL in 15 patients and >10 ng/mL in 1 patient. Serum PSA levels in the PC group were <4 ng/mL in 3 patients, 4-10 ng/mL in 26 patients and >10 ng/mL in 4 patients.
Characteristics of study population
AMACR = α-methylacyl-CoA racemase; PSA = prostate-specific antigen.
Alpha-methylacyl-CoA Racemase
The lowest AMACR level possible to be measured in the sample was 1.56 ng/mL, which resulted from the assay limitation. AMACR levels were below this value in 13 samples collected before prostate massage in the BPH group. In the PC group, 8 patients had AMACR levels below 1.56 ng/mL. AMACR levels below the limit of quantitation were present in 22 samples collected after prostate massage in the BPH group. In the PC group, again, 8 patients had AMACR levels below 1.56 ng/mL. A comparison of the samples collected before prostate massage between the BPH and the PC groups did not show any statistically significant differences. When these 2 groups were compared in terms of AMACR levels after prostate massage, these levels were significantly higher in the PC group (p<0.0001) (Fig. 1). To obtain more detailed data, the PC group was stratified by Gleason score. Median AMACR levels were 16.57, 26.32 and 55.12 before prostate massage and 23.81, 24.68 and 108.37 after massage in patients with a Gleason score of 5, 6 and 7, respectively. It was observed that only when comparing samples after prostate massage in patients with a Gleason score of 7 were the levels of AMACR significantly higher than those in patients with a Gleason score of 6 (p = 0.038) (Fig. 2). Patients were also stratified by tumor stage. Median AMACR levels were 19.65, 92.55 and 15.15 before prostate massage and 15.3, 113.32 and 41.63 after prostate massage in patients with pT2a, pT2b and pT2c tumors, respectively. No statistically significant differences were observed (p>0.05) (Fig. 3). A ROC analysis was performed to compare the diagnostic potential of AMACR versus PSA. At the cutoff point of 11.7 ng/mL for AMACR levels, true positive and false negative rates were 75% and 26%, respectively (area under the curve [AUC] = 0.748; 95% confidence interval [95% CI], 0.63-0.865) (Fig. 4). For comparison, a ROC curve for serum PSA levels was also constructed. The true positive and false negative rates for the cutoff point of 4.01 ng/mL were 91% and 39%, respectively (AUC = 0.769; 95% CI, 0.659-0.879) (Fig. 4).
Group comparison of α-methylacyl-CoA racemase (AMACR) concentrations in urine before and after prostate massage.
Comparison of α-methylacyl-CoA racemase (AMACR) levels in urine collected before after prostate massage in cancer patients with different Gleason scores.
Comparison of α-methylacyl-CoA racemase (AMACR) levels in urine collected before and after prostate massage in cancer patients with different tumor stages.
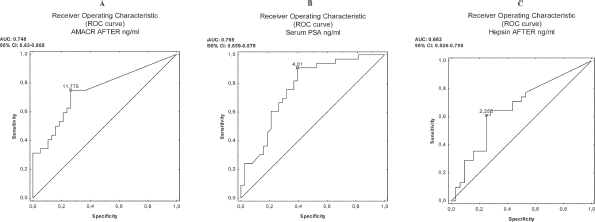
Comparison of diagnostic potential of serum prostate-specific antigen (PSA), α-methylacyl-CoA racemase (AMACR) and hepsin using ROC curve. AUC = area under the curve.
Human Serine Protease
The lowest hepsin level possible to be measured in the sample was 0.78 ng/mL, which resulted from the assay limitation. Hepsin levels were below this value in 12 samples collected before prostate massage in the BPH group. In the PC group, 11 patients had hepsin levels below 0.78 ng/mL. Hepsin levels below the limit of quantitation were present in 15 samples collected after prostate massage in the BPH group. In the PC group, again, 9 patients had hepsin levels below 0.78 ng/mL. A comparison of the samples collected before prostate massage between the BPH and the PC groups did not show any statistically significant differences. When these 2 groups were compared in terms of hepsin levels after prostate massage, these levels were significantly higher in the PC group (p<0.024) (Fig. 5). As was the case with the analysis of AMACR levels, to obtain more detailed data on urinary hepsin levels, the patients were stratified by Gleason score (Fig. 6). Median hepsin levels were 0.00, 2.42 and 3.30 before prostate massage and 2.25, 2.41 and 3.10 after massage in patients with a Gleason score of 5, 6 and 7, respectively, although no statistically significant differences were observed. Patients were also stratified by tumor stage. Median hepsin levels were 0.00, 3.49 and 2.71 before prostate massage and 2.66, 1.14 and 2.67 after prostate massage in patients with pT2a, pT2b and pT2c tumors, respectively. No statistically significant differences were observed (p>0.05) (Fig. 7). An ROC analysis was performed to compare the true positive and false negative rates. At the cutoff point of 2.25 ng/mL for hepsin levels, the true positive and false negative rates were 61% and 25%, respectively (AUC = 0.662; 95% CI, 0.526-0.798) (Fig. 4).
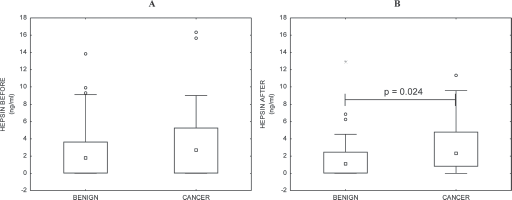
Group comparison of hepsin concentrations in urine before and after prostate massage.
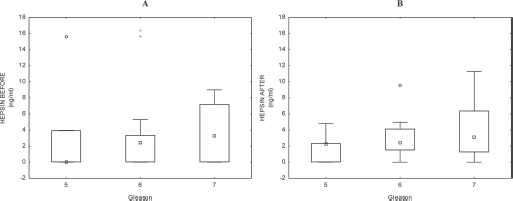
Comparison of hepsin levels in urine collected before and after prostate massage in cancer patients with different Gleason scores.
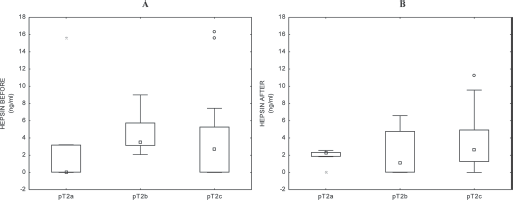
Comparison of hepsin levels in urine collected before after prostate massage in cancer patients with different tumor stages.
Discussion
The aim of the study was to establish whether changes in urinary levels of selected proteins may be used for differentiating between BPH and PC. We decided to compare these 2 conditions because high serum PSA levels are very often observed in patients with BPH, which leads to incorrect initial diagnosis and places the patient at risk of being subjected to more invasive diagnostic procedures. In our study, we utilized urine samples collected from patients diagnosed with BPH and patients diagnosed with PC. We showed that only in urine collected after prostate massage were there significantly higher levels of both AMACR and hepsin in patients with PC. We also showed that in the BPH group, AMACR and hepsin levels were lower in samples collected before prostate massage. Of the 2 proteins, the between-group differences were greater for AMACR. Unfortunately, we did not observe any correlations between AMACR and hepsin levels in the urine collected before and after prostate massage, tumor stage and Gleason score. The comparison of the diagnostic potential showed that AMACR allowed for differentiation between PC and BPH with a true positive rate of 75% and a false positive rate of 26%, and hepsin allowed for differentiation between PC and BPH with a true positive rate of 61% and a false positive rate of 25%. Compared with the results obtained in the analysis of serum PSA levels and evaluation of the usefulness of this parameter for differentiating between PC and BPH, PSA levels managed to achieve this aim with a higher true positive and false negative rates (91% and 39%, respectively). While higher levels of AMACR and hepsin may be seen in the PC group, a better solution is sticking to the current diagnostic methods (i.e., PSA). PSA has the advantage of not requiring prostate massage before the test (prostate massage is indeed contraindicated). This solution is also more comfortable for the patient. In conclusion, AMACR and hepsin are not appropriate single markers for the correct differentiation between BPH and PC. An alternative could be to create a screening test that would include multiple parameters, including AMACR and/or hepsin.
Conclusion
AMACR and hepsin were unable to diagnose PC with better true positive and false negative rates than PSA. Supposedly, an additional procedure combined with other markers should be applied for the reliable diagnosis of cancer stage and further treatment. A combined, fast and noninvasive assay might be of special importance in the screening procedure for elderly men.
Footnotes
Financial support: The project was supported by a National Science Center Research Grant for Young Scientists (Preludium #2012/07/N/NZ7/01139).
Conflict of interest: None declared.