
Abstract
Purpose
Emerging evidence suggests that adiponectin may play a protective role in tumor progression and prognosis. However, available evidence in prostate cancer is conflicting. Therefore, we carried out a meta-analysis to evaluate the role of circulating adiponectin and prostate cancer.
Methods and results
An extensive search was performed on Google, PubMed, Elsevier Science and Springer from the date of the inception of those services to December 2013. Eleven studies with 2,504 patients and 3,565 controls concerning this association were included in our analysis. Standard mean difference (SMD) with 95% confidence intervals (95% CIs) was used to estimate this association. The pooled analysis showed that circulating adiponectin concentrations were lower in patients with prostate cancer than controls, with a pooled SMD of -0.893 μg/mL (95% CI, -1.345 to -0.440, p=0.000). Dose-response relationships between concentrations of adiponectin and risk of prostate cancer were evaluated. We found that decreased concentrations of adiponectin were associated with a significantly greater risk of prostate cancer (p for nonlinearity = 0.043).
Conclusions
The results of our analysis indicated that concentration of adiponectin in cancer patients was significantly lower than in controls. Thus, adiponectin may serve as a potential biomarker for early diagnosis of this disease. We also found that decreased concentration of adiponectin was associated with a significantly greater risk of prostate cancer. However, more studies in future, especially larger, prospective studies, are needed to confirm this association with underlying biological mechanisms.
Introduction
Prostate cancer is one of the most common cancers in men. Prostate cancer causes considerable morbidity and mortality, particularly in North America, the United Kingdom and Australia where obesity is also a substantial health problem (1). Prostate cancer is predominantly a disease of older men, but around 20% of cases occur in men under the age of 65. Recent evidence showed that over 60% of men had histological evidence of prostate cancer by the age of 85 years. However, the etiology of this disease remains largely unknown.
Accumulating evidence suggests that adiposity and high body mass index (BMI) are associated with prostate mortality (2, 3), but the underlying mechanisms are still unclear. Emerging evidence has shown that adipocyte is an important secretory organ which can produce various hormones, cytokines and growth factors, collectively called adipokines. Among these adipokines, adiponectin has gained much more attention because of its potential role in the development and progression of prostate cancer (4–5–6).
Several studies have focused on the correlation of circulating adiponectin and prostate cancer, and found conflicting results regarding any correlation of concentration of adiponectin and prostate cancer. Although some of these studies found that cancer patients had significantly lower adiponectin levels than controls (7–8–9–10–11), other studies did not find any difference in concentrations of adiponectin between patients and controls (12–13–14–15–16), while some even found the opposite (17). Previous data lead to the hypothesis that adiponectin may be a protective factor against prostate cancer. Understanding the association between circulating level of adiponectin and prostate cancer may provide useful information in the development of preventive and therapeutic strategies against prostate cancer. However, no studies have systematically summarized the existing evidence so far. Therefore we carried out this analysis to evaluate the role of adiponectin in prostate cancer, especially the potential link between adiponectin and prostate cancer.
Methods
This meta-analysis was carried out in accordance with preferred reporting items for systematic reviews and meta-analyses.
Search strategy
This meta-analysis was carried out in accordance with the guidelines of the Meta-analysis of Observational Studies in Epidemiology (MOOSE) Group. An extensive search was performed in all major electronic databases from inception to December 2013. The search strategy was created and carried out prior to the study selection process. The search was limited to human studies and was without language restrictions. The search strategy was constructed by using a combination of MESH subject headings and text-words: “adiponectinor APN or Adipor ACRP30 protein or Adipocyte Complement-Related Protein 30-kDa or Adipocyte, C1q and Collagen Domain Containing Protein or Adipose Most Abundant Gene Transcript 1 or apM-1 Protein” and the name of prostate cancer (for example “adiponectin and prostate cancer”). Two reviewers (Q.L. and C.L.) independently conducted a search of Google, PubMed, Elsevier Science and Springer. Finally, we reviewed the references of all relevant articles to identify additional relevant studies. Any disagreement was resolved by discussion with the third investigator (Z.D.).
Inclusion and exclusion criteria
Abstracts, full articles and gray literature (such as symposia proceedings or poster presentations from relevant meetings) that passed the primary screening were retrieved and scrutinized for the presence of all of the following details: (i) all studies were cohort studies or case-control studies, which reported the relation between circulation adiponectin level and prostate cancers; (ii) cancer diagnosis must have been clearly proven; (iii) adiponectin was measured in the blood samples collected prediagnosis or before any treatment postdiagnosis; (iv) if there were multiple publications of the same trial, only the most detailed publication was considered for analysis; and (v) there was enough information about the size of clinical trial or enough information to estimate the mean value and standard deviation of circulating adiponectin. Studies were excluded if they were studies on animals or cell lines, studies of genetic variations in adiponectin-related genes or studies with other cancer control group, or if they were case series, letters, editorials, comments, reviews or abstracts without sufficient details to estimate the mean value and standard deviation, even after contact with relevant authors had been made.
Data collection process and data synthesis
Data were extracted independently by 2 reviewers (Q.L. and C.L.). Each article was scrutinized to determine whether it met the inclusion and exclusion criteria. Data were extracted independently by each reviewer using a standardized data collection form to increase the uniformity of data extraction and to reduce reporting bias. Inconsistencies between reviewers’ data were resolved through discussion until a consensus was reached. The extracted data included several data points, such as country of study, study design, number of cases and controls, blood sample, assay method, assay resource, mean age, mean BMI, summary effects and adjusted factors. Disagreements over values or analysis were resolved by discussion. Adiponectin levels in each study were extracted as means ± SD. One study did not provide the relevant data, although communication with authors had taken place. For studies that provided outcomes in sizes, medians and ranges, the means and standard deviations were calculated based on the method previously described (18).
Assessment of study quality
The quality of reports included was scored using the Newcastle-Ottawa scale (NOS) (19). A star system for the NOS was developed for the assessment. Because there were no established standard criteria, we considered a study awarded 0 to 3, 4 to 6, or 7 to 9 stars, to be low, moderate or high quality, respectively. Two investigators (Q.L. and C.L.) independently rated the selected articles in a blinded fashion, and any inconsistencies were resolved by discussion with the third investigator (Z.D.).
Statistical analysis
The meta-analysis was completed according to the recommendations from the Cochrane Collaboration (20). The effect measures estimated were standard mean difference (SMD) for extraction data and reported, with 95% confidence intervals (95% CIs). The SMD was calculated using the fixed-effect model when heterogeneity was low. We tested for heterogeneity among studies using the I2 test. In the I2 test, a calculation of greater than 50% reflects statistical significance for heterogeneity. If results were heterogeneous (p<0.01), a random-effects model was employed. Publication bias was assessed by Egger's linear regression test, which is reported using funnel plots. Analysis was performed using the statistical software Intercooled Stata version 11.0 for Windows (Stata Corp, College Station, TX, USA).
Results
Literature search
The detailed steps of our study selection are shown in Figure 1. Twenty-eight studies were identified as potentially relevant studies. After scrutinized to determine whether it met the inclusion and exclusion criteria, 1 article was excluded for not giving enough information to calculate the means and standard deviations. Another 9 articles were also excluded because no healthy or benign prostatic obstruction controls were available in their studies. Another 7 studies were excluded for unclear cancer diagnosis or other cancer diagnosis. Finally, 11 studies were selected for further analysis including 4 nested case-control studies and 7 case-control studies. No cross-sectional studies or randomized controlled trials (RCTs) were included, based on our inclusion and exclusion criteria.
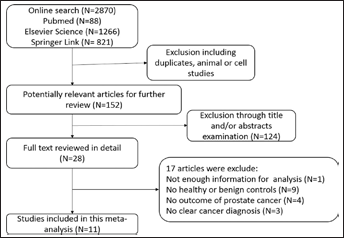
Flow diagram of the study selection process.
Study characteristics
We identified 11 studies (7–8–9–10–11–12–13–14–15–16–17) with 2,504 patients and 3,565 healthy controls or patient controls with benign prostatic obstruction, to evaluate the circulating adiponectin levels in this analysis (Tab. I). Of these articles identified, 5 described studies that found that concentrations of adiponectin in cancer patients were significantly lower than in controls (7–8–9–10–11). The other 5 studies did not find a significant difference in concentration of adiponectin between cancer patients and controls (12–13–14–15–16). A study by Al Khaldi et al even found concentrations of adiponectin in cancer patients were significantly higher than in controls (17). Only 4 studies (10, 12, 14, 15) were carried out in Europe and North America, and the rest (7–8–9, 11, 13, 16, 17) were conducted in other parts of the world. Among the studies included, 4 (10, 12, 14, 15) were s, and the rest were case-control studies. Levels of circulating adiponectin were all detected in blood samples, including plasma samples (7, 10, 14, 15, 17) and serum samples (8, 9, 12, 13, 16). Levels of circulating adiponectin were analyzed by radioimmunoassay from Linco Research in 6 (7–8–9, 13–14–15) of the studies included. Concentrations of adiponectin in 3 studies were detected by ELISA from Linco Research (16, 17) or R&D Systems (10). Only 1 study (11) did not provide enough information about the sample or the method for detection. Controls from 2 studies (7, 8) included healthy people and patients with benign prostatic obstruction, whereas only healthy controls were enrolled in 7 other studies (9, 10, 12, 14–15–16–17). Only patient controls with benign prostatic obstruction were enrolled in the rest (11, 13).
Characteristics Of Included Studies On Adiponectin And Prostate Cancer In This Analysis

BPH = benign prostatic hyperplasia; CC = case-control: ELISA = enzyme-linked immunosorbent assay: NA = not available: NCC = nested case-control: RIA = radioimmunoassay.
I. The low adiponectin levels were associated with an increased risk for breast cancer. II. There was no association with adiponectin and breast cancer risk. III. The high adiponectin levels were associated with an increased risk for breast cancer.
1. age, 2. body mass index, 3. race, 4. family history of prostate cancer, 5. total cholesterol level, 6. triglycerides, 7. diabetes mellitus, 8. liver dysfunction, 9. chronic heart failure, 10. renal failure, 11. smoking status, 12. height, 13. supplementation of antioxidant vitamins and minerals in intervention group, 16. alcohol intake, 17. physical activity, 18. educational level.
The quality assessments of all of the included studies were conducted, and the results are shown in Table I. Four of these studies (8, 11, 13, 16) were of moderate quality, and the rest (7, 9, 10, 12, 14, 15, 17) were of high quality according to the assessment (Tab. I).
Main analysis
A meta-analysis of 11 studies, including a total of 6,069 individuals (3,565 controls and 2,504 patients with prostate cancer), was performed. Significant heterogeneity was observed across these studies (p for heterogeneity <0.001), and thus the random-effects model was applied. Circulating adiponectin concentrations were lower in patients with prostate cancer than in controls, with a pooled SMD of -0.893 μg/mL (95% CI, -1.345 to -0.440, p=0.000), with statistically significant heterogeneity (I2=97.90%, p<0.0001) (Fig. 2). In addition, 3 studies (8, 10, 14) were about the association of concentration of adiponectin and risk of prostate cancer. Dose-response relationships between concentrations of adiponectin and risk of prostate cancer were evaluated (21), and we found that decreased concentrations of adiponectin were associated with a significantly greater risk of prostate cancer (p for nonlinearity = 0.043). For a 5-μg/mL increase in circulating adiponectin, the risk of prostate cancer decreased by 13% (relative risk = 0.87, 95% CI, 0.76 to 0.99).

Forest plots of SMD with 95% CI for studies concerning the concentration of adiponectin in cancer patients compared with healthy control and BPH controls. The horizontal lines represent the 95% CI, the diamonds represent the summary SMD. BPH = benign prostatic hyperplasia; CI = confidence interval; SMD = standard mean difference.
Subgroup analysis
We conducted stratified analyses to evaluate potential sources of heterogeneity according to potential contributing factors including geographic region, study design, blood sample, assay method and source, study size, study quality, adjustment for age and BMI factors. In stratified analysis, the summary SMD of adiponectin levels comparing prostate cancer patients with controls did not differ substantially in the various subgroup analyses according to blood sample, adjustment for age and BMI (Tab. II). Stratified analysis according to control source, geographic region, study design, assay method and source, study size, study quality was also carried out; however, these associations were significantly different in each stratum (Tab. II).
Meta-Analysis Of Circulating Adiponectin Levels And Prostate Cancer By Study Characteristics

BMI = body mass index; BPH = benign prostatic hyperplasia; CC = case-control; CI = confidence interval; ELISA = enzyme-linked immunosorbent assay; NA = not available; NCC = nested case-control; RIA = radioimmunoassay; SMD = standard mean difference.
Meta-regression and sensitivity analysis
Due to the high heterogeneity in the above analysis, we performed meta-regression analysis to investigate the impact of the above study characteristics on the estimate of SMD. In meta-regression analysis, none of the factors geographic region, study design, blood sample, assay method and source, study size, study quality or adjustment for age and BMI factors, were found to be significant contributing factors. A sensitivity analysis was also conducted by removing 1 factor at a time and calculating the pooled SMDs for the remaining studies, and we found that none of the selected studies substantially influenced the pooled result in this analysis (Fig. 3).

The influence of individual studies on the pooled standard mean difference.
Publication bias
Publication bias was evaluated by funnel plot and Egger's test. Funnel plot shapes showed a slightly asymmetrical distribution. Therefore, we conducted further analysis with Begg's and Egger's tests. The results of Begg's test (p=0.127) and Egger's test (p=0.087) suggested that publication bias was not evident in this meta-analysis (Fig. 4).

a) Funnel plot showed a slightly asymmetrical distribution, which raises the possibility of a publication bias; b) Begg's funnel plot; s.e. = standard error; SMD = standard mean difference.
Discussion
Prostate cancer, the third most common cancer in men worldwide, is becoming an increasing important public health problem (1). Although obesity is a well-established risk factor for some types of tumor, its roles in the initiation and prognosis of prostate cancer are still unclear. The relation between obesity and prostate cancer is quite complex and has yielded many inconsistent results. Emerging evidence has shown that obesity is associated with mortality, advanced stage disease and higher grade Gleason score in prostate cancer, but not necessarily related with increased risk of prostate cancer (7, 8, 22). The precise mechanisms for obesity's influence on the progression of prostate cancer have not been defined, but several studies have indicated that the mechanisms may include insulin-related pathways. Additionally, several studies have observed that insulin resistance may alter the risk of prostate cancer through the obesity-sex hormone pathway and non-obesity-related pathways. A study by Hsing and his colleagues also showed that insulin resistance may increase the risk of prostate cancer among men with a low BMI and waist to hip ratio through obesity-independent mechanisms such as inflammation, oxidative stress and apoptosis (23, 24). However, the connection between obesity and prostate cancer must be other than insulin resistance, because the insulin resistance contributes to an increased risk and obesity may be related to tumor progression (7). Therefore, the underlying mechanisms are still opaque, and it remains to explain the association between obesity and initiation and progression of prostate cancer.
Adipokines might represent such an association between prostate and cancer. Although more than 50 types of adipokines have been identified, with diverse functional roles, adiponectin has been most extensively studied (25). We focused here on adiponectin, which is a peptide with 244 amino acids, mainly synthesized exclusively by adipocytes and secreted into plasma. Adiponectin is abundant in human plasma, with concentrations ranging to 3 to 30 μg/mL and accounting for up to 0.05% of total plasma protein (26). In humans, plasma adiponectin concentrations fall with increasing obesity, and this effect is greater in men than in women (27). Reduced adiponectin concentrations correlate with insulin resistance and hyperinsulinemia (28). According to published studies, obesity, inflammation, insulin resistance, metabolic syndrome, cardiovascular disease and cancer are significantly associated with concentrations of adiponectin. Moreover, a recent meta-analysis (29) also indicated that low circulating adiponectin levels are associated with an increased breast cancer risk. It seems that adiponectin may be the link between obesity and cancer.
Recent data have focused on the association between circulating adiponectin and risk for prostate cancer, and circulating levels of adiponectin in prostate cancer patients compared with controls. But inconsistent results were reached. The results of the present meta-analysis suggested that lower adiponectin levels are found in patients with prostate cancer than in controls. Although high heterogeneity was observed in the present analysis, this discrepancy of adiponectin concentration between malignant and controls appeared to show that adiponectin might have the potential to serve as a noninvasive novel biomarker for the early detection of prostate cancer. However, well-designed studies are needed to confirm the biomarker role of adiponectin in prostate cancer. In addition, dose-response relationships between concentration of adiponectin and risk of prostate cancer were analyzed in 3 studies (8, 10, 14). We found that that decreased concentrations of adiponectin were associated with a significantly greater risk of prostate cancer. For a 5-μg/mL increase in circulating adiponectin, the rate of prostate cancer decreased by 13%. However, the underlying mechanisms for how adiponectin reduces the risk of prostate cancer remains unclear.
So far, there are several mechanisms which may be proposed to explain these findings. Adiponectin can induce phosphorylation and activation of the AMPK pathway, which is the regulator of systemic energy balance. Activation of AMPK was reported to inhibit the growth of prostate cancer cell lines by 90% and induce apoptosis (30, 31). Wang et al found that recombinant adiponectin markedly reduced serum-induced phosphorylation of Akt and GSK3β, decreased intracellular accumulation and nuclear translocation of β-catenin which is a central event of activation of the canonical Wnt/β-catenin pathway, and suppressed cyclin D1 expression (32). Therefore it was suggested that the cross-talk between adiponectin and Wnt signaling pathways might represent a critical mechanism underlying the development of obesity-related prostate cancers. Furthermore, adiponectin has been shown to possess antiinflammatory activity, and it can inhibit the production of a number of inflammatory factors involved in promoting mammary tumorigenesis, such as interleukin 6 (IL-6), tumor necrosis factor alpha (TNF-α) and monocyte chemoattractant protein-1 (MCP-1) (33). Moreover, adiponectin also inhibits inflammation by reducing recruitment and activation of mature macrophages, their production of TNF-α, and the activity of Toll-like receptor-4, all of which have been linked to prostate cancer (34). In addition, evidence for why adiponectin is reduced in some cancers is still lacking, but reversal of this reduction may be helpful for improving prognosis.
Our study had several limitations that need to be taken into consideration when interpreting the findings. First, as in any other meta-analysis, residual confounding inherent in the original studies cannot be controlled in the meta-analysis, which may have led to either overestimation or underestimation of risks (35). Nevertheless, our sensitivity analysis excluding studies that did not adjust for age and BMI, 2 important potential confounders, did not materially change the results. However, type 2 diabetes is also an important confounding factor (36, 37), and none of the studies included in this analysis took that into consideration. Second, there was significant heterogeneity observed across these studies, which would reduce the reliability of these results. Although stratified analysis and meta-regression analysis were performed, none of the factors geographic region, study design, blood sample, assay method and source, study size, study quality or adjustment for age and BMI factors were found to be significant contributing factors. Third, the assay applied in the studies included detected the total adiponectin and could not distinguish between the adiponectin isoforms, high- and low-molecular-weight complexes which may have different biological activities. Also, emerging data have shown that posttranslational modifications such as glycosylation at lysine residues located in the collagenous domain are major determinants of the biological activity of adiponectin (38). Therefore, the fact that only the total concentration of adiponectin was measured in the studies included reduces the power to evaluate the association of adiponectin and risk of prostate cancer, and further studies focused on functional part of adiponectin are warranted. In addition, the sensitivity of both Egger's and Begg's tests is generally reduced in a meta-analysis including fewer than 20 studies (39). Therefore, it is difficult to evaluate the influence of publication bias accurately. Finally, these findings were all based on studies with retrospective design, and those studies included in this analysis were mostly of small sample sizes, which would also reduce the statistical power.
Despite these limitations, our study indicates that adiponectin levels in patients with prostate cancer are significantly lower than those in controls, which suggests that adiponectin may be a potential biomarker for early detection of prostate cancer. Moreover, we found that levels of adiponectin were inversely associated with risk of prostate cancer. Further studies, both epidemiological and experimental, are warranted to clarify the association between adiponectin and the development of prostate cancer.