
Abstract
Introduction
The identification of microvessel density (MVD) in patients suffering from different types of cancer has become a hot point as an emerging and promising biomarker. The aim of the present study is to clarify the prognostic relevance of MVD in hepatocellular carcinoma (HCC).
Methods
Relevant articles were screened in PubMed and EMBASE databases. Patients' clinical characteristics, overall survival (OS), disease/recurrence-free survival (DFS/RFS), and MVD levels were extracted for further analysis. The statistical analysis derived from the Kaplan—Meier survival curves was calculated indirectly with the methods developed by Parmar, Williamson, and Tierney. Multivariate Cox hazard regression analysis was used directly in Stata 11.0. The pooled hazard ratio (HR) and 95% confidence interval (CI) were calculated to evaluate the prognostic role of MVD in HCC.
Results
Our online literature search identified 12 articles including a total of 1,138 HCC patients. Meta-analysis of all the included studies considering survival outcomes showed a positive correlation between poor prognosis and higher-MVD levels. The pooled HRs (and 95% CIs) for OS and DFS/RFS were respectively 2.08 [1.77-2.45] and 2.64 [2.12-3.29]. Subgroup analyses considering tumor stage (I-II/III-IV), tumor size (<5 cm/≥5 cm), differentiation (well/poor), or cirrhosis status (≥20%/<20%) were also conducted, and all the above analyses supported the prognostic role of MVD in HCC.
Conclusion
Our meta-analysis showed that the available evidence supports the proposition that MVD has a good predictive role in HCC, especially when the patients have late stage, large size, or poorly differentiated tumors.
Introduction
Hepatocellular carcinoma (HCC) is one of the most prevalent tumor types, with a high incidence especially in Africa, South-East Asia, and China because of the high hepatitis B/C infection rate and the diffuse alcohol consumption (1, 2). Its incidence and mortality rates have both increased in recent years; the global cancer statistics report estimated that 748,300 new liver cancer cases occurred worldwide in 2008 and that, in the same year, 695,900 patients died of cancer, most of whom suffering from HCC (3, 4).
Angiogenesis indicates the formation of new capillaries from the existing vascular network and is essential for tumor development. Folkman firstly clarified the role of angiogenesis in tumor growth and metastasis, that is, the highly vascular nature of the tumor plays an important role in promoting the propensity of cancer cells to grow, spread, and invade neighboring and distant sites (5, 6). HCC is widely known to be characterized by a progressive development (being highly refractory to conventional chemo and radiation therapy), a high recurrence rate, and a poor prognosis, all characteristics that have been attributed to its highly vascular nature (7). Early post-operative recurrence in the liver remnant or distant sites is a common phenomenon after HCC resection (8). Therefore, this disease is still a major challenge, and identification of novel markers to identify individuals at high risk of recurrence is of great concern.
Nowadays, one of the most extensively studied parameters that have been applied for testing angiogenesis in tumor tissue is the presence of microvessels. Microvessel density (MVD), reflecting angiogenesis in tumor areas, may be an important factor for identifying those patients who are at high risk of recurrence or metastasis. MVD can be assessed by immunoreactive anti-pan-endothelial antibodies, such as CD31, CD34, CD105, or Von Willebrand Factor (vWF), with a technique similar to that firstly proposed by Weidner in 1991 (9). In brief, establishing MVD in tumor tissues may provide us with novel insights in clinical prognosis and treatment strategies. Until now, MVD was proven to be an important factor for prognosis and metastasis in many carcinomas such as lung, bladder, and breast cancer (10-11-12). However, the relationship between MVD and the outcome of patients with HCC has not been clearly evaluated. Specifically, the association between MVD in the tumor and survival outcome is highly variable. Most researchers believe that HCC patients with high MVD have a poor prognosis. A few other researchers have different opinions, and hypothesize that HCC patients with low MVD might have a higher fraction of hypoxic tumor cells resulting in a more aggressive tumor cell population, with a greater chance of intra-hepatic metastasis, and bad prognosis (13, 14). In this article, we performed the first literature-based meta-analysis to evaluate the prognostic value of elevated MVD among patients suffering from HCC.
Materials and Methods
Search strategy
The PubMed and EMBASE databases were searched until Jan 14, 2014. We retrieved articles with the combination of the following key words: [hepatoma OR hepatocellular] AND ([cancer OR carcinoma OR tumor OR neoplasm]) AND ([MVD] OR [microvessel density]). We also manually screened the references of the relevant original articles and reviews to supplement our final search.
Study selection and inclusion/exclusion criteria
Studies were considered eligible if they met all of the following inclusion criteria: (i) investigated HCC patients, regardless of the patients' clinical characteristics, such as different stage, differentiation, or metastasis status; (ii) compared the correlation between MVD expression level and one or more of the following survival outcomes: overall survival (OS), disease-free survival (DFS), recurrence-free survival (RFS), etc.; (iii) was written as full paper in English or Chinese. Studies were excluded based on any of the following reasons: (i) review articles, laboratory articles, or letters; (ii) presented duplicate data; (iii) lacked key information to calculate the log hazard ratio (logHR) and standard error (SE).
Two independent reviewers carried out an initial assessment by identifying the eligibility of abstracts from the identified studies. Full articles were retrieved for further assessment if the eligibility was unclear from the sole abstracts. Any disagreements were resolved by discussion or consulting a third reviewer. We carefully examined the names of all authors and the medical centers involved in each publication to avoid including duplicate data.
Data extraction
To avoid including duplicate data, the most integrated study with the longest follow-up time was included if several published studies with the same patients were performed in the same research center, or if the study included patients also described in another study. Conversely, we included both studies if different patients were included in 2 studies of the same research center. Similarly, when a study presented multiple sets of data, such as various detection markers (CD34, endocan, vWF, etc.) or different treatment strategies (resection or liver transplant), we listed all data sets as separate ones.
Articles were independently reviewed by 2 investigators (Xuelei Ma and Yanyan Li) for data extraction. Any discrepancy was resolved by further discussion to reach a common consensus. Multivariate Cox hazard regression analysis was initially included in our analysis and, if not available, the Cox hazard regression analysis or Kaplan—Meier curves of the survival outcomes with log-rank p values were extracted. Additional data were carefully extracted from all eligible publications, using a standardized data collection form including the following items (as we previously defined them): first author, publication year, study size, patient resource, patient's age, gender ratio (females/males), tumor stage, degree of differentiation (well/poor), HBsAg status, cirrhosis status, metastasis status, follow-up period, detection method, tumor size, and other relevant clinical characteristics.
Statistical Methods
The logHR and SE were required for our analysis. Some of the original papers provided both these parameters; however, for those studies that did not state the logHR and SE, we calculated the parameters with the methods developed by Parmar (15), Williamson (16), and Tierney (17). These computable parameters include: (i) multivariate Cox hazard regression analysis data; (ii) univariate Cox hazard regression analysis data with log-rank p value; and (iii) Kaplan—Meier survival curves with log-rank p value. The statistical analyses derived from Kaplan—Meier survival curves with log-rank p values were calculated with the software designed by Matthew Sydes and Jayne Tierney (Medical Research Council Clinical Trials Unit, London, UK). Forrest plots were used to estimate the prognostic role of MVD in HCC. Secondary pooled calculations were performed using RevMan 5.0 (Cochrane collaboration, Oxford, UK).
Since the outcomes under examination were survival or progression in HCC patients, a significant outcome was defined as having a p<0.05. A combined HR>1 frequently indicated a poorer prognosis in the high-MVD cohort. A p<0.10 or I2>50% indicated that heterogeneity in combined HRs existed (18). When homogeneity was good (p≥0.10, I2≤50%), a fixed-effects model was applied to the secondary analysis, otherwise a random-effects model was used. All the abovementioned calculations as well as the evaluation of publication bias, determined using the Begg's funnel plot, were performed in Stata 11.0 (Stata Corporation, College Station, TX).
Results
Eligible studies
The primary literature search yielded 264 articles. After screening their titles and abstracts, 241 studies were excluded because they were laboratory studies (n=192), review articles (n=24), articles on other types of cancer (n=18), or duplicate studies (n=7). The remaining 23 full-text publications were reviewed thoroughly. As a result, 11 articles were further excluded because they did not have enough survival data available for further calculation. Finally, 12 studies (19-20-21-22-23-24-25-26-27-28-29-30) were included in this meta-analysis, all of which were published between 1996 and 2011 (Fig. 1).

Selection of the studies included.
Zeng et al (28) detected MVD in patients who received different treatment strategies (resection or liver transplant). Similarly, 3 other studies (22, 24, 25) detected MVD using different markers (CD34, vWF, endocan, claudin-5 [CL-5]). These data groups estimating the HRs of OS and RFS/DFS were all extracted as separate data sets for further statistical analysis.
The eligible studies encompassed a total of 1,138 patients, with a mean number of 95 patients per study. All the included studies were from Asia: 4 (19, 20, 24, 29) were from Japan and the remaining 8 from China. The main characteristics of the included studies are summarized in Table I.
SUMMARY TABLE OF THE META-ANALYSIS

resection;
liver transplant;
overall survival;
disease free survival;
relapse free survival.
Because the parameters of DFS and RFS were similar, we combined them together as RFS/DFS. Finally, we considered the 12 eligible articles, including 19 data sets, for the analysis of survival outcomes: of these, 7 articles contained 10 data sets estimating the prognostic effect of MVD for OS, and 8 articles included 9 data sets estimating RFS/DFS; all these data were used for our meta-analysis.
Correlation between MVD and survival outcome
Overall survival
The HRs for OS were available in 7 studies for a total number of 716 patients, while the HRs for RFS/DFS were available in 8 studies for a total of 842 patients. We found that the pooled estimated HR for all the studies showed a significantly increased risk of shorter OS in HCC patients with higher MVD expression (HR 2.08, 95% CI 1.77-2.45). The pooled HR for RFS/DFS for all the included studies was 2.64 (95% CI 2.12-3.29), which suggested a significant risk of disease progression in patients with high-MVD levels. Since for both outcomes the heterogeneity test performed among the studies was not significant (I2=44% and I2=0% separately), the fixed-effect model was applied (Fig. 2).

Estimated hazard ratios (HRs): summary for (A) overall survival (OS) in all HCC patients; (B) disease-free survival/recurrence free survival (DFS/RFS) in all HCC patients.
Subgroup analysis
Relevance of MVD after liver transplantation or resection
When we performed the subgroup analysis stratifying the patients by treatment strategy (Tab. II), both subgroups with HCC (the liver transplant and resection subgroups) were characterized by statistically significant differences for RFS/DFS. The studies from Zhang and Zeng (23, 28) analyzed the survival of HCC patients after liver transplantation: the HRs and 95% CIs were 1.15 (0.40-3.26) for OS and 4.40 (1.39-13.94) for RFS/DFS. All the rest of the studies included HCC patients who underwent resection; for these patients the HR and 95% CI for OS were 2.11 (1.79-2.49), and for RFS/DFS were 2.59 (2.07-3.24) (Tab. II).
META-ANALYSIS OF MVD EXPRESSION IN HCC: HAZARD RATIOS AND CONFIDENCE INTERVALS TO PREDICT THE SURVIVAL OUTCOME

overall survival;
recurrence-free survival/disease-free survival;
hazard ratio;
confidence interval.
Relevance of MVD for tumor differentiation
We then modified the analysis regarding the specific differentiation status of HCC. Some of the studies (20-21-22, 24, 27-28-29-30) included more patients with a well-differentiated tumor (≥50%), and the HRs and 95% CIs were 1.95 (1.59-2.38) for OS, and 2.54 (2.02-3.19) for RFS/DFS. Conversely, in other studies (19, 25) that included more patients with a poorly-differentiated tumor (>50%) the HR and 95% CI were 2.51 (1.47-13.27) for OS, and 4.03 (1.36-11.96) for RFS/DFS (Tab. II).
Relevance of MVD for tumor stage
We then further stratified our subgroup analysis by the ratio (≥50% or <50%) of patients with stage III-IV tumors. The studies by Zhang et al (23, 26), including more patients (≥50%) with stage III-IV tumors, reported the prognostic role of MVD in OS (HR, 2.31; 95% CI, 1.20-4.44) and RFS/DFS (HR, 4.40; 95% CI, 1.39-13.94). Additionally, in the studies including fewer patients (<50%) with stage III-IV tumors (29, 30), the pooled analysis of HRs and 95% CIs were 2.01 (1.00-4.01) for OS, and 2.05 (1.29-3.25) for RFS/DFS (Tab. II).
Relevance of MVD for tumor size
We then divided the studies according to the tumor size of HCC patients. In the studies including more patients (≥50%) with a large tumor size (≥5 cm) (23, 26), the pooled HRs and 95% CIs were 2.19 (1.63-2.95) for OS and 2.67 (2.01-3.55) for RFS/DFS. By contrast, in the studies including fewer patients (<50%) with large tumor size (≥5 cm) (29, 30), the pooled HRs and 95% CIs were 1.62 (1.19-2.20) for OS and 2.47 (1.71-3.56) for RFS (Tab. II).
Relevance of MVD for cirrhosis status
In the studies including more patients (≥20%) with HCC-related cirrhosis (23, 27, 30, 31), the pooled HRs and 95% CIs were 1.92 (1.08-3.42) for OS, and 3.01 (1.63-5.56) for RFS/DFS. By contrast, in studies including fewer patients (<20%) with cirrhosis (22, 25, 28), the pooled HRs and 95% CIs for OS and RFS/DFS were 2.26 (1.69-3.03) for OS, and 2.77 (2.06-3.73) for RFS/DFS.
Publication bias
The Begg's funnel plot and test were used to examine the possible publication bias. The results of our meta-analyses regarding the MVD prediction value for OS and DFS/RFS were, respectively, p=0.891 and p=0.221 (Fig. 3).
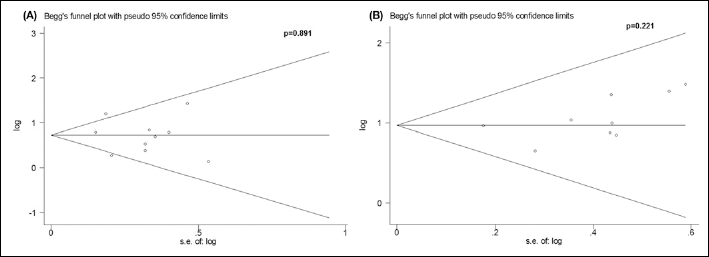
Funnel plots of the publication bias summary for the corresponding meta-analysis shown in Figure 2. Specifically: Funnel plots of the publication bias for the meta-analysis of hazard ratios (HRs) for (A) OS with higher-MVD expression in the tumor tissue; (B) DFS/RFS with higher-MVD expression in the tumor tissue.
Discussion
This is the first detailed and comprehensive meta-analysis of the prognostic role of MVD in HCC patients. By pooling all the studies that compare survival of patients with HCC according to the angiogenic activity of the tumor (as expressed by their MVD level) our meta-analysis showed a significant prognostic effect of the MVD levels detected in tumor samples for OS and RFS/DFS. Patients with elevated tumor MVD showed a significantly higher risk of recurrence and overall decreased survival rates. The pooled results were fairly consistent also when stratifying by tumor stage, degree of differentiation, tumor size, and cirrhosis status. The results of our collective evaluation of the literature on HCC suggested that MVD in HCC had a good predictive value. As a rule of thumb, a risk ratio (RR) >2 was considered as positive for a prognostic biomarker in clinical practice. The combined HRs and 95% CIs for RFS/DFS and OS both met this standard. These results suggest not only that MVD is a promising biomarker to predict survival outcome and evaluate tumor progression, but also that it may be an effective drug target.
In addition, the adverse prognostic effect of MVD detection was confirmed throughout all the subgroup analyses performed. All results of the pooled analysis stratified by degree of differentiation (well/poor) and tumor stage (I-II/III-IV) were above 2; also, we easily found that the group including more patients with poorly-differentiated tumors (well differentiation/poor differentiation <50%) had a better predictive value than the group including more patients with well-differentiated tumors. Similarly, the group including more patients with late stage tumors (III-IV) had a higher predictive value for both OS and RFS/DFS. When classifying the results by tumor size, we found that the group including more patients (≥50%) with large-size tumors (≥5 cm) also had a higher predictive value for both OS and RFS/DFS. All the above results suggest that MVD is a good prognostic factor in HCC patients, and that it plays a better prognostic role in poorly-differentiated, late-stage, and large-size HCCs; moreover, in HCC cases MVD expression is closely related to lymph node status, tumor stage, and tumor size. These results are potentially important for prognostic reasons as well as for treatment purposes. When considering the cirrhotic status of HCC cases, it is important to note that patients with non-cirrhotic HCC often present in advanced stages, with large-size tumors, and have high recurrence rates because they are not participating in screening programs. However, our results suggest a similar prognostic role for MVD in both cirrhotic and non-cirrhotic HCC. Above all, our meta-analysis suggests that MVD in HCC is a good prognosticator regardless of tumor stage, degree of differentiation, tumor size, and cirrhosis status. When we divided the studies by treatment strategies, the HRs for OS or RFS/DFS had a good result in HCC patients who received resection, while the HRs for OS in liver transplant patients were not statistically significant. A possible explanation of the fact that MVD does not relate to survival in transplanted patients could be that, most frequently, metastases occur first in the liver. Thus, while the intrahepatic metastases are removed during liver transplantation, after partial liver resection the remnant liver can harbor clinically undetectable metastases that give rise to recurrences in due time (28).
Angiogenesis is an important mediator of tumor progression. As tumors expand, diffusion distances from the existing vascular supply increase resulting in hypoxia. Because of this, hypoxia-induced angiogenesis has become an attractive target for cancer therapy. MVD is commonly used to indicate the angiogenic activity of tumors (31). Hyperplasia of the microvessel indicates more extended exchange areas between the blood and tissue fluid, which means significantly increased perfusion capability and penetrability, thus indicating that the microvessel distribution is closely related to the blood supply of the tumor (31). At the same time, as tumors expand and determine hypoxia, this latter condition selects a more aggressive phenotype. Because of this, angiogenesis has become an attractive target for cancer therapy. Indeed, various mechanisms are involved in the angiogenic process reflected by MVD, with convergence of these signals allowing transduction and subsequent activation of pathways that promote tumor proliferation, migration, invasion and, ultimately, survival and metastasis (9). According to our meta-analysis, we hypothesize that angiogenesis assessment can be useful in stratifying patients for the use of certain drugs against angiogenesis; on the other hand, angiogenesis assessment is also critical in predicting their response to treatments such as chemotherapy and anti-angiogenic therapy. Therefore, the anti-angiogenic therapy may also be a useful therapeutic modality in preventing recurrence after treatment of HCC. To some extent, this detection tool could also be considered as a much more sensitive way to identify the pre-cancerous lesions.
Since only full-text published studies, and studies for which methodology data were available in full publications were included into this meta-analysis, and since we could not take into account the few studies published in languages other than English or Chinese, this selection might have favored the studies presenting positive results (32). Clearly, the meta-analysis could not account for unpublished studies. We attempted to minimize the publication bias by making our literature search as complete as possible. In our analysis, the Begg's test was used to examine the publication bias. No significant publication biases were found in the results of our meta-analyses for MVD prediction of OS and RFS/DFS in HCC (p=0.891 and p=0.221, respectively).
However, certain limitations are still intrinsic to the statical methods we used for our meta-analysis. Firstly, the multivariate analysis of logHR and SE could only be extracted using a direct method, while the logHR and SE extracted from the survival curves and the p values are univariate analysis; thus, we combined univariate and multivariate analysis together to ensure data integrity. Furthermore, the detection of MVD is made with a qualitative test that requires the interpretation by a pathologist or laboratory technician, which can be highly variable. Direct MVD staining could only be performed on a small tissue sample, which was affected by the possibility of heterogeneity in angiogenesis distribution, a characteristic commonly seen in tumors. As for quality assessment, we did not assign a quality score to the included studies, because there is currently no generally agreed assessment system for prognostic meta-analysis.
In conclusion, our meta-analysis showed the available evidence supporting the proposition that MVD has a fine predictive role in liver cancer patients. It may also be speculated that MVD could perform as a good detecting method in liver cancer. These results were mostly based on data extracted from univariate survival analysis in retrospective trials. In order to become a useful prognostic factor, the present results need to be confirmed by adequately designed prospective studies with an appropriate multivariate analysis that takes into account the classical well-defined prognostic factors for liver cancer.