
Abstract
Platelet activation observed in cancer patients is associated with the release of various cytokines, including P-selectin and CD40 ligand (CD40L). We analyzed the plasma levels of sCD40L in association with adhesion molecules (sP-selectin and sVCAM-1) to check the hypothesis of a possible involvement in cancer progression.
Blood samples were obtained from 59 patients with different stages of colorectal cancer (CRC) and 29 age and gender-matched control subjects. Plasma sCD40L, sP-selectin, and sVCAM-1 concentrations were measured with quantitative sandwich enzyme-linked immunoassay.
All patients with CRC had significantly higher levels of sCD40L (p<0.001), sP-selectin (p<0.02), and sVCAM-1 (p<0.03), as compared to healthy subjects. The level of sCD40L significantly correlated with sP-selectin (p<0.05) in patients with distant metastases to the liver. We also observed a high negative correlation between sP-selectin and platelets count (p<0.02) in patients with lymph node metastasis. The receiver-operator curve for CRC patients indicated that the area under the curve for sCD40L was 0.915, which may indicate its high efficiency as an inflammatory marker.
In our study, the sCD40L correlated with sP-selectin in patients with advanced stage of CRC, which might indicate its possible participation in metastasis formation.
Introduction
The participation of the CD40/CD40 ligand (CD40L) system in inflammation and thrombosis is already relatively well known; however, its involvement in the neoplastic processes is currently a novel aim of research. Inflammation takes part in tumor development and progression (1), and CD40L could be a new link between inflammation and thrombosis (2).
CD40L (or CD154) is a membrane protein present on the surface of numerous immune cells, such as T and B lymphocytes, basophils, NK cells, macrophages, mastocytes, endothelial cells, and blood platelets. It has been estimated that over 95% of plasma soluble CD40L (sCD40L) is derived from active blood platelets (3-4-5). Besides P-selectin, resting platelets contain CD40L in α granules; within a few seconds after platelet activation by the classical agonists (i.e. ADP, collagen, or thrombin) the ligand is expressed on the platelet surface. Then, metalloproteinase activity leads to proteolytic hydrolysis, and CD40L is released into the circulation where it can be identified as sCD40L, its biologically active soluble form (5, 6). Both the ligand and its soluble form can bind the glycoprotein IIb/IIIa, due to the presence of the KGD sequence, and may thus play a role in platelet activation and stimulate further release of CD40L (7-8-9).
The receptor for CD40L is a type-I transmembrane protein belonging to the TNF-CD40 family (10), which is present on the surface of numerous cells, including blood platelets, monocytes, macrophages, and endothelial cells (5, 11). Although CD40L and its receptor individually do not perform any definite biological function, their interaction results in the generation of an intracellular signal and in the production of surface and secretory molecules that have an ultimate effect on both humoral and cellular immune responses (12). The CD40/CD40L system increases the expression of adhesion molecules such as VCAM-1 (13) that recruit monocytes and lymphocytes, thus causing their accumulation in the inner vascular membrane (14, 15); it also increases the secretion of metalloproteinases (MMPs), cytokines, and chemokines, such as IL-8, IL-10, IL-12, MCP-1, MIP-1α, and RANTES (16). These cytokines can modulate the function of T lymphocytes in antitumor responses, i.e. immune suppression (17).
Some authors indicate that CD40L can mediate the induction of tumor cell apoptosis and the stimulation of the inflammatory response, thus leading to their elimination (18, 19). The CD40/CD40L system is suggested to play roles also in the stimulation of endothelial cells, in the formation of tubules, as well as in angiogenesis promotion, by inducing VEGF production from endothelial cells and by activating platelets (20, 21), thus facilitating tumor growth (19, 22). Understanding the mechanisms involving the CD40/CD40L pathway and CD40L in neoplastic disease might contribute to exploiting this interaction in antineoplastic therapy.
Since there is only little evidence concerning the involvement of CD40L derived from active platelets in cancer spread, as well as its role as disease biomarker, we decided to explore the subject. Therefore, the major aim of the study was to clinically assess whether the plasma level of sCD40L depends on the stage of colorectal cancer (CRC). We analyzed the plasma sCD40L levels in association with either sP-selectin, which is used as a marker of in vivo platelet activation, or sVCAM-1, used as marker of endothelial cell activation, to check the hypothesis of its involvement in the formation of neoplastic metastases and cancer progression. Finally, we checked if sCD40L could be a useful biomarker of inflammation in neoplastic disease.
Materials and Methods
Patients
Fifty-nine patients with CRC surgically treated at the second Department of General and Gastroenterological Surgery, University Hospital in Bialystok (Poland), were recruited to participate into the study. The patients were enrolled between November 2011 and April 2013.
The diagnosis of CRC was based on clinical symptoms and imaging investigations (radiology and TK), as well as endoscopy (colonoscopy). Patients who had received chemotherapy, immunotherapy, or radiotherapy before the study were excluded. Patients had no symptoms of inflammation or infection, and none of them received antiplatelet drugs, antinflammatory drugs, corticosteroids, or anticoagulants within the 2 weeks preceding the study.
Patients (34 males and 25 females; mean age, 66 years) were histologically diagnosed with adenocarcinoma (51/59) and adenocarcinoma mucinosum (8/59). Low malignancy grade cancer (G2) was observed in 52 CRC patients, and high malignancy grade cancer (G3) in 7. Malignancy grade was verified based on histopathological assessment of cancer lesions excised during surgery. Tumors were localized in the colon in 16 patients (27.1%), the sigmoid colon in 21 patients (35.5%), and the rectum in 22 patients (37.2%).
CRC patients were divided into 3 groups according to the tumor, node, metastasis classification: group A1, 27 patients with stage I/II (T1-4N0M0); group A2, 19 patients with stage III with lymph node metastasis (TXN+M0); group A3, 13 patients with stage IV with distant metastasis to the liver (TxNxM+). The control group consisted of 29 healthy subjects (16 males and 13 females; mean age, 64 years) without any systemic disease or infection at the time of enrollment.
The study was approved by the ethical committee of the Medical University of Bialystok, and was performed according to the guidelines for good clinical practice. Patients enrolled in the study gave written informed consent for participation.
Material
Venous blood (2.7 mL) was collected, without stasis, into S-Monovette (Sarstedt) test tubes containing 3.2% sodium citrate (1:9, v:v), during the morning of the same day in which surgery was planned. To minimize in vitro platelet activation during blood drawing, samples were collected without stasis, and the first 2 mL of blood were discarded. Within 30 minutes after collection blood was centrifuged twice according to the manufacturer's instructions: first at 1.500 g for 15 minutes, and then at 10.000 g for 10 minutes. Then, platelet poor plasma (PPP) samples were stored at -70°C until analysis. Before the assays, the samples were thawed slowly and centrifuged again (Vortex).
Methods
Plasma sCD40L, sP-selectin, and sVCAM-1 concentrations were measured with quantitative sandwich enzyme immunoassay using the following kits according to the manufacturer's instructions: Human CD40 Ligand, Human sP-selectin Immunoassay, and Quantikine Human sVCAM-1 (all from R&D Systems, Abingdon, UK). According to the R&D Systems the minimum detectable dose (MDD) of CD40L was in the range 2.1-10.1 pg/mL (mean MDD was 4.2 pg/mL), and the range was between non-detectable (ND) and 139 pg/mL. The MDD of sP-selectin was typically less than 0.5 ng/mL and its range in citrate plasma was observed to be 20-44 ng/mL. The mean MDD of sVCAM-1 was 0.6 ng/mL and its range was 341-897 ng/mL.
All samples were assayed in duplicate and there were no statistically significant differences between the two measurements of the same sample.
Platelets count
Blood samples (2 mL) were collected into test tubes containing EDTA-K2, and platelets count was automatically determined in the same sample on the hematological analyzer ADVIA 2120i (Siemens). The platelets count in healthy subjects range from 150x103/μL to 350×103/μL.
Statistical Analysis
We used the results for statistical analysis, and the mean and standard deviation were calculated. The Shapiro-Wilk test was used for normally distributed data, the Student's t test was used to compare the 2 groups, and the univariante analysis of variance with Bonferroni post-hoc test was used to compare the data between multiple groups. The Mann-Whitney test and Kruskal-Wallis test with Dunn's analysis of contrasts were applied for features inconsistent with this distribution. Correlation coefficients were calculated depending on the Pearson's or Spearman's distribution. The ROC curves were also analyzed using the MedCalc statistical software.
The differences were considered statistically significant for p<0.05. The calculations were performed using the statistical packages SPSS and NCSS.
Results
The demographic and clinical data of CRC patients are presented in Table I. Among the patients we included, men were more than women (57.6% vs 42.4%).
DEMOGRAPHIC AND CLINICAL DATA COLORECTAL CANCER PATIENTS
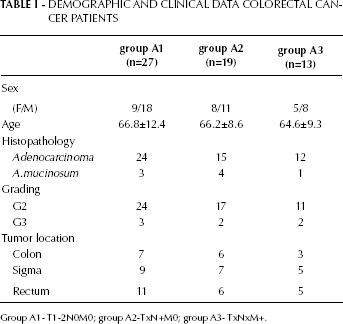
Group A1- T1-2N0M0; group A2-TxN+M0; group A3- TxNxM+.
The mean plasma levels of sCD40L (p<0.001), sP-selectin (p<0.02), and sVCAM-1 (p<0.03) were significantly higher in CRC patients than healthy subjects. Similarly, the platelets count was higher in CRC patients than in controls, but not statistically significant (Tab. II).
PLASMA LEVELS OF sCD40L, sP-SELECTIN AND sVCAM-1 AND PLT COUNT IN COLORECTAL CANCER PATIENTS (CRC) AND IN CONTROL GROUP
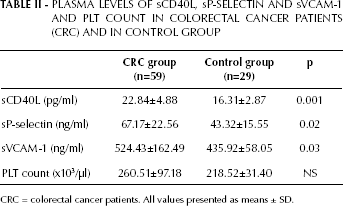
CRC = colorectal cancer patients. All values presented as means ± SD.
Subgroup analysis by tumor stage of sCD40L showed that in all groups the sCD40L levels were significantly higher than the controls (p<0.001) (Tab. III). The highest concentration of CD40L was observed in patients with metastases to the lymph nodes (group A2), but there was no statistically significant correlation between the level of CD40L and cancer stage.
SUBGROUP STATISTICAL ANALYSIS OF PLASMA sCD40L, sP-SELECTIN and sVCAM-1 LEVELS AND PLT COUNT IN CRC PATIENTS
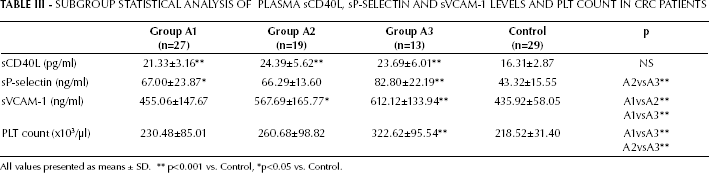
All values presented as means ± SD.
p<0.001 vs. Control,
p<0.05 vs. Control.
The sP-selectin level was significantly higher in patients with stage I/II (group A1) (p<0.05) and stage IV (group A3) (p<0.001) than healthy controls (Tab. III). However, statistically significant differences were observed only between the level of sP-selectin in patients with lymph node involvement (group A2) and patients with distant metastases to the liver (group A3) (p<0.005) (Tab. III).
The platelets count increased along with the degree of cancer progression, and statistically significant differences were observed between patients with stage I/II and stage IV CRC (p<0.008), and between stage III and stage IV CRC (p<0.04) (Tab. III).
The sVCAM-1 level showed a trend toward increased values from stage I/II to stage IV CRC, and statistically significant differences were found between group A1, A2 (p<0.0.004), and A3 (p<0.009). In groups A2 and A3, the plasma levels of sVCAM-1 were statistically significantly different from those of the control group (Tab. III). The levels of both sP-selectin and sVCAM-1 were the highest in group A3.
The analysis of sCD40L concentration and other study parameters showed the presence of a highly positive correlation with sP-selectin (r=0.632, p<0.05) in patients with metastases to the liver (group A3). Moreover we observed a highly negative correlation between sP-selectin and platelets count in group 2 (patients with lymph-node metastases, r=-0.704, p<0.02). Conversely, there were no correlations between CD40L levels and gender, age, histological diagnosis, malignancy grade, and sVCAM-1 in CRC patients.
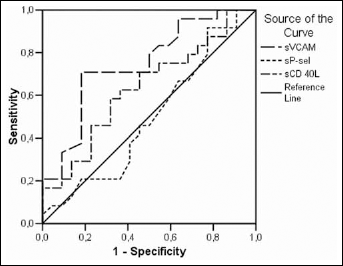
The differences between the diagnostic sensitivities and specificities of sCD40L, sP-selectin, and sVCAM-1 were investigated by ROC curve analysis (Figs. 1 and 2). For sCD40L the discrimination between CRC patients and healthy subjects showed an area under the ROC curve of 0.915 (p<0.03), which indicates its excellent diagnostic power (Fig. 1). The discrimination between CRC patients with and without metastases showed the greatest area under the ROC curve for sVCAM-1 (0.746; p<0.004) (Fig. 2).
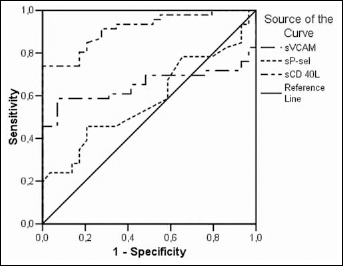
ROC curves for sCD40L (AUC=0.915, SE=0.031, p<0.000), sP-selectin (AUC=0.582, SE=0.066), and sVCAM-1 (AUC=0.650, SE=0.065) distinguishing between CRC patients and healthy subjects.
ROC curves for sVCAM-1 (AUC=0.746, SE=0.073, p<0.004), sCD40L (AUC=0.633, SE=0.82), and sP-selectin (AUC=0.495, SE=0.087) distinguishing between CRC patients with or without metastases.
Discussion
Recent reports indicated that CD40L expression on active blood platelets defines de novo the role of platelets not only as cells involved in the coagulation process but also as immunologically competent cells (23). Data from the literature have proven a dual role of CD40L in neoplastic disease. This role within the immune system in cancer patients is difficult to interpret and, at the same time, therapeutically interesting.
Our results showed a significantly higher level of sCD40L in CRC patients than their correspondent age and gender-matched controls. As reported by Huang et al (17), age is not a factor that can influence CD40L levels in healthy donors. We confirmed this observation, and what is more, we also failed to find an effect of age in CRC patients. Some authors suggested that high levels of sCD40L could be a result of platelet activation in vitro caused by pre-analytical factors (24). We centrifuged blood twice, at a temperature of 2°C-8°C, and for the examination we used platelet-poor plasma, which should overall prevent platelet activation in vitro. In our study, the highest sCD40L levels were found in patients with metastases to local lymph nodes and with distant metastases to the liver, although the differences were not statistically significant when compared to metastasis-free CRC patients. Therefore, it is hard to explain whether elevated sCD40L levels can have a direct effect on disease progression. It is possible to conclude that the secretion of sCD40L occurs in CRC patients irrespective of the degree of tumor progression, inducing, perhaps, a stimulation of the immune system. According to Huang et al (17), high levels of sCD40L may inhibit the antitumor immune response. The authors demonstrated that the significantly increased synthesis of suppressive cytokines (such as IL-6 and IL-10) after administration of sCD40L leads to a significant reduction in T cell proliferation and, indirectly, to an increased level of CD40L. This may be one of the factors that enhance the suppressive function of sCD40L (17).
Increased levels of sCD40L have been observed in inflammatory diseases of the colon (5), in diabetes (25), atherosclerosis (13), cardiovascular diseases (26), as well as in neoplasms including colon (18), lung (27), stomach (28), breast (17), and prostate cancer (17), and hematological malignancies (29, 30). Jablonska et al (30) reported significantly lower levels of sCD40L in B-CLL patients than controls, and they suggested that this may be caused by an excess of CD40-leukemia cells that interfere with the T-cell response and determines an acquired CD40L-deficiency syndrome. Patients with B-CLL have immune defects similar to those observed in patients with X-linked hyper-IgM syndrome (HIGM). While CLL-cells express on their surface variable amounts of functional CD40L, the CD4+ T-cells from CLL patients fail to express CD40L upon ligation of CD3. Furthermore, increased sCD40L levels after treatment can be related with an increased number of activated T-helper cells (30). On the other hand, Tsirakis et al (29) found increased concentrations of sCD40L in patients with multiple myeloma before treatment and decreased serum sCD40L levels after cancer therapy. In this case, the high levels of sCD40L may be determined by the increased number of T cells, which characterize multiple myeloma but decrease after successful treatment (29).
According to other authors, in patients with solid cancer CD40L is more likely derived by activated platelets than T cells (17), the latter being characteristic of hematological malignancies (29). Roselli et al (27) found the highest sCD40L levels in most advanced stages of lung cancer, in patients with distant metastases. In turn, Li et al (28), examining the expression of CD40L in gastric cancer patients, found a correlation between the ligand and the presence of metastases, thus indicating its involvement in the formation of new metastatic foci and tumor progression.
Blood platelets are a major component in cancer development and progression during all stages of the metastatic cascade. The main platelet activation marker, sP-selectin mediates cancer cells' interactions with platelets and endothelial cells during hematogenous metastasis. There is substantial evidence of the increased platelet activation in vivo and elevated platelet count in patients with various cancer types. This was confirmed by our current report as well as our previous studies on CRC patients (31). In the present study, the mean level of sP-selectin was statistically significantly higher in patients than in healthy subjects. The highest plasma level of sP-selectin was observed in patients with the most advanced cancer stages, with distant metastases to the liver. It is noteworthy that, at the same time, in patients with metastases to the liver we observed a strong, positive, significant correlation between circulating sCD40L levels and sP-selectin (r=0.63, p<0.05), which may indirectly confirm the hypothesis that the ligand is of platelet origin and that platelets, together with the molecules expressed on their surface, are actively involved in cancer spread. This fact may also have an unfavorable impact, since the elevated platelet count observed in more advanced CRC patients, together with the increased secretion of sCD40L, leads, as we know, to the expression of adhesion molecules, generation of TF, and release of proinflammatory cytokines; these factors could contribute to the activation of the coagulation in these patients. Similar hypotheses have been reported by other authors: Roselli et al (27) showed correlations between both the sCD40L and sP-selectin and activation markers of coagulation (F1+2 and TATc). Their findings indicate an enhanced pro-coagulation activity associated with platelet activation, release of sCD40L, and its possible interaction with the receptor present on the surface of tumor-associated macrophages and lung cancer cells (27, 32, 33).
CD40L binds to its receptor CD40 that is expressed on endothelial cells, thus leading to effective immune response, e.g. induces the expression of adhesion molecules (VCAM-1) and secretion of proinflammatory cytokines. These interactions are well documented also in the formation of atherothrombosis (9, 16); however, much less known is the involvement of platelet CD40L in cancer cell spread and formation of metastases. In a previous study, we observed a significant association between sVCAM-1 levels and cancer progression (34). Moreover, we reported a correlation between the levels of the adhesion molecules sVCAM-1 and sICAM-1 in all groups of CRC patients, which could indicate the stimulation of endothelial cells and the possible participation of these molecules in CRC progression (34). In the current study, which is in part a continuation of the previous one conducted on a larger group of patients, we used sVCAM-1 as a marker of endothelial cells. We found a highly statistically significant increase in the level of sVCAM-1 in CRC patients as compared to controls; especially, this difference was considerable among the groups of patients with metastases to lymph nodes and liver compared with CRC patients with non-metastatic tumors limited to the bowel wall. Although in the current study we did not find statistically significant correlations between CD40L and sVCAM-1, our findings may indirectly indicate the involvement of active endothelial cells in the adhesion and extravasation of cancer cells, which are the key stages of metastasis formation beyond the vascular lumen.
The evaluation of the ROC curve is an important criterion for neoplastic markers as it illustrates the link between diagnostic sensitivity and specificity. The area under the curve indicates the clinical significance of the parameters evaluated. To the best of our knowledge, we are the first to determine the diagnostic specificity and sensitivity of CD40L in CRC patients. The diagnostic usefulness of the examined parameters in CRC patients was compared with that of healthy subjects. Among the assessed parameters, the greatest area under the curve was that of CD40L (0.915), meaning that sCD40L has the highest ability to discriminate cancer patients from healthy controls and is, therefore, a highly useful marker of CRC. For further diagnosis, the ROC curve was used to distinguish between patients with and without metastasis. In this latter case, the greatest area under the ROC curve was that of sVCAM-1 (0.746). A limitation of our study was the small number of patients included, implicating that further research on larger groups of patients is still required.
In conclusion, we observed that sCD40L levels correlated with those of sP-selectin in patients with advanced stage CRC, an observation that might indicate its likely participation in metastasis formation and its association with platelet activation. Our study indicates that sCD40L could be taken into consideration as a biomarker of inflammation, as it is released in cancer patients irrespective of the degree of cancer progression.