
Abstract
For patients with breast cancer, obtaining tissue samples from liver lesion becomes more and more important for both differential diagnosis and subsequent treatment. However, the procedure is not considered as mandatory routine and is not frequently performed. We here reported about a patient with breast cancer history and a solitary liver metastasis that was clinically diagnosed by both magnetic resonance imaging (MRI) and position emission tomography - computed tomography (PET-CT). However, pathologic diagnosis after partial hepatectomy (between sections VII and VIII) revealed multifocal granulomas. The case further addresses the importance of core needle biopsy, or surgical biopsy, for obtainment of a histological diagnosis, especially in the presence of a solitary lesion, even when the lesion has a typical medical imaging supporting metastasis, and uptake of radioactive 18F-fluorodeoxyglucose (18F-FDG) by PET-CT.
Introduction
Breast cancer is the most common malignant cancer in women worldwide (1), and is a life-threatening disease. About 10%-15% of patients have an aggressive form of breast cancer and suffer distant recurrence within 3 years (2). The most common sites of metastasis are bone, lung, and liver. The percentage of liver metastasis at autopsy is approximately 60% (3). Liver metastasis accounts for about 12%–15% of the initial sites of recurrence, according to either self-examination or follow-up examinations (4). Accurate diagnosis of liver metastasis at an early stage is crucial and helps the clinical management of the disease. Several imaging techniques, such as computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) scan, are useful for the detection of hepatic metastases. However, the most accurate and final diagnosis depends on histologic materials obtained from liver biopsy or surgery.
We here reported the case of a 44-year old woman with breast cancer history, in whom a solitary liver nodule was identified and then diagnosed as liver metastasis of breast cancer by both MRI and PET-CT. However, after partial hepatectomy (between sections VII and VIII) the pathologic diagnosis was of multifocal granulomas. We also discussed the clinical guidelines focusing on this issue.
Case Report
A 44-year old woman was diagnosed with invasive ductal carcinoma (IDC) of her left breast on December 20th, 2011, and immediately underwent modified radical mastectomy. The tumor was 3.5 cm in size and 5 of 22 lymph nodes were involved. The pathological data was reviewed in our hospital and IDC with grade 3 was diagnosed. Immunohistochemical examination showed that tumor cells were positive for estrogen receptor (ER) and negative for progestrone receptor (PR). The Ki-67 proliferative index was 30%. The human epidermal growth factor receptor-2 (HER2) gene showed amplification by fluorescence in situ hybridization (FISH). The patient received 3 cycles of FEC regimen (5-Fu, epirubicin, and cyclophosphamide), and 3 cycles of docetaxel, radiotherapy, and trastuzumab. Since July 2012, after chemotherapy, the patient has been treated with tamoxifen and goserelin.
The patient was followed up every 3 months, and the ultrasonography performed on August 22th, 2012 showed irregular fatty infiltration of the liver and a hypoechoic lesion in the right lobe. Abdominal MRI also revealed a slight hyperintense lesion with an irregular shape on T2-weighted imaging. Treatment continued on planned schedule as no evidence of disease progression was found. However, the MRI taken in October 2012 showed a 1.3-cm solitary nodule in the right lobe of the liver. The lesion revealed homogeneous hyperintensity on T2-weighted imaging and rim enhancement after contrast administration, with an irregular margin (Fig. 1A). The PET-CT scan revealed an uptake of radioactive 18F-fluorodeoxyglucose (18F-FDG) in the same nodule (Fig. 1B). All the examinations strongly indicated a solitary hepatic metastasis. Meanwhile, the patient had a slightly elevated carcinoembryonic antigen (CEA) level of 6.67 ng/mL (normal reference range being 0.00–5.20 ng/mL), which was higher than previously documented. However, liver function tests were normal. Altogether, the patient was clinically diagnosed with liver metastasis of breast cancer.
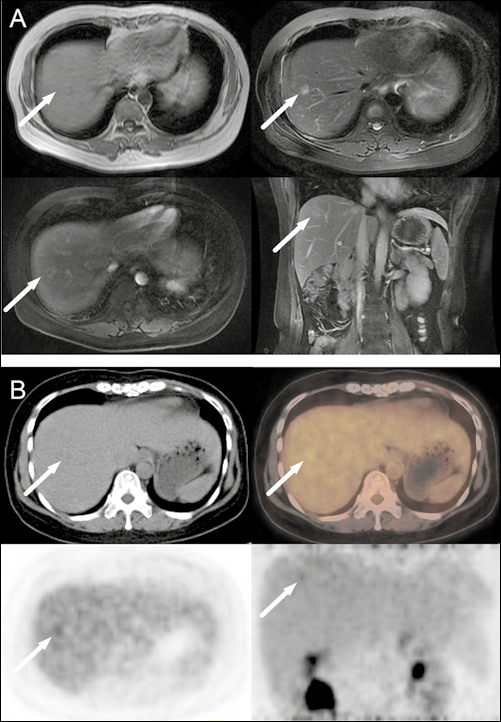
The final medical diagnosis by imaging was determined to be breast cancer hepatic metastasis.
The patient underwent partial hepatectomy (between sections VII and VIII) on November 22th, 2012. During the operation, the intraoperative ultrasound identified the liver nodule, which still suggested liver metastasis of breast cancer. Surprisingly, the histological examination of the resected sample revealed multifocal granulomas with central necrosis, peripheral eosinophils’ infiltration, and multinuclear giant cells’ reaction (Fig. 2A). CD68 immunohistochemical staining was positive (Fig. 2B) and acid-fast staining was negative (Fig. 2C). There was no evidence of cancer metastasis. No granuloma-related medical history, such as infection (tuberculosis, ect.), surgery, trauma, exposure to chemical substances, or drugs was found. Therefore, the patient continued the planned treatments consisting of trastuzumab, tamoxifen, and goserelin. At the moment the patient is under periodic follow-up and no recurrence has been diagnosed up to date.
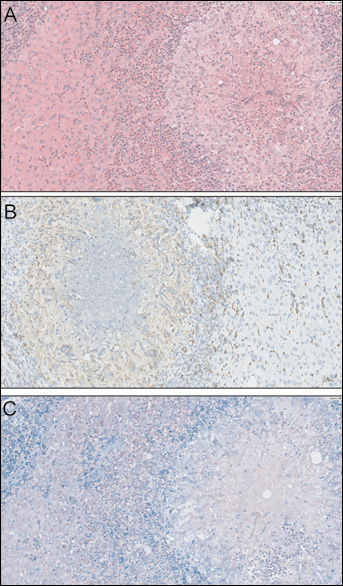
Pathological findings supported a diagnosis of non-specific granuloma.
Discussion
The clinical manifestations and elevated serum tumor markers (5) should draw the physician's attention, and a further examination should be performed in order to possibly identify a metastatic lesion. However, not all instrumental examinations are 100% accurate. The diagnostic sensitivities of MRI on a per-lesion and per-patient basis are 90.7% and 83.7%, respectively, while its accuracy for liver nodules of less than 1.5 cm is 91.1% (6). For PET-CT the sensitivity and specificity for the detection of distant metastases in breast cancer are, respectively, 97.4% and 91.2% (7). It has been reported that some abnormal findings in the liver may lead to misdiagnosis on medical imaging (e.g. fatty liver, which can be caused by tamoxifen treatment) (8).
A granulomatous reaction can be induced by various infective agents and foreign bodies, such as suture material, sponges used during surgery, and fragments of wood or glass introduced during a trauma, but also occupational exposure to chemicals and drugs use. Granulomas can present neoplasm-like imaging, which cannot be easily differentiated from liver matastasis by ultrasound and MRI (9, 10). Here we reported a case of a granuloma that was misdiagnosed as liver metastasis by PET-CT, in the absence of any evidence of possible causative agents of granuloma.
MR findings in granuloma are usually non-specific (9, 10). The lesion in our patient was slightly hypointense on T1-weighted images, and homogeneously hyperintense on T2-weighted images. Even more challenging, the liver lesion was rim-enhanced after contrast administration. Poyanli et al (9) reported of a foreign-body granuloma in the liver with peripheral enhancement that was indistinguishable from liver metastasis of colorectal cancer in ultrasound and MRI studies. Ferrozzi et al (11) even reported of a granuloma case in kidney that contained fat and calcifications and was indistinguishable from renal cell carcinoma. PET-CT findings in granuloma are also non-specific. Bajin et al (12) reported a false-positive FDG uptake of a Teflon granuloma in the larynx.
Therefore, the final and most accurate diagnosis is dependent on histological materials obtained from biopsy or surgery, not only because it helps to confirm or exclude an advanced disease, but also allows individualizing the therapy, which relies on molecular subtyping of the metastatic disease rather than the primary one (13, 14). The American Society of Clinical Oncology (ASCO) Breast Cancer Guidelines suggested that a biopsy of metastases should be considered when it was safe and easy to perform, since possible discordance between primary tumor and liver metastases in receptor status might impact the treatment choice (15). The 2009 National Comprehensive Cancer Network (NCCN) Breast Cancer Guidelines included a suggestion for a biopsy of first relapse site in order to determine ER and PR status (16). The European Society of Medical Oncology (ESMO) Breast Cancer Clinical Practice Guidelines recommended physicians to obtain histopathological confirmation, especially in case of a solitary metastatic lesion, while surgery might be considered for limited metastatic presentations (17). However, the procedure is not considered as a mandatory routine and is not frequently performed for liver metastases of breast cancer.
This unusual clinical case indicates that clinicians should think twice before making a diagnosis of metastasis only according to the medical imaging results, especially when the solitary metastatic nodule in the liver of a breast cancer patient is the only distant recurrence site. Granuloma may cause diagnostic challenges since it has neoplasm-like imaging by both MRI and PET-CT, thus providing additional reasons to perform a biopsy or a hepatectomy.
Footnotes
Acknowledgements
We would like to thank the pathologist Deming He for providing us with pathological sections, and the radiologist Rui Liu for medical imaging advice.