
Abstract
Abstract
Introduction
Prostate cancer (PC) is the second most common cancer in men (1). Radical prostatectomy (RP) is considered the first line of treatment for PC patients. Nevertheless, one-third of treated patients shows local or distant relapse even 5 years after surgical intervention, generally preceded by an increase in serum prostate-specific antigen (PSA). In fact, despite PSA being a non-specific tumor marker (for the reasons indicated above), after a RP with curative intent this serum value acquires the role of main trigger of PC relapse (2). In particular, since the whole prostate tissue is removed during a successful RP, detection of serum PSA using standard immunoassays is considered indicative of residual prostatic tissue, presumably representing locoregional or systemic cancer.
Since PSA could play a role during the monitoring of PC patients after RP, it is important to underscore that some PSA kinetics, such as PSA doubling time (PSAdt) and PSA velocity (PSAve) could play a role in the management of patients and in their prognostic stratification. These parameters are commonly obtained from two absolute consecutive PSA values. PSAve is determined by linear regression of the PSA values over time and is associated with the overall aggressiveness of the tumor during the staging (3) and the restaging of the disease (4). Currently, there are various methods for calculating PSAve and PSAdt that have only small differences in the predictive value of the PSA derivative values obtained (5).
On the other hand, in patients with an increasing serum PSA level after RP it is important to differentiate between local relapse and distant metastases in order to choose the best therapeutic option that is associated with favorable outcome (e.g. salvage radiation therapy in case of local relapse) (6).
The ideal whole-body imaging modality should detect, in the same session, the presence of local relapse and/or distant metastases. Since PC has a malignant biological behavior with a low-grade rate of glucose metabolism (7, 8), positron emission tomography (PET)/computed tomography (CT) with 18F-FDG (an analogue of glucose, considered the most useful radiopharmaceutical for the diagnosis of malignant tumors) is not routinely employed for this disease.
In the last decade, the use of choline (labeled with 18F or 11C) has been proposed to assess the extension and the localization of the disease during biochemical relapse of PC. Choline is a component of phosphatidylcholine, an important element of cell membranes. It is already known that the biosynthesis of the cell membrane is very fast in PC and that the upregulation of choline kinase activity, particularly increased in PC cells, induces a higher uptake of choline (7). Therefore, 11C-choline and 18F-choline can characterize the biosynthesis of the cell membrane in tumor tissues. However, 11C-choline is characterized by a short half-life of only 20 minutes that may determine some logistic problems in those PET centers lacking a cyclotron. For these reasons, other PET centers prefer the use of 18F-choline, which has an extended availability due to its longer half-life of 109.8 minutes.
Many authors support the usefulness of PET/CT with choline in the restaging of PC (especially in patients with high PSA serum levels), because it represents a single step, whole-body, non-invasive examination that allows disease localization (9, 10). Furthermore, it has been shown that PET/CT with choline (labeled with 18F or 11C) can detect more metastatic lymph nodes or bony metastatic lesions than 18F-FDG in PC patients (11, 12). With regard to conventional imaging techniques, other diagnostic modalities, such as bone scan and magnetic resonance (MR), have a limited role because they rarely detect the site of relapse and are not useful until the PSA value is higher than 5 ng/mL (13, 14); similarly, contrast-enhanced CT seems generally not sufficiently sensitive (15).
Materials and Methods
We performed a PubMed research to find studies on the feasibility of PET/CT with 18F or 11C-choline and its diagnostic performance on patients with biochemical relapse of PC after RP. The bibliographic research was performed with the following keywords “prostate cancer”, “biochemical relapse”, “choline”, “PET”, “PET/CT”, “restaging”.
Furthermore, the following limits were used: species (human), article type (original articles), and language (English). The following items were searched in each of the examined studies: number of examined patients, kind of nuclide used for labeling choline (18F or 11C), mean PSA trigger used to enroll the patients, PET/CT detection rate, proposed PSAdt and PSAve cutoffs associated with a better sensitivity.
The references reported by the selected articles and reviews were also evaluated to find additional information that could meet the inclusion criteria. A particular emphasis was attributed to the relationship between PSA values and PSA kinetics in patients at the time of the scan, in order to assess the feasibility of these clinical parameters in relation to the detection rate of the choline PET/CT.
Results
PSA
In many examined studies the results of PET/CT with choline were related to the PSA values, as indicator of relapse of pathology in patients with PC after RP.
In one of the first studies published on this topic, Cimitan et al examined 100 patients with biochemical relapse after therapy by means of PET/CT with 18F-choline. They concluded that choline PET/CT is not likely to have a significant impact on the care of PC patients with biochemical recurrence until PSA increases above 4 ng/mL (16). The abovementioned study also included patients previously submitted to radiotherapy with curative intent or hormonal therapy.
Other studies, performed on more homogeneous populations, have described well the good diagnostic performance of the choline PET/CT technique, especially when referring to patients treated only with surgical intervention. In a population of 41 patients examined for biochemical relapse of PC after RP, Rinnab et al found a good sensitivity (75%), especially in those patients with PSA ≥1.5 ng/mL at the time of examination (17). Later, Husarik et al demonstrated, in a population of 68 patients with the same characteristics, that recurrent disease can be reliably localized in patients with PSA levels of >2 ng/mL (18). In a population with biochemical relapse (PSA ≥0.2 ng/mL) after RP, Scattoni et al showed that PET/CT resulted positive in 21/85 patients: in 90% of these positive scans (19/21) histologic examination confirmed the presence of nodal metastases of PC (19). The authors concluded that, since PSA is correlated with the volume of the prostatic tumor, it is probably necessary for a patient to present a certain tumor volume or PSA level to display a positive imaging finding. In particular, since the enrolled population presented a low mean PSA level (1.98 ng/mL), the authors suggested that patients with a low PSA are more difficult to investigate. For the same reason, the cited study by Scattoni et al was one of the first demonstrating a relatively low sensitivity (64%), attributable to the inability of PET/CT to detect microscopic foci of metastatic PC in lesions smaller than 1 cm in diameter (19).
In patients with biochemical relapse after radical treatment for PC, Pelosi et al found that the PET/CT scan detected disease relapse in 42.9% of the cases (24/56). Also, in this paper the sensitivity was closely related to serum PSA levels, showing values of 20%, 44%, and 81.8% respectively in the groups of patients with PSA <1 ng/mL, 1-5 ng/mL, and >5 ng/mL (9).
On the other hand, Krause et al (20) were the first authors that performed a large study aiming at investigating a PSA cutoff value able to differentiate patients that could actually benefit from the PET/CT with choline. The authors evaluated 63 patients with biochemical relapse (mean PSA=5.9 ng/mL) with 11C-choline PET/CT. They found a significant correlation between the detection rate of the examination and the PSA levels: in particular, the detection rates were 36%, 43%, 62%, and 73% respectively in patients with PSA <1 ng/mL, 1-2 ng/mL, 2-3 ng/mL, and >3 ng/mL. They also concluded that the examination could help not only in the diagnosis of the disease but also in the clinical management (especially with regard to the localization of the relapse), and, therefore, the patients' outcome.
Furthermore, Giovacchini et al confirmed all results of the cited studies. In particular, they evaluated a large population of 358 patients (with mean PSA levels of 3.7 ng/mL), previously submitted to RP o radiotherapy with curative intent. In their study, PET/CT with 11C-choline showed a percentage of positive findings directly correlated to the patients' PSA values. In particular, the PET/CT-positive patients were: 19% of patients with a PSA 0.2-1 ng/mL, 46% of those with a PSA 1-3 ng/mL, and 82% of those with a PSA >3 ng/mL. Moreover, the authors found that the PSA of patients with bone metastases was significantly higher than that of patients with positive PET/CT scan but without bone involvement.
Conversely, in a recent paper by Schillaci et al the results of PET with choline were compared with those of CT with contrast agents performed in the same examination session. In their study, PET alone was positive in 31/49 patients (63.3%); on the other hand, while the CT scan was negative in 14 out of these 31 PET-positive cases, CT was able to diagnose bone metastases in 2 patients with negative PET scan. To the best of our knowledge, the last paper cited was the only one able to compare PET/CT scans to full-dose contrast-enhanced CT, and showed better results, in terms of sensitivity, for PET/CT (15). Furthermore, in the abovementioned paper, the authors confirmed a good relationship between the patients' absolute PSA serum levels and the PET/CT detection rate. In particular, they found a significant difference in PSA values between patients with a positive PET/CT scan (with a mean PSA of 5.35 ng/mL) and those with negative PET/CT scan (with a mean PSA of 1.63 ng/mL). Moreover, PET/CT was positive only in the following percentages: 20% of patients with a PSA <1 ng/mL, 55.6% of patients with a PSA of 1-2 ng/mL, 80% of patients with a PSA of 2-4 ng/mL, and 86.7% of patients with PSA >4 ng/mL.
All the data examined from the literature seem to confirm the significant accordance between the high levels of serum PSA and the PET/CT detection rate. The cited results are similar both in case of lymph node localizations and bone metastases. Actually, further studies are needed to assess the detection rate of local relapse for the pathology of the prostatic fossa in relation to very low PSA values in the examined patients. A recent study by Panebianco et al compared the diagnostic performance of 18F-choline versus MR at 3-Tesla scanner and reported a higher sensitivity of MR in detecting local relapse of PC, in particular in patients with low PSA values (0.2-2 ng/mL) (21).
PSA Kinetics
In the last years, clinicians developed several parameters to assess PSA kinetics. The most important are PSAdt and PSAve. The PSAdt is defined as the time needed for the PSA level to double on an exponential growth pattern, while the PSAve is the linear progression of PSA during time. Several studies have demonstrated the prognostic role of these parameters in patients treated for PC (4, 22).
The hypothesis that PSA kinetics can express the overall aggressiveness of the tumor over time better than PSA was formulated by Carter et al (23): the authors showed that PSA kinetics are more sensitive than PSA in distinguishing patients with benign disease of the prostate from patients with PC. Furthermore, it has been reported that a short PSAdt is related to poor clinical outcome of PC patients treated with radiotherapy (24): in fact, PSAdt can be used for a better stratification of patients in order to choose the best therapeutic approach. Other studies demonstrated that PSAdt in patients treated with RP can play a role as predictor of distant disease (25).
Therefore, similarly to PSA density, the initial role of PSA kinetics was to assess the risk of metastases in patients during staging of PC (8). Subsequently, these parameters were used to monitor the response to therapy and the risk of relapse in patients already treated with curative intent for PC (RP or radiotherapy).
In 2010 Giovacchini et al published one of the first papers aimed at comparing the detection rate of choline PET/CT with PSA kinetics. In a per-patient analysis they calculated the PSAdt using 3 or more PSA measurements spaced by at least 3 months, each with a minimum increase of 0.20 ng/mL (26). The 11C-choline was positive in 75/170 patients (44%). The study not only confirmed the role of PSA as a trigger of relapse of the disease, since patients with a positive scan had significantly higher PSA levels (p<0.05), but also showed for the first time the role of PSAdt for the same group of patients (p<0.05). Furthermore, PSAdt was highly predictive of a true positive scan. In particular, a significantly higher risk of positive PET/CT was found for the intervals of PSAdt <3 months (26/170; 15.3%) and for PSAdt between 3 and 6 months (46/170; 27.1 %), but not for the intervals between 6 and 9 months, >9 months, or >12 and 15 months. The authors also investigated the relationship between PSAdt and pathological choline uptake in the prostatic fossa, lymph node localizations, or skeleton. PSAdt was significantly longer in patients with supposed local recurrence than in patients with presumed bony metastases. In synthesis, in this study the percentage of patients with positive PET/CT was 81% for PSAdt <3 months, compared with lower risk of secondary localizations in the group of patients with PSAdt between 3 and 6 months, and PSAdt >9 months (26). The authors concluded that the probability of a positive PET/CT increases as PSAdt decreases.
These data were also confirmed by Castellucci et al (27) in a retrospective study that enrolled 190 patients previously treated with RP during biochemical relapse. The role of PSA as a trigger of a positive scan (especially using a cutoff value of 2.43 ng/mL) was confirmed. Furthermore, the authors examined the role of PSAdt and added the PSAve in a selected group of patients; in particular, 19/34 (56%) patients who were PET/CT-positive had a PSAdt less than or equal to 3.4 months while the detection rates of PET/CT were 12%, 34%, 42%, and 70% respectively in patients with PSAve of <1 ng/mL/year, 1-2 ng/mL/year, 2-5 ng/mL/year, and >5 ng/mL/year. The optimal cutoff point of PSAve (using ROC analysis) was 1.1 ng/mL/year (54% of patients with positive PET/CT and PSAve greater than or equal to 1.1 ng/mL/year).
All the cited studies were developed in patients with moderately high PSA values. An interesting paper by Castellucci et al (28) examined 102 patients previously treated with RP that showed a mild increase of PSA serum levels (<1.5 ng/mL). Globally, PET/CT was positive in 29/102 patients (only 28%): the main feature of this study was that only PSAdt was found as a significant and independent predictive factor for relapse of pathology in multivariate analysis. Also, in this paper the ideal cutoff value of PSAdt was similar to other previous reports, with a threshold of <7.2 months, which gave a sensitivity of 93%.
In 2012, also Breeuwsma et al analyzing a population of 64 patients with previous RP and increased PSA serum levels, found no significant differences between PSA and PET/CT results, but observed that the patients with positive PET/CT had higher PSAve (>3.09 ng/mL) and shorter PSAdt (<4.8 months). Disease-specific survival was also significantly higher in the group with negative PET/CT (p<0.05). The latter is probably the main finding of this paper, because it was the first to correlate PSA kinetics not only with the results of PET/CT but also with the disease-free survival. These authors also confirmed their results in a larger population of 185 patients with increased PSA (>0.2 ng/mL) after RP (29).
Finally, the previously cited study by Schillaci et al (15) also examined the role of PSA kinetics in the management of PC patients, indicating a global meaningful diagnostic performance of PET/CT in patients with PSA higher than 2 ng/mL. When using a cutoff value of PSAdt of <6 months, PET/CT was positive in 84% of patients, whereas when using a PSAve cutoff value of >2 ng/mL/year PET/CT was positive in 86% of patients. Therefore, the authors concluded that, especially in patients with an absolute PSA value higher than 2 ng/mL, a PSAve cutoff >2 ng/mL/year better correlates with the overall aggressiveness of the tumor and with the possibility to have a positive choline PET/CT scan.
Discussion
When biochemical relapse of PC is diagnosed by means of detectable PSA serum levels, the various conventional diagnostic modalities (such as MR, CT, and bone scan) are normally employed to assess the localization and extension of the disease. According to the European Association of Urology, this diagnostic procedure is not recommended until PSA does not exceed the threshold of 20 ng/mL (30). Considering that the advent of choline-PET/CT (labeled with 11C or 18F) has changed the diagnostic management of PC patients (also those with absolute PSA values lower than 20 ng/mL), it is mandatory to assess the optimal timing to perform this examination in PC patients with biochemical relapse; this is to avoid originating a large number of non-useful scans and false expectations in both clinicians and patients, especially considering the relatively high cost of this technique. On the other hand, it is important to underline the high detection rate of choline-PET/CT compared with conventional imaging and 18F-FDG PET/CT (6, 12-15).
It is well proved that there is a significant correlation between the increase of PSA serum levels and the results of PET/CT scan. From the first studies on this topic, we observed that the threshold suggested by the various authors to perform a PET/CT with choline was progressively reduced during time. In particular, in 2006 Cimitan et al proposed a cutoff value of 4 ng/mL (probably due to the presence of patients previously treated with radiotherapy in the whole examined population) (16), while Pelosi et al in 2008 proposed a threshold of 5 ng/mL (9). After these, the majority of more recent studies agreed in assessing the optimal threshold to perform a PET/CT with choline when the absolute PSA serum levels exceed 2 ng/mL (15, 17-19, 27, 28). Generally, all the authors agree about the difficulty to diagnose PC relapse when using a cutoff value lower than this threshold (26, 29, 31), with unclear or debatable results of the scans.
Furthermore, considering the intrinsic property of the radiopharmaceutical, we can also state that the uptake of choline is not specific to PC cells. In fact, the uptake of the tracer can occur in some benign or malignant conditions other than PC. It is already known that detection of 11C or 18F-labeled choline uptake can occur in various conditions such as brain lesions, lymphomas, inflammation, and malignant tumors, as well as in benign lesions with high synthesis of cell membrane, such as thymoma, sarcoidosis, and parathyroid adenoma (7, 32-39). Also for these reasons it is important to underline the role of PSA, together with an adequate collection of anamnestic data and an accurate knowledge of the “in vivo” biodistribution of the labeled choline, for the correct interpretation of PET/CT images in PC patients.
Regarding the PSA kinetics, all the previously cited papers published over time found an overall concordance between PSA kinetics and PET/CT results, since PSAdt and PSAve better express the aggressiveness of the disease during time with a dynamic model. The various cutoff values proposed for PSAdt and PSAve could play a role in the management of PC patients, due the intrinsic high importance in terms of patients' morbidity and mortality (2, 22). The lack of a routine use of these values in clinical practice and in relation to diagnostic imaging is difficult to explain, especially considering the relative easiness in calculating these parameters.
It is also important to consider that, according to the literature, the positive detection rate of choline PET/CT imaging depends on the plasma PSA levels and PSA kinetics (8, 15, 26-29, 31). In fact, PSA kinetics are the expression of prostatic tissue growth; therefore, the best imaging modality associated with these parameters should be the PET/CT with choline, considering that it is a technique that conjugates both functional and anatomic imaging.
The main limitation of the abovementioned data is that the majority of examined papers are developed on a selected population with increased PSA after RP. For example, the lack of similar data on groups of patients treated with radiotherapy does not allow reaching the same conclusions for this group of patients. In particular, considering that in patients treated with radiotherapy there is a “physiological” amount of measurable serum PSA, there is an implicit difficulty to determine a threshold of PSA that could be potentially useful in selecting patients undergoing PET/CT with choline.
Furthermore, the added clinical value of PSAdt and PSAve cannot be used in patients submitted to antiandrogen therapy, since this kind of therapy could affect the evolution of PSA during time and, moreover, could invalidate the quality of the PET/CT scan, causing a large series of false negative exams.
Finally, since the usefulness of choline PET/CT in detecting distant lymph node and/or bone metastases is well known, future studies are needed not only to assess its definitive role in detecting local recurrence of PC in the prostatic fossa, especially in those patients with very low absolute PSA values (lower than 1.5 ng/mL) (28), but also to assess the potentiality of PSA kinetics in this particular population, considering that the diagnostic performance of this technique in the field is still not so clear (21). However, regarding these last suggestions, Mamede et al recently found a good significance of PSAdt and ongoing hormonal therapy in a population of patients with low PSA serum levels (<0.5 ng/mL) after RP. In particular, they confirmed that PSAdt is a statistically significant predictor of a positive choline PET/CT also in this selected population (40).
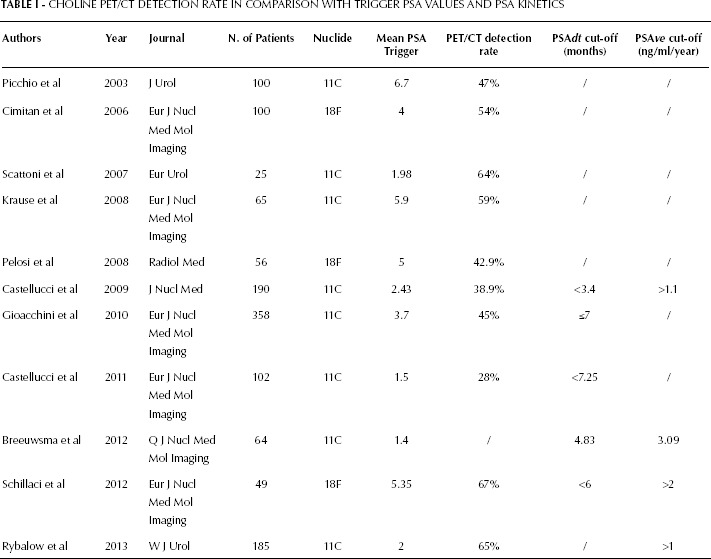
In conclusion, according to the examined papers, we can suggest that the optimal timing to perform the examination in selected patients is when the PSA trigger is higher than 2 ng/mL (Fig. 1), in agreement with the PSA cutoff value mostly used in some relevant papers on this topic (Tab. I). Since the authors agree on the utility of the PSA kinetics, but unique and unequivocal cutoff values are still not available, we can suggest that a PSAve higher than 1 ng/mL and a PSAdt shorter than 6 months could improve the diagnosis and the efficacy of the examination, because it seems to better detect those patients with a potential positive PET/CT scan, even when very low PSA serum levels (<2 ng/mL) are recorded. This clinical behavior could improve the overall diagnostic accuracy of choline PET/CT and reduce the number of inappropriate scans.
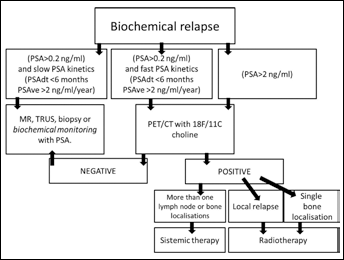
Diagnostic flowchart in prospate cancer patients with biochemical disease relapse.
CHOLINE PET/CT DETECTION RATE IN COMPARISON WITH TRIGGER PSA VALUES AND PSA KINETICS
Furthermore, the availability of PET/CT data could select patients with single secondary localizations that could truly benefit from a conservative focused radiotherapy, thus reducing the possibility of systemic therapy, such as antiandrogenic therapy, over time (Fig. 1).