
Abstract
Introduction
Carcinoembryonic antigen (CEA) is a commonly used tumor marker, and its value in colon cancer is well established. However it is overexpressed in many different tumors. Here we report a case of colorectal cancer with high postoperative CEA levels that were associated with medullary thyroid carcinoma.
Case
A 60-year old man was operated for colon cancer. Postoperative CEA level was 107.6 ng/mL, while preoperative CEA level was unknown. For the detection of distant metastasis or local recurrence, we performed 18-flouro deoxyglycose (FDG) positron emission tomography (PET) and computed tomography (CT). We observed an increased FDG accumulation in the right lobe of the thyroid. The patient had cystic and non-metabolic lesions in the liver, and started a treatment with FOLFOX regimen. After 3 months of chemotherapy CEA was still as high as 146 ng/mL. There was no pathologic FDG uptake other than the thyroid nodule in PET-CT. Fine needle aspiration of the thyroid nodule revealed a follicular neoplasia. The patient underwent total thyroidectomy and histopathology revealed a medullary thyroid carcinoma. Postoperative CEA levels then lowered to normal ranges.
Conclusion
The case we here report was a stage III colorectal cancer with high CEA levels. Our focus on searching a residual/metastatic disease made us blind to other possible explanations; in fact, none of us noticed the thyroid nodule. This case reminds us not to forget that high CEA levels can be associated with conditions other than colon cancer, such as thyroid medullary carcinoma.
Introduction
Carcinoembryonic antigen (CEA) is a complex serum glycoprotein and functions as an intercellular adhesion molecule (1). It is a common cell product that is elevated in serum of patients affected by several types of cancers, including colon, breast, lung, gastric, pancreatic, biliary cancers and cancers of the female reproductive gland (2). An increase in CEA is also reported in patients with medullary thyroid carcinoma (3). Additionally, a variety of non-malignant conditions, including cirrhosis, cholelitiasis, obstructive jaundice, cholangitis, liver abscess, emphysema, bronchitis, gastric ulcer, diverticulitis, diabetes, and collagen vascular disease are also characterized by increased CEA levels (4).
The clinical significance of CEA in colorectal cancer is well established. An elevated preoperative CEA level is associated with advanced cancer stage and poor survival. Failure of CEA to return to normal levels can be a sign of inadequate resection (5). It has been observed that some patients continue to have high postoperative serum CEA levels after curative resection, and this was significantly associated with postoperative relapse (6). The ASCO guidelines recommend postoperative serum CEA testing every 3 months in patients with stage II or III colon cancer for at least 3 years after diagnosis. However, if the patient is a candidate for surgery or systemic therapy (7), a normal CEA cannot exclude recurrence.
Here we report a case of colorectal cancer with high postoperative CEA levels that were associated with medullary thyroid carcinoma.
Case
A 60-year old man was operated for colon cancer. Pathologic stage was T3 N2. After surgical resection the patient was admitted at our clinic for adjuvant treatment. The preoperative CEA level was unknown while the postoperative level was 107.6 ng/mL. Computed tomography (CT) of chest and abdomen showed cystic lesions in the liver. For the detection of distant metastasis or local recurrence 18-flouro deoxyglycose (FDG) positron emission tomography (PET) and CT were performed. We found an increased FDG accumulation in the right lobe of the thyroid. Liver lesions were cystic and non-metabolic. The patient started a treatment with FOLFOX regimen and serial monitoring of CEA was planned. After 3 months of chemotherapy CEA was still as high as 146 ng/mL. Integrated PET and CT (PET/CT) scan showed a thyroid nodule of 2.4 cm in the right thyroid lobe with maximum standard uptake value of 8 (SUVmax). Fine needle aspiration of the thyroid nodule revealed follicular neoplasia. Preoperative calcitonin was 3,752 pg/mL. The patient underwent total thyroidectomy and histopathology revealed a medullary thyroid carcinoma. Postoperative CEA levels returned to normal ranges (see Fig. 1 for CEA levels and Fig. 2 for calcitonin levels before and after thyroidectomy, and at the time of colon cancer recurrence).
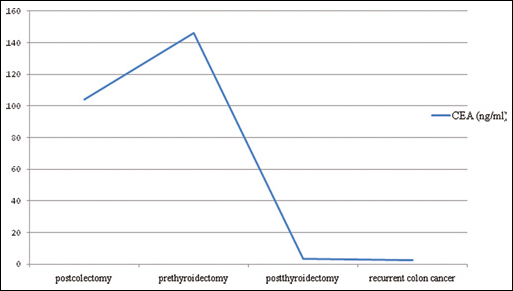
Varying CEA levels of the patient.
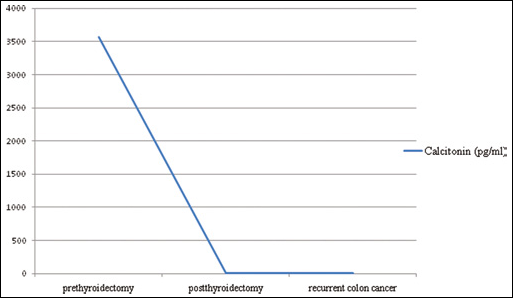
Calcitonin levels of the patient.
Discussion
CEA is a tumor marker commonly associated with colorectal cancer. Elevated preoperative CEA levels are associated with advanced cancer stage and the incidence of recurrence and survival (5, 8). Postoperative CEA levels ≥5 ng/mL are significantly correlated with more advanced stage and postoperative relapse (6). Patients with high postoperative CEA levels should be evaluated for residual disease and/or distant metastasis.
In the last years, functional imaging using PET/CT has been increasingly used in colorectal cancer patients with elevated CEA levels. Mittal et al reported that with PET/CT imaging the detection rate of recurrence increases up to 71%. In all patients with a CEA level of more than 50 ng/mL FDG-PET/CT detected the recurrent disease (9). Incidental focal thyroid uptake can be seen in 1%-4% of patients undergoing PET/CT for other reasons. The risk of malignancy for incidental thyroid lesions on PET/CT is reported to range between 14% and 50% (10).
Medullary thyroid carcinoma is a rare malignancy arising from parafollicular C cells of the thyroid gland. Serum calcitonin is a specific and highly sensitive marker for medullary thyroid carcinoma (11, 12). CEA is also secreted from the tumor, and CEA levels may provide useful information for risk stratification. In patients with preoperative serum CEA levels >30 ng/mL achievement of surgical remission is hard (13). FDG-PET/CT is valuable for the detection of residual, recurrent, or metastatic medullary thyroid carcinoma with a sensitivity of 78%, especially in patients with high calcitonin levels (14).
Of note, the case we report here was a stage III colorectal cancer with high CEA levels. Our focus on searching a residual/metastatic disease made us blind to other possible explanations; in fact, none of us noticed the thyroid nodule. The persistence of high CEA levels and the presence of the nodule with high FDG accumulation in the second PET-CT were indicative of the thyroid malignancy. This case reminds us the importance to being open to all possible explanations, and not to forget that high CEA levels can be associated with conditions other than colon cancer, such as thyroid medullary carcinoma.