
Abstract
Background
Aims
Methods
Results
Conclusions
Introduction
Studies of hepatocellular carcinoma (HCC) patients aim to identify phenotypic subsets for rational treatment choices and prognosis. Most HCCs arise in a chronically diseased liver. Tumor size, as well as liver damage, is considered among the most important prognostic factors (1-2-3-4). Whether inflammatory processes only predispose to HCC or also influence HCC biology is still unclear. Thrombocytopenia, an HCC risk factor was reported to be a cirrhosis surrogate marker (5-6-7), and has been associated with smaller size HCCs (8, 9). Conversely, thrombocytosis has been described in many cancers (10, 11) and larger HCCs (12, 13). In the current report, we analyzed a large database of HCC patients in whom both baseline characteristics and survival were known. Our analysis confirms the association between increased platelets count and larger tumor size. Additionally, alpha-fetoprotein (AFP) and gamma-glutamyl transpeptidase (GGTP) levels increased with tumor size, whereas AFP and platelets count did not relate to survival.
Methods
Data collection. We retrospectively analyzed prospectively-collected data from the Italian Liver Cancer (ITA.LI.CA) study group database: we included 3,027 HCC patients recruited until 2008 in 11 Italian centers (14). A total of 2,773 newly diagnosed HCC patients had complete data of baseline parameters including: radiology of maximum tumor diameter (MTD), number of tumor nodules, and presence of portal vein thrombosis (PVT); demographics (gender, age, alcohol history, hepatitis B or C); blood counts (hemoglobin, white cells, platelets, prothrombin time); blood AFP and routine liver function tests (total bilirubin, AST, ALKP, GGTP, albumin). The ITA.LI.CA database management conforms to the Italian legislation on privacy, and this study conforms to the ethical guidelines of the Declaration of Helsinki. Approval for the study on de-identified patients was obtained by the institutional review board of the participating centers.
Statistical methodology. Means and standard deviations (M±SD) for continuous variables, and relative frequency for categorical variables were used as indices of centrality and dispersion of the distributions.
To test for associations between groups we used the chi-square test for categorical variables, and the Kruskal-Wallis rank test and Wilcoxon rank-sum test (Mann-Whitney test) for continuous variables.
The Z-test for proportions was used for comparison between 2 categorical variables.
For the identification of MTD terciles, since the distribution was not normal, the total dataset was first transformed into natural logarithm scale and then used to identify the relative terciles, with which we performed statistical evaluations. Histograms of the platelet counts were examined in relation to size-terciles of MTD. The Pearson's correlation was calculated for selected tumor parameters in the total cohort.
For the AFP scatter plots and platelet dichotomization analyses, we used the median value of the specific parameter for the total cohort.
A multinomial logistic regression model was applied to evaluate the association of MTD terciles with selected factors (e.g. blood parameters, PVT and number of nodules). In the same way, 3 different multinomial logistic regression models were undertaken (by total cohort, absence and presence of PVT) to evaluate the association between the combination of MTD terciles and the number of nodules based on platelets count (cutoff 125 ×109/L) and AFP levels (cutoff 30 ng/dL), which were all included in these 3 models.
MTD terciles, alone or combined with the variable “number of nodules”, were defined as nominal measures and were considered as unique outcomes within each model.
In the multiple multinomial logistic regression models we used as the reference category the MTD (MTD ≤2.4 cm, I tercile) and the number of nodules (1-2-3), as appropriate.
The Cox proportional-hazards model, corrected for gender, age, and history of alcohol consumption, was used to evaluate the predictive factors associated with overall survival.
Both multiple multinomial logistic regression and Cox proportional-hazards final models were applied with the backward stepwise method and the variables that showed associations with a p<0.10 were left in the models. Those factors associated with outcome (p<0.05) were maintained in the final models.
All models were adjusted for gender, age, and history of alcohol consumption. Results are presented as relative risk ratios (RRR), and as coefficient with relative 95% confidence interval (CI).
The relative risk ratio can be obtained by exponentiating the regression coefficients, which represent the relative risk ratios for a one-unit variation of the predictor variable.
When testing the hypothesis of significant association, a two-tailed p value <0.05 was considered statistically significant. All statistical computations used the STATA v. 10.0 statistical software (StataCorp, College Station, TX, USA).
Results
Tumor Size Terciles
Patients' data were sorted according to the MTD and then trichotomized, thus resulting in 3 tumor size terciles. The tercile analysis in relation to platelet counts (Fig. 1) shows that platelet counts were significantly different when the III MTD tercile was compared to terciles I or II (p<0.0001), with larger size tumors correlating to higher platelet counts (Tab. I). The mean values of the biochemical parameters and the tumor parameters associated with each tercile are shown in Table I. Patients in the III tercile with largest tumors had a significantly higher percentage of PVT, tumor multifocality, and the highest AFP values, together with the highest GGTP and ALKP values, likely indicating the worsening cirrhosis or liver damage determined by the tumor. The mean survival time at 1, 2, and 3 years of diagnosis was shorter for tercile III patients compared with tercile II patients. For the total cohort the median values for platelet counts were 105 x 109/L, for GGTP were 51 IU/mL, for total bilirubin were 1.22 mg/dL, and for AFP were 33 ng/dL.
MAXIMUM TUMOR SIZE TERCILES
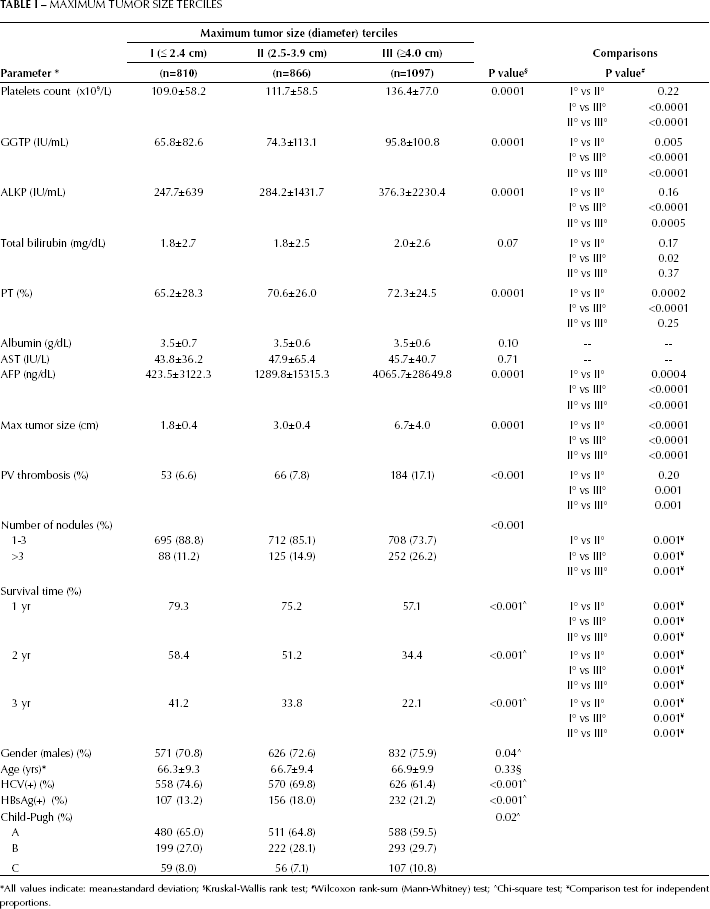
All values indicate: mean±standard deviation;
Kruskal-Wallis rank test;
Wilcoxon rank-sum (Mann-Whitney) test;
Chi-square test;
Comparison test for independent proportions.
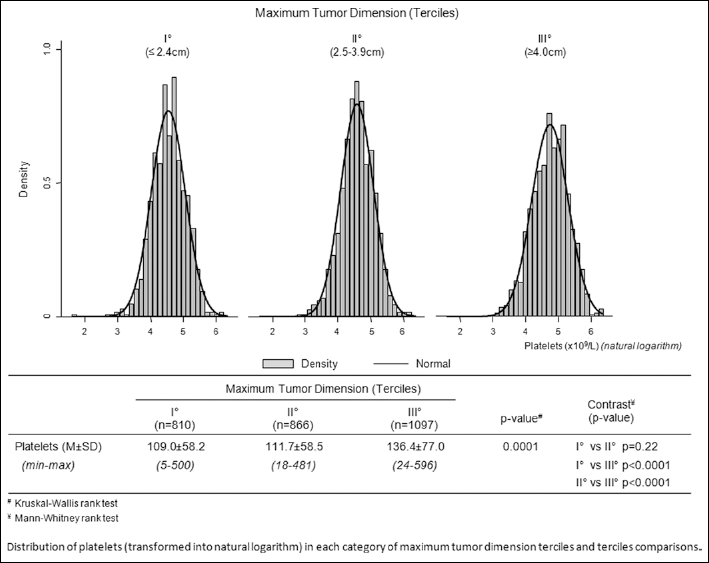
Distribution of platelets in each category of tumor size terciles and tercile comparisons.
Factors relating to tumor size
MTD and blood parameters in the total cohort. Table IIA shows the results of our final multinomial (polytomous) logistic regression model of MTD terciles on predictive factors, where the significant factors were blood platelet counts, GGTP, and AFP levels, as well as PVT and tumor multifocality, for tercile III compared with tercile I patients (the reference category). Furthermore, a multiple multinomial logistic regression model including the combination of MTD terciles and the 2 categories of the variable “number of nodules” (where MTD<2.4cm [I tercile] and number of nodules [1-3] were used as reference category, Tab. IIB) showed a statistically significant correlation for platelet counts and AFP, when MTD >2.4 cm and whether or not the tumor numbers were multifocal. The RRR was higher in PVT+ patients than in PVT− patients. Given these findings and those reported in Tab. I, we depicted the scatter plots for MTD as a function of platelet counts, GGTP, bilirubin, and AFP levels (Fig. 2). We found that the correlation coefficients were significant for platelet counts and GGTP levels (p<0.0001), as well as for bilirubin levels (p=0.039, Fig. 2A-C). Interestingly, among all, the AFP scatter plot seemed the most heterogeneous (Fig. 2D). We therefore analyzed the AFP data on basis of the levels below or above the median threshold value of 33 ng/mL (Figs. 2E, F). The results showed that patients with AFP levels above this value had a stronger association with MTD (r=0.3247 and p<0.0001), compared to patients with AFP levels below the median value (r=-0.0093 and p=0.7256).
FINAL MULTIPLE MULTINOMIAL LOGISTIC REGRESSION OF MTD TERCILES $ ON SELECTED FACTORS. MODEL CORRECTED FOR GENDER, AGE, AND ALCOHOL CONSUMPTION
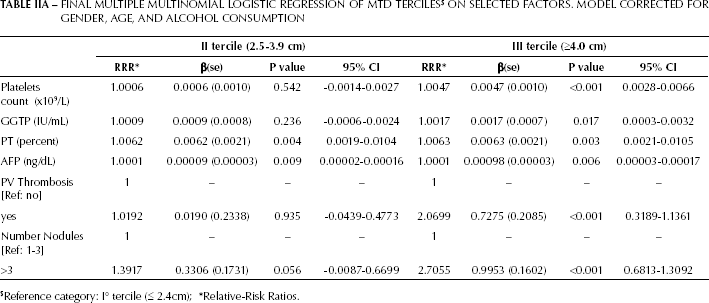
Reference category: I° tercile (≤ 2.4cm);
Relative-Risk Ratios.
MULTIPLE MULTINOMIAL LOGISTIC REGRESSION MODELS OF MTD AND NUMBER OF NODULES COMBINATION $ , ON PLATELET COUNTS AND AFP. THE MODELS ARE CORRECTED FOR GENDER, AGE, AND ALCOHOL CONSUMPTION
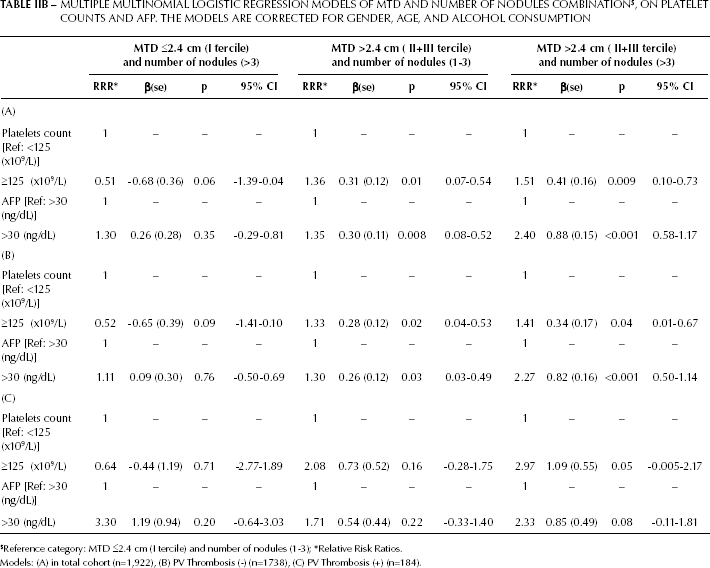
Reference category: MTD ≤2.4 cm (I tercile) and number of nodules (1-3);
Relative Risk Ratios.
Models: (A) in total cohort (n=1,922), (B) PV Thrombosis (-) (n=1738), (C) PV Thrombosis (+) (n=184).
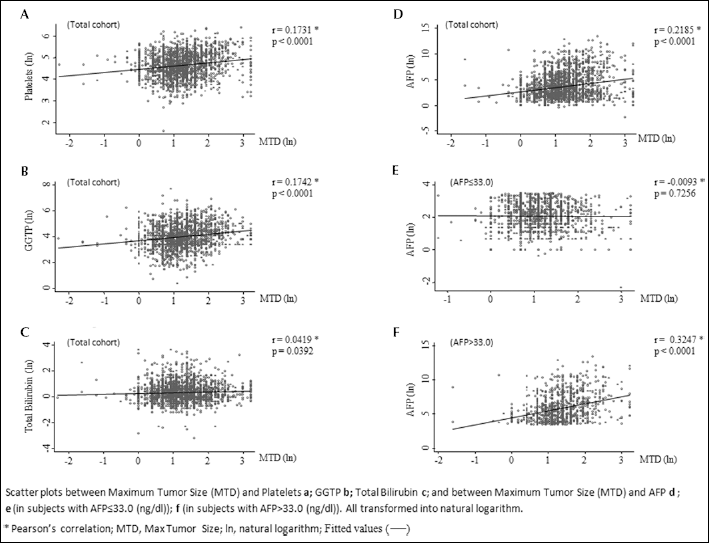
Scatterplots showing the correlation between maximum tumor size and (
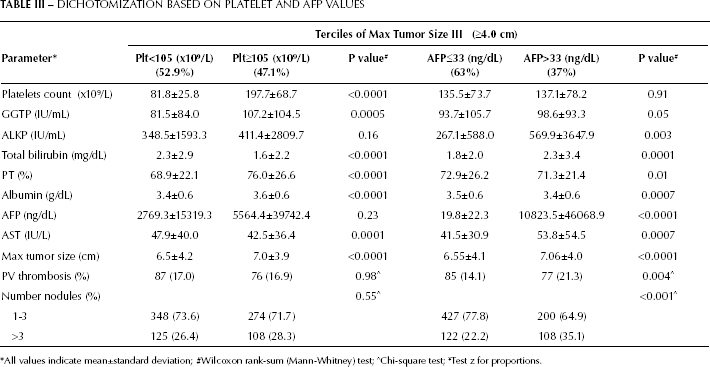
Platelet counts and AFP in relation to tumor size in tercile III patients. The condition of thrombocytopenia during cirrhosis is generally considered to be irreversible, yet the large tumors of tercile III patients were not associated with thrombocytopenia (Tab. I). This suggests that the large size of tumors in tercile III HCC patients might be heterogeneous or reflect more than 1 subset of patients. Tercile III was therefore dichotomized according to the median platelet value of the cohort (105x109/L; Tab. III, left side). Patients with the highest platelet counts had the largest tumors, the highest GGTP levels, and the lowest bilirubin levels. The opposite was true for patients with the lowest platelet counts. By contrast, AFP was not significantly different in these 2 categories of patients. Interestingly, there was a similar proportion of patients in the low and high-platelet counts' groups (52.9% vs. 47.1%). Thus, we can derive that portal hypertension did not limit tumor growth. Seen the relative risk of AFP for tumor size shown in Table IIA, patients in tercile III were then dichotomized according to the median AFP value of the total cohort (Tab. III, right side). Unlike the 2 groups defined based on platelet counts, the high AFP subset (37% of patients in tercile III) with larger tumors had significantly more PVT and multiple tumor nodules, together with higher bilirubin levels, likely reflecting a more invasive HCC biology.
DICHOTOMIZATION BASED ON PLATELET AND AFP VALUES
All values indicate mean±standard deviation;
Wilcoxon rank-sum (Mann-Whitney) test;
Chi-square test;
Test z for proportions.
Survival
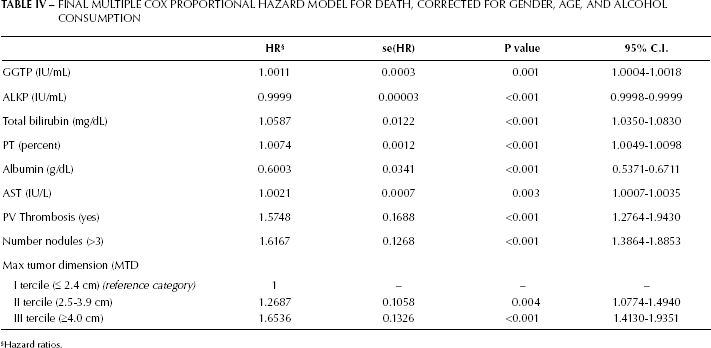
A survival analysis was carried out according to the Cox proportional-hazard model. The final model is shown in Table IV. We ound statistically significant effects of GGTP, bilirubin, AST, PVT, MTD, and tumor multifocality, but not of platelets' nor AFP levels (data not shown). Thus there is a difference in the factors that significantly affected MTD and patients' death; however, the presence of PVT or an increase in the number of tumor nodules were significant factors for both outcomes (MTD and survival).
FINAL MULTIPLE COX PROPORTIONAL HAZARD MODEL FOR DEATH, CORRECTED FOR GENDER, AGE, AND ALCOHOL CONSUMPTION
Hazard ratios.
Discussion
In this analysis a higher MTD tercile was associated with increasing GGTP, ALKP, and AFP levels, with more PVT, as well as with multifocality and decreased survival (Tab. I). GGTP and ALKP have also been reported to be possible HCC markers (15-16-17-18-19-20). The final multiple multinomial (polytomous) logistic regression analysis on MTD size terciles showed a statistical significance in terms of relative risk ratios for platelet counts, GGTP, and AFP, as well as PVT and tumor multifocality (Tab. II). We therefore performed a correlation analysis of several parameters for MTD (Fig. 2). The main finding was the heterogeneity in the AFP/MTD plot (Fig. 2D). When we re-analyzed the data after dichotomizing by the median AFP value, we found 2 different plots: in contrast to the high AFP values, the lower AFP values had an almost flat trend. Since the dynamic range of the low AFP plot was limited, we then compared tercile III patients who were dichotomized at the same value (Tab. III): we found that the high AFP patients had a different parameter profile compared to the low AFP patients, with higher bilirubin values, a higher number of tumors, and an increased incidence of PVT. This indicates that patients with large tumors can have 2 different profiles. We hypothesized that larger tumors can grow better in the presence of better liver functions, but these data do not provide the full explanation to support this hypothesis.
Despite the screening programs, patients usually present at different phases during their HCC natural history (15, 20). A small tumor can be either a slowly growing tumor or a more aggressive tumor diagnosed at an early stage. Conversely, a large tumor can be either an aggressive one or a slowly growing tumor that has been detected late because asymptomatic. At diagnosis, HCC growth characteristics are thus often unclear. As HCCs grow, portal hypertension and hence thrombocytopenia can worsen, as enlarging tumors destroy the hepatic parenchyma. Thus, worsening liver functions could be due to the progression of cirrhosis, to the expanding tumor, or both. Our results show that large HCCs can occur in the presence of both low or normal platelet counts and high or normal bilirubin levels. As previously suggested (21-22-23-24), a more nuanced view allows the possibility of interactions between the liver microenvironment and HCC in tumor growth.
Similarly to what found for tumor size with the final multiple multinomial logistic regression analysis (Tab. IIA), also with the Cox proportional-hazard model for survival (Tab. IV) we found that the 2 parameters with the highest HR were PVT and number of tumor nodules, together with tumor size. Thus, the presence of PVT and the number of tumor nodules were important factors for both tumor size and survival.
In order to better understand the patient's and tumoral phenotype associated with large tumors, tercile III patients were dichotomized according to the median value of platelet levels (Tab. III). As expected, we observed that larger tumors were found in patients without thrombocytopenia. However, there were similar percentages of patients in tercile III with large tumors having either normal or low platelet counts. Patients with higher platelet counts had larger tumors, lower bilirubin, but higher GGTP levels. In the presence of normal bilirubin, high GGTP levels can be possible HCC tumor markers (16, 17). Elevated levels of GGTP also seem to be an especially useful marker in patients with low AFP (18). In this cohort, elevated GGTP levels seemed to be particularly associated with high platelet counts and with low bilirubin levels. Thus, there might be 2 different growth patterns for HCC: one may be associated with normal platelet and bilirubin levels, and elevated GGTP, while the other may be associated with low platelet counts and elevated bilirubin levels. Once again, the hypothesis that tumors can grow larger in the absence of inflammatory processes or in case of poor liver functions is not supported by these observations.
A question still remains: can platelets have a role in tumor growth and not simply reflect the severity of the cirrhosis-associated fibrosis? Interestingly, platelets produce HCC growth factors such as PDGF, FGF, VEGF, and serotonin (8, 9, 20, 21), and can represent a possible mechanism inducing an increase in tumor size, or as part of the tumor microenvironment (22-23-24-25). Additionally, anti-platelet therapy has been suggested to have a role in HCC, especially in patients with normal platelet counts (21) and coagulation system.
Footnotes
Acknowledgements
Author statement. This MSS is approved by all authors, who approve the author listing. I act as guarantor. Author contributions. All co-authors except the first two, collected the clinical data. The first author analyzed the database and wrote the paper, with additional corrections by the co-authors. Dr Guerra performed the statistical analyses.