
Abstract
Background
During the apexification procedure for teeth with open apices, mineral trioxide aggregate (MTA) may be unintentionally extruded. The aim of the present study was the retrospective evaluation of the healing of periapical lesions in permanent incisor teeth with open apices after the unintentional extrusion of MTA.
Methods
The clinical and radiographic records of 55 maxillary permanent central teeth treated by MTA apexification were evaluated. Filled teeth with unintentionally extruded MTA were selected as group 1 (n = 21), whereas the teeth with no MTA extrusion were selected as group 2 (n = 34). For each tooth, the clinical and radiographic records from a 3-year follow-up were investigated.
Results
Complete healing (CH) was observed in 19 teeth (90.4%) in group 1, whereas the same type of healing was observed in all 34 teeth (100%) in group 2 (p>0.05). At the 6-month follow-up appointment, 25 teeth (73.5%) showed CH in group 2, whereas 15 teeth (71.4%) showed CH at the 1-year follow-up in group 1 (p<0.001). At the end of the 3-year follow-up period, the amount of MTA extrusion was reduced in 17 teeth (85%) (p<0.05), whereas it was almost absent in 2 teeth (10%).
Conclusions
The unintentional extrusion of MTA does not prevent the healing of periapical lesions, but may be a delaying factor for periapical healing.
Introduction
The most common reasons for the inflammation or necrosis of the pulp tissue in permanent teeth are caries and trauma (1). Although root canal treatment is necessary under these circumstances, the treatment process is complicated for permanent teeth if their apices are open for reasons such as incomplete root development by the necrosis of the pulp tissue or resorption of the root apex by a periapical infection (2, 3). One of the aims of root canal filling is providing an effective obturation that prevents the transition of any bacteria to the periapical tissues (4). However, the absence of any apical constriction which an obturation material can be placed against makes the obturation process complicated and creates a risk for the extrusion of the root canal filling material beyond the apex into the periapical tissues. Therefore, it is essential to create an artificial apical plug to eliminate those difficulties and the risks associated with the root filling process in teeth with open apices (1–3).
In 1966, the apexification procedure that consists of periodical root canal medication using calcium hydroxide to stimulate the occurrence of an apical barrier was presented (5). Despite widespread clinical practice and successful results (1, 2), the technique has some disadvantages such as long treatment period, need for multiple appointments, reinfection during the treatment period and increased risk of cervical root fracture (2, 3, 6). Because of these disadvantages, different alternatives have been considered. The technique of single-visit apexification using mineral trioxide aggregate (MTA) has been suggested as an effective treatment method by many researchers (7–10), and they have emphasized the advantageous properties of MTA, such as excellent biocompatibility (8, 11), antimicrobial properties (10), stimulation of hard tissue formation (12) and effective sealing ability (8, 12).
MTA requires an orthograde condensation process during the apexification procedure, and the filling material can be unintentionally extruded into periapical tissues because of open apices (2–4). In the literature, the extrusion of MTA during the apexification process has been reported in many case reports (2–4, 13, 14). However, the data obtained were presented within the limits of case reports, and there are no adequate data reported by any study for the evaluation of periapical healing after the extrusion of MTA.
The aim of the present study was the retrospective evaluation of the healing of periapical lesions in permanent incisor teeth with open apices after unintentional extrusion of MTA. In addition, the radiographic evaluation of the resorption of extruded MTA was also sought.
Methods
The present study was performed by evaluating the clinical and radiographic records of 45 systemically healthy patients (28 males and 17 females) who were treated by MTA apexification in the Department of Pediatric Dentistry, Faculty of Dentistry, Bulent Ecevit University, between the years 2011 and 2013. The essential ethical approval to use these records in this study was given by the ethics committee of Bulent Ecevit University (protocol number 2016-20-27/01), and consent forms were received from parents for pediatric patients.
For the present study, the records for the maxillary central incisor teeth treated by MTA (Angelus, Londrina, PR, Brazil) apexification and periodically followed up for 3 years were included. Of them, teeth without any apparent periapical lesions that could be evaluated radiographically were excluded. In addition, teeth with a root fracture or perforation were also excluded. Periapical lesion size was not considered as a criterion. According to the inclusion and exclusion criterion, the completed 3-year clinical and radiographic follow-up records of 55 maxillary central incisor teeth, with single root and canal, which were treated with a similar MTA apexification procedure, were evaluated in the present study. The mean age of the patients was 9.47 years (age range 8–12 years).
In the creation of the groups, filled teeth with unintentionally extruded MTA, regardless of the size of the extrusion, were selected as the experimental group (group 1, n = 21). The extrusion of MTA in each tooth was confirmed by by 2 observers (L.D. and E.H.B.) who had at least 10 years of clinical experience in pediatric dentistry. The teeth with no MTA extrusion were selected as the control group (group 2, n = 34). For each tooth, the clinical and radiographic records of the beginning and 3- and 6-month and 1-, 2- and 3-year follow-ups were evaluated using the procedure described in the study of Sari and Duruturk (15). The same two obervers (L.D. and E.H.B.) evaluated both the clinical and radiographic records according to description of Halse and Molven (16). In situations of initial disagreement between researchers, a final evaluation was reached by consensus following discussion.
According to the procedure (15) periapical healing was considered as follows:
Complete healing (CH; i.e., success):
Clinical parameters: no signs or symptoms; Radiographic parameters: Normal-width periodontal ligament space
Incomplete healing (IH):
Clinical parameters: no signs or symptoms; Radiographic parameters: reduction in lesion size
No healing (NH):
Clinical parameters: indications of acute phase of apical periodontitis Radiographic parameters: no change, or an increase in lesion size.
The amount of the unintentionally extruded MTA which was radiographically observed in the follow-up periods was considered as either unchanged, reduced, almost absent or absent, and the data obtained were recorded.
Statistical analysis
The percentages of CH, IH and NH were compared within each group and between the groups according to the follow-up periods. In addition, the situation of the resorption of extruded MTA was evaluated for each parameter of periapical healing. The chi-square test was used for the statistical analysis. All analyses were performed using statistical software (SPSS Inc., version 19.0, Chicago, IL, USA), and p value less than 0.05 was considered statistically significant.
Results
The results for the periapical healing of all teeth in both groups are shown in Table I. At the end of the 3-year follow-up period, the difference between group 1 and group 2 was not statistically significant (p>0.05) for CH: it was observed in 19 teeth (90.4%) in group 1, whereas the same type of healing was observed in all 34 teeth (100%) in group 2.
Periapical healing results after each follow-up period for the different groups studied
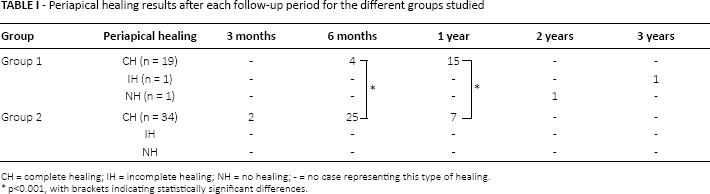
When the teeth with CH were considered during follow-up periods in both groups, 2 teeth showed CH (5.8%) at the third month in group 2, when all teeth in group 1 showed no CH at the same session. Only 4 teeth (19%) showed CH in the sixth month in group 1, whereas 25 teeth (73.5%) showed the same result in group 2 at the same follow-up appointment (p<0.001). On the other hand, at the 1-year follow-up appointment, 15 teeth (71.4%) showed CH in group 1, whereas 7 teeth (20.6%) showed the same result in group 2 (p<0.001). At the 2- and 3-year follow-up sessions, the teeth that previously showed CH in both groups were still in the same condition, and no recurrence of an apical inflammation had occurred in these teeth. In group 1, 1 tooth (4.8%) showed NH at the 2-year session, whereas 1 tooth (4.8%) was still in the condition of IH at the end of the third year.
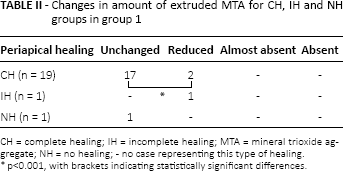
The changes in the amount of extruded MTA for the CH, IH and NH groups for group 1 are shown in Table II. When CH was observed in each tooth in group 1, the amount of extruded MTA was unchanged in 17 teeth (89.5%), whereas the extruded material was reduced in 2 teeth (10.5%) (p<0.001). On the other hand, at the end of the 3-year follow-up period, the amount of extruded MTA was observed to be significantly reduced in 17 teeth (85%), (p<0.05). In 2 teeth (10%), the extruded material was almost absent (Fig. 1), whereas the amount of extruded MTA was unchanged in 1 tooth (5%). In 1 tooth, resorption was not considered because of surgical removal of the extruded MTA at the 2-year follow-up appointment. The distribution of each tooth in group 1 according to the amount of extruded MTA at the end of the 3-year follow-up period is shown in Fig. 2.

(A) Pretreatment of tooth with an unsuccessful trial of a treatment. (B) At the end of root canal filling including mineral trioxide aggregate (MTA) apexification, the arrow shows the extruded MTA; (C) At 1-year follow-up appointment. (D) At 2-year follow-up appointment. (E) At 3-year follow-up appointment. Note that the extruded MTA was almost absent.
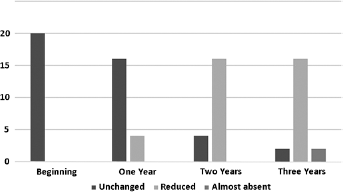
Distribution of teeth according to unchanged, reduced, almost absent and absent amounts of extruded mineral trioxide aggregate (MTA) at the beginning and at 1-, 2- and 3-year follow-ups.
Changes in amount of extruded MTA for CH, IH and NH groups in group 1
Discussion
The extrusion or displacing of root filling material may cause various complications such as severe inflammation, necrosis of the bone tissue or foreign body reaction (17–19). Therefore, it has been suggested to be cautious during the filling process in a root canal treatment procedure since overfilling commonly occurs, especially in teeth with open apices (2, 3, 15). Extrusion of MTA was documented in many cases (2–4, 13, 14), and different clinical results from failure to heal (13) to complete healing (2–4, 14) have been reported. However, the reported data for the evaluation of the clinical outcomes after the unintentional extrusion of MTA are inadequate.
For teeth with periapical lesions, to assess the exact clinical outcomes, long-term clinical and radiographic follow-up are suggested (2, 15) after the treatment is completed. On the other hand, various opinions have been voiced about the appropriate time intervals, such as 1 year (20, 21), 3–4 years (22) and 4–5 years (15, 23), for the optimal follow-up to avoid any remaining concern about whether periapical healing has been completed. In a recent study, Azim et al (24) reported that the average time required for a periapical lesion to heal was 11.78 months, which was similar to previous findings (20, 21) suggesting that 1 year was the minimum time required for most cases to reach the conclusion of a treatment. In the present study, the follow-up period was 3 years for each tooth, and based on the previous comments about the optimal healing time for a periapical lesion after a root canal treatment, this period can be considered as sufficient time to determine the success of the treatments. Thus, in 2 case reports (2, 4) including a case with the unintentional extrusion of MTA, complete healing was reported in each case at the end of 1- or 2-year follow-up periods.
In the present study, no significant difference was found when the percentages of teeth with CH were compared between group 1 (90.4%) and group 2 (100%) at the end of the follow-up periods. From this result, it can be concluded that the extrusion of MTA did not prevent periapical healing. Although the surgical removal of the extruded material may be addressed as a necessary procedure (19), most of the cases in the present study completely healed without any further intervention, and this result may be identified as one of the beneficial properties of MTA. MTA has excellent biocompatibility (2, 8, 11), and it enables the regeneration of periapical tissues to a normal condition (12). Moreover, the material provides bone deposition with minimal or absent inflammatory response (12, 25) by induction of growth factors such as transforming growth factor beta-1 (TGF-β1) and bone morphogenetic protein-2 (BMP-2) (2, 26, 27). In addition, MTA stimulates bone growth over itself, and this situation changes the behavior of osteoblasts in increasing the osteocalcin production (26, 28). Besides, previous studies (2–4) have shown that contact with extruded MTA does not cause a foreign body reaction. Moreover, MTA prevents the continued irritation of periapical tissues with its good sealing ability, and it provides a proper environment for healing of periapical tissues (8–12). For these reasons, stimulation of bone growth, not causing any host response, and good sealing ability may be accepted as 3 important factors to obtain favorable periapical healing results with MTA even when the material is unintentionally extruded.
In a cohort study (29), it was reported that orthograde placement of MTA apical plugs showed promising results, with a high healing rate (90%) for teeth with open apices. On the other hand, in the same study, it was stated that extrusion of MTA and the presence of preoperative apical periodontitis were identified as important prognostic factors for healing. In the present study, no CH was observed in 2 teeth (9.6%) in group 1. In 1 tooth, the periapical radiolucency diminished in size but did not completely disappear, and the healing status of this case was considered to be IH. However, the other case was treated with a surgical intervention for the removal of extruded MTA because of the appearance of acute symptoms of periapical periodontitis at the second year, and the healing status of this case was considered to be NH. Although the percentage of teeth without CH was so low in the present study, it should be noticed that incomplete or failure to heal may be observed in some teeth, even if the extruded material is MTA. Thus, as highlighted by Froes et al (17), it can be suggested that the extruded material may cause deleterious effects on periapical tissues and the healing process.
The remarkable finding in the present study was the significant difference between group 1 and group 2 when the follow-up appointments were compared for the observation time of CH. According to the results, CH was significantly more often observed in group 2 at the 6-month follow-up, whereas the same healing type was significantly more often observed in group 1 at the 1-year follow-up. It can be concluded from these results that the extrusion of MTA does not prevent, but may cause a delay to, periapical healing.
Regardless of extrusion of MTA, CH was observed in 96.4% (n = 53) of all teeth when the 1-year follow-up was completed after treatment. According to previous studies, the time required to observe a complete healing in periapical lesions ranges from 1 to 5 years (15, 20–23). It is well-known that tissue healing and regeneration is faster in younger age groups than in the older individuals (15, 24), and this factor may be a reason that CH was obtained in most of the patients within the first year. In addition, it has been widely reported that immunological changes may cause to delay periapical healing and prolong the healing time (24). Therefore, patients with systemic diseases were not included in the present study, to avoid any factors which could negatively affect the results for periapical healing time. On the other hand, lesion size might be considered as another factor in the time needed to observe CH, but this situation would be applicable if all of the periapical lesions with bigger size were present in the same group. However, this situation was not a point at issue for the present study, and the size of the periapical lesion was not considered as a criterion. Thus, the same evaluation procedure was performed which was used by Sari and Duruturk (15) in their study to investigate the complete healing of periapical lesions after the extrusion of AH Plus.
The other remarkable finding of the present study was the significant reduction in the amount of extruded MTA over time. In 85% of teeth (n = 17), the amount of MTA appreciably reduced. Moreover, the extruded MTA was almost absent in 2 teeth (10%) at the end of the 3-year follow-up period. Although the solubility of MTA is a controversial issue, the literature supports a relationship between the intensity of extruded material and the solubility of MTA, and it is reported that the solubility of MTA increases when the water ratio is higher than the powder (3, 30). In addition, over long periods, increased solubility has been reported (31), and in 1 case (3), it was documented that all extruded MTA was completely resorbed after 7 years. On the other hand, it should be noted that the amount of MTA was significantly unchanged when CH was observed in most of the teeth in the present study, and it can be concluded that resorption is not a prerequisite for complete healing of a periapical lesion.
The findings of the present study showed that extrusion of MTA does not prevent the healing of periapical lesion, but may be a delaying factor for periapical healing. Although, the amount of extruded MTA was reduced and the resorption of the material was observed over time, the resorption was not essential for periapical healing. On the other hand, clinicians should be cautious during the placement of MTA as an apical plug, even with the positive results that were obtained for the extruded material in the present study. If the MTA material is extruded, patients should be informed about the complication and its possible consequences. In addition, patients should be followed up to give a chance to observe periapical healing without any surgical removal of the extruded material, which may be unnecessary because of the advantageous properties of MTA.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: All authors declare that they have no relationship with any people or organizations that could inappropriately influence their work. In addition, all authors declare that they have no conflicts of interest.