
Abstract
Background
A variety of antiinflammatory therapies are employed to promote corneal wound healing. The effects of steroidal and nonsteroidal antiinflammatory drugs on the biomechanical properties of rabbit cornea were investigated over time using tensile tests.
Methods
Full-thickness incisions were made and used to analyze the effects of dexamethasone sodium phosphate 0.1% and diclofenac sodium 0.1% on corneal biomechanical properties during wound healing at 7, 14 and 21 days after surgery.
Results
The full-thickness incision deeply modified all of the mechanical properties. At 3 weeks after incision, regardless of the drug therapy, the tensile modulus was about 70% of the value for the intact cornea.
Conclusions
Topical treatment with dexamethasone was particularly effective during the first week after surgery; the second week after surgery, a similar result was observed in the corneas treated with diclofenac. Low doses of steroidal and nonsteroidal antiinflammatory drugs would seem to have the potential to improve biomechanical properties only during the early stage of the healing process of the cornea.
Introduction
With regard to cornea healing, in recent decades, drug therapies have gained attention as a consequence of the increasing popularity of surgical procedures developed to correct refractive errors of the cornea (1). In 1968, Gasset and Dohlman measured the tensile strength of intact rabbit corneas and those with full-thickness incisions. No wound healing could be detected during the first 6 days. By day 100, the incised corneas reached 50% of the value of normal strength (2). The tensile test represents a very popular method to assess the biomechanical properties of cornea. Specifically, rabbit (3-4-5-6-7), bovine (3, 8) and porcine (9-10-11) models have been frequently analyzed. Often, the biomechanical properties of the animal corneal tissue have been compared with those of the human cornea (3, 7, 8).
The inflation test is another method that has been widely used to assess the biomechanical properties of the corneal tissue. This approach involves the use of a pressure chamber, inflation test rig and mechanical clamps (12-13-14-15). Measurements of pressure and displacement of the apex of the cornea in conjunction with the shell theory allows the determination of the mechanical properties (14, 16).
Concerning the tensile and inflation tests, it is worth noting that each method has its own advantages and drawbacks. Taking into consideration its time-dependent mechanical behavior, cornea is a viscoelastic material like other soft biological tissues (6, 17, 18). Therefore, the speed of testing strongly influences its mechanical properties. Different from the inflation test which prevents a proper control of the rate by which pressure increases on the corneal tissue, tensile tests can be finely controlled for the stress and the strain rate (17, 18). Furthermore, in a tensile test, the specimen can be easily stretched until break occurs (4, 8), while the inflation test may fail to guarantee a proper sealing of the specimen as pressure is increased to high levels. On the other hand, the flattening of the corneal strip is considered the main drawback related to the tensile test, as it may lead to an overestimation of the stiffness (16). However, mathematical procedures can be carried out to compensate for errors due to flattening (16).
Another source of error affecting the mechanical measurements of the properties is related to the thickness distribution (11, 16). The central and superior regions of the human cornea are the thinnest and thickest parts, respectively (19). With regard to the porcine cornea, similar differences have been found (11). In contrast, in the rabbit cornea, the thickness distribution is almost uniform, with a mean value of 407 µm (20) and a mean radius of curvature of 7.5 mm (21).
Corticosteroids are antiinflammatory drugs used to inhibit diverse inflammatory disorders (22, 23). In particular, it has been suggested that dexamethasone inhibits corneal angiogenesis (24). The effects of corticosteroids on the tensile properties of the cornea during wound healing are controversial. For example, twice-daily application of dexamethasone (0.1%) had no effect on corneal wound strength (25). Instead, significant effects were only observed with frequent administration of high doses of dexamethasone, thus showing a dose-dependent efficacy (26). Conversely, Sugar and Chander have reported that corneal wounds treated with dexamethasone (0.1%) 3 times a day for 7 days were significantly weaker than the untreated controls (27). In the results of inflation testing, after 7 days of corneal steroid treatment, administered 4 times a day, no significant reduction in wound strength was observed (9), and similar findings were reported for corneas treated for 21 days with 4 daily applications of prednisolone, diclofenac or flurbiprofen (28). However, after 21 days of treatment with diclofenac sodium (0.1%) applied 6 times a day, a significant increase in corneal wound strength was observed (29). Accordingly, in the current study, the effect of steroidal and nonsteroidal antiinflammatory drugs on the biomechanical properties of rabbit cornea was investigated over time using tensile tests.
Materials and Methods
A total of 50 albino rabbits (2.5-3.5 kg) were used, and all experiments were conducted according to the Association for Research in Vision and Ophthalmology Statement for the Use of Animals in Ophthalmic and Visual Research. This study was approved by the Catholic University of the Sacred Heart Institutional Animal Care and Use Committee (protocol number: 14-1295).
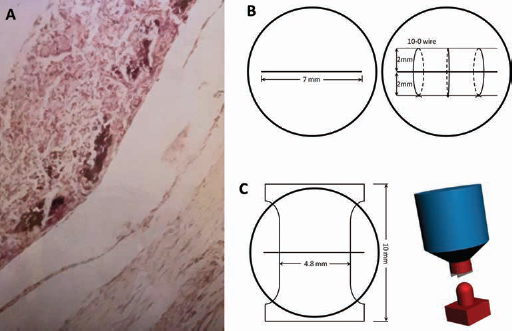
Corneal thickness was measured with an ultrasonic pachymeter. Five rabbits (10 corneas) were used to characterize the intact tissue. A central full-thickness incision (7 mm in length) was made in 45 animals (90 corneas) under general anesthesia. The histology of the involved tissues is shown in Figure 1A.
(
The incision was sutured with 3 interrupted 10-0 nylon sutures (Fig. 1B), following the procedure described by Leibowitz et al (30). After the surgery, the 45 rabbits with corneal wounds were randomly divided into 3 groups, each containing 15 animals (30 corneas). Group A was treated with topical diclofenac sodium 0.1% 3 times a day, group B was treated with low-dose dexamethasone sodium phosphate 0.1% 3 times a day, and group C was treated with saline as control.
On postoperative days 7, 14 and 21, animals (n = 5) from each group were euthanized with an overdose of sodium pentobarbital, and both corneas were harvested. A plastic mold reproducing the curvature of the cornea (R = 7.5 mm) was 3D-printed using stereolithography (31, 32), and an hourglass-shaped punch was used to cut the specimens (Fig. 1C) according to a modified tensile test (ASTM D1708). The “dog-bone” shaped specimen (Fig. 1C) provides an area for clamping higher than specimens having a uniform width (3-4-5-6-7-8-9), thus preventing premature fracture close to or within the grips. The wound (length 7 mm) was perpendicular to the long axis of the specimen (15 mm) and situated at the “waist” of the hourglass (4.8 mm). The specimens were allowed to dry for up to 60 minutes, and then the sutures were removed. To avoid sample slippage, each end of the strip was clamped between 2 identical pieces of sandpaper covering the jaws, and approximately 2 mm at the end of each strip was used for clamping (3-4-5). Tensile tests were performed at a strain rate of 1.4 min−1 (5 mm/min) using an INSTRON 5566 Testing Machine. The strip was preloaded at 0.05 N. During testing the specimens were kept hydrated with saline solution.
According to the shape and size of the specimen, stress-strain curves were obtained. The engineering stress was evaluated as the ratio between the force and the original cross-sectional area (σ = F/A), the mean value of the cross-sectional area was 2.03 ± 0.24 mm2. The engineering strain was calculated as the change in length per unit of the original length (ε = Δl/l). Thus, the stress-strain curve was no longer dependent on the size and the shape of each specimen, and the curve comparisons were possible (3-4-5-6-7, 33, 34). For each specimen, the tensile modulus, maximum stress, maximum strain and strain at break were calculated from the stress-strain curves. In particular, the tensile modulus was computed as a function of the strain level according to the first derivative of the stress-strain curve. Multi-way ANOVA followed by the Tukey post hoc test was used to compare the properties of the investigated groups of corneas (35). The significance level (p) was set at 0.05.
Results
As generally reported for soft biological tissues, a J-shaped stress-strain curve (Fig. 2) was obtained from the intact corneas. The stress-strain curves were characterized by an initial upward concavity (toe region) up to a strain of 0.30 mm/mm, suggesting a relatively high flexibility at low strain levels, followed by an almost linear region.
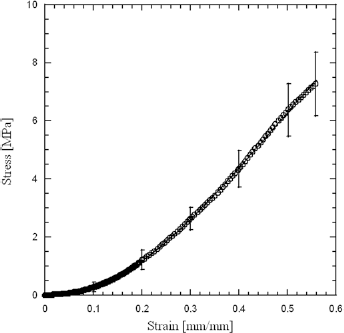
Stress-strain curve for intact cornea loaded at a strain rate of 5 mm/min. The J-shaped or toe region, extending up to a strain of 0.30 mm/mm, suggests a relatively high flexibility at low strain levels. An almost linear region can be detected up to the break point. The error bars represent the standard deviation.
The tensile modulus (Fig. 3) was evaluated from the slope of the linear region of the stress-strain curve. In the initial toe region, the tensile modulus was low, while it increased with strain, reaching a maximum value (17.40 ± 2.80 MPa) at a strain level of 0.30 mm/mm (30%). Further important parameters, such as the maximum tensile stress and strain (7.40 ± 1.10 MPa and 0.56 ± 0.11 mm/mm, respectively), were evaluated from the stress-strain. In particular, the modulus varied from 135 kPa to 5.8 MPa as the strain increased up to 10%.
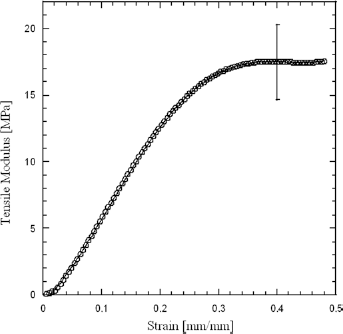
Tensile modulus vs. strain for intact cornea loaded at a strain rate of 5 mm/min. The tensile modulus is derived from the slope of the stress-strain curve. In the initial toe region of the stress-strain curve, the tensile modulus is low, while it gradually increases with strain, reaching a maximum value at a strain level of 0.30 mm/mm (30%). The error bar represents the standard deviation.
Similar J-shaped stress-strain curves were obtained for control group, group A and group B at day 7, 14 and 21 postsurgery. Figures 4, 5 and 6 report the values of tensile modulus, ultimate stress and ultimate strain, respectively, obtained for the incised corneas from week 1 to 3. The corresponding values obtained from tests on intact corneas were considered as reference data. At day 7, the tensile modulus (Fig. 4) was significantly higher (p<0.05) for the corneas treated with steroidal drugs (group B), while no statistical difference was found between the diclofenac (group A) and control group. However, at day 14, the difference was significant (p<0.05) only for the diclofenac-treated group.
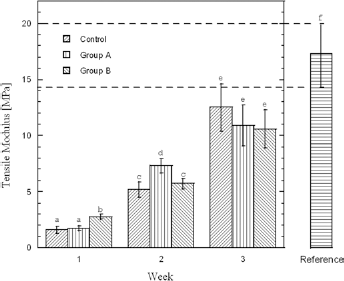
Tensile modulus of control, group A and group B. Column heights and error bars represent the mean values and standard deviations, respectively. Columns displaying different superscript letters are significantly different (p<0.05). Irrespective of the group sample, the tensile modulus significantly increases with time. After 1 week of treatment, the tensile modulus of corneas treated with steroidal drugs (group B) is significantly higher (p<0.05) than that of the control and group A. After 2 weeks, the difference is statistically significant only for the diclofenac-treated group (group A). No difference was observed among the samples after 3 weeks. Irrespective of the treated group sample, after 3 weeks of treatment, the tensile moduli are significantly lower than that of the intact cornea (reference group).
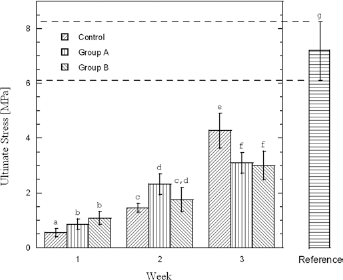
Ultimate stress of control, group A and group B. Column height represents the mean value. Columns displaying different superscript letters are significantly different (p<0.05) – i.e., the difference between the mean values of 2 samples is not statistically significant if 1 or 2 letters are the same. After 1 week of treatment, the mean value of the ultimate stress of group A and group B is significantly higher (p<0.05) than that of control group. After 2 weeks of treatment, no significant difference can be observed between the group treated with dexamethasone (group B) and the control group. Instead, a statistically significant difference is found between group A (treated with diclofenac 0.1%) and control group. After 3 weeks of treatment, the strength of both group A and group B samples is significantly lower than that of the control group. Irrespective of the treated group sample, after 3 weeks of treatment, the strength values are significantly lower than that of the intact cornea (reference group).
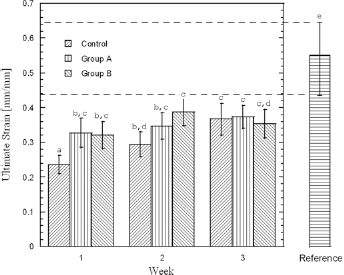
Ultimate strain of control, group A and group B. Column heights represent mean values, and error bars represent standard deviations. Columns displaying different superscript letters are significantly different (p<0.05) – i.e., the difference between the mean values of 2 samples is not statistically significant if 1 or 2 letters are the same. After 1 week of treatment, the ultimate strain of both groups A and B is significantly different than that of the control group (p<0.05). After 2 weeks of treatment, no difference is observed between diclofenac-treated (group A) and dexamethasone-treated (group B) groups, and a significant difference (p<0.05) is detected only between group B and control group. After 3 weeks of treatment, no difference is observed in the ultimate strain values among all groups. Irrespective of the treated group sample, the ultimate strain values are significantly lower than that of the intact cornea (reference group).
At 1 week, the ultimate stress (mean value ± standard deviation) was 1.08 ± 0.24 MPa and 0.86 ± 0.19 MPa (Fig. 5) for the group treated with dexamethasone and diclofenac, respectively. Taking into account the results obtained, a statistically significant difference (p<0.05) was found between the treated groups and the untreated control group (0.55 ± 0.15 MPa). After 2 weeks of treatment, with regard to the maximum stress, no significant difference was found between the group treated with dexamethasone and the control group. Instead, a statistically significant difference (p<0.05) was observed between group A (treated with diclofenac 0.1%) and group C (control).
At day 7, the ultimate strain (Fig. 6) of both groups A and B was significantly different from that of the control (p<0.05). However, after 21 days of treatment, no difference was observed in the ultimate strain values among all groups.
Discussion
The J-shaped stress-strain curve obtained here for the corneal tissue is commonly observed in animal and human corneas stressed through both the tensile and inflation tests (2-3-4-5-6-7-8-9-10-11-12-13-14-15-16). Similarly to other soft and dense biological tissues, cornea can be considered a composite material consisting of a proteoglycan-based matrix reinforced by collagen fibers (36, 37). In the toe region, the mechanical behavior is mainly regulated by the matrix (11, 36, 37). The sudden increase in the tensile modulus is related to the contribution of the collagen fibrils within the stromal lamellae (11). During the loading process, the influence of the fibers sharply increases, and the linear region is related to the fibers straightening (Fig. 2) (36, 37). Compared with other animal models, rabbit cornea has an almost uniform thickness (20), thus reducing errors in computing stress and strain (16). In the toe region (Fig. 2), the tensile modulus, which is also time-dependent (38, 39), increases from 135 kPa to 5.8 MPa up to a strain of 10%. The range of values obtained is consistent with those reported for the rabbit cornea (3, 6) and for the human cornea (40). On the other hand, the tensile modulus values computed at the very beginning of the toe region were consistent with nanoindentation measurements recently reported for the rabbit cornea (41). In the high strain region, the value of the tensile modulus (17.40 ± 2.80 MPa) was consistent with that measured by Hoeltzel et al in the third stress cycle (3). An almost constant tensile modulus of 19.5 MPa has also been observed over an extended stress level range for human cornea (16).
In the current research, the tests were performed at 5 mm/min, obtaining an ultimate stress of 7.3 ± 1.1 MPa and an ultimate strain of 0.57 ± 1.1 mm/mm. However, taking into account that modulus, strength and ductility are time-dependent, the above-reported values are in between those reported for rabbit cornea stretched at 1 mm/min (4) and 10 mm/min (6).
The mechanical properties of the incised corneas (Figs. 4-5-6) showed that steroidal and nonsteroidal antiinflammatory drugs influence the wound healing rate. In particular, at day 7 after surgery, dexamethasone and diclofenac groups presented properties which were higher than those obtained for the control. However, this trend was inverted at day 21, and the maximum stress and the tensile modulus (Figs. 4 and 5) for the control corneas were significantly higher (p<0.05) than those of groups A and B. Instead, strain at maximum stress values (Fig. 6) showed no statistically significant differences between the control and the 2 treated groups. It is worth noting that at 7 days after surgery, the tensile modulus and ultimate stress for group A, group B and control were about tenfold lower than the corresponding values for the intact cornea.
Figure 5 would seem to suggest that antiinflammatory drugs exerted different effects on corneal wound strength at different phases of the wound healing process, and this result generally corroborates previous findings (29, 42, 43). A similar effect of steroid drugs has also been reported in the literature (2, 29). By day 21, scar remodeling should take place, and the negative effects of dexamethasone at this time point are probably related to the inhibition of fibroblast activation and collagenase activity (22-23-24, 44). Corneal scar tissue is characterized by a disorganized collagen matrix with irregularly spaced large-diameter fibrils (45, 46). Petroll et al (47) suggested that the spatial organization of the stress fibers changes as wound closure proceeds. Three weeks after full-thickness incision, Rawe et al (48) found that the collagen fibrils were small and abnormally spaced, and the normal polysaccharide “packing” was still absent 21 months after incision.
On the other hand, the early improvement observed in group B contradicts the results of earlier investigations (12, 25), which indicated that low-dose steroids had no effect on corneal wound strength. Accordingly, further studies are needed to clarify the effects of steroids during the early phase of corneal wound healing. It may be hypothesized that the antiinflammatory action of steroids might facilitate reepithelialization in the immediate postoperative phase by reducing the effects of stromal inflammatory cells and the subsequent release of proteolytic enzymes (49). The positive effects of diclofenac on the tensile modulus and maximum stress, are evident by day 14. McCarey et al found that corneal wound strength was significantly increased by 3 weeks of treatment with diclofenac sodium 0.1% (6 times a day) (29). However, in contrast to previous works focused on theoretical and experimental analyses of soft tissues (50-51-52), tensile tests were performed without cycles of preconditioning.
The current findings are also consistent with the ability of diclofenac to inhibit fibroblast proliferation (53), which is similar to that of dexamethasone. Cleary, this effect would be expected to have negative repercussions on wound strength in the late phase of wound healing, when tissue remodeling plays a key role (43).
Additional studies are also needed to clarify the relationship between the mechanical behavior of the cornea and its structure, from the molecular to the tissue level. These data would increase the ability to predict the effects of various corneal surgical procedures and optimize postoperative antiinflammatory therapy. Within the limitation of the current study, a low dose of steroidal and nonsteroidal antiinflammatory drugs would seem to have the potential to improve biomechanical properties only during the early stage of the healing process of cornea. However, in the late phase of wound healing, a negative effect on wound healing may be recognized.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has any financial interest related to this study to disclose.