
Abstract
Background
Vertebral compression fractures occur in the thoracolumbar junction, causing the collapse of the vertebral body. For their treatment, vertebroplasty and kyphoplasty are used, but it is still unknown which technique is to be preferred.
Methods
Finite element models of the thoracic spine were developed to evaluate the outcomes of vertebroplasty and kyphoplasty. A mild and severe collapse of T10 treated with vertebroplasty or kyphoplasty was studied. Stresses on the endplates and intradiscal pressures were extrapolated to determine the stress distribution in the adjacent structures.
Results
The validation ensured a correct stiffness and a proper kinematic of each functional spinal unit. The results demonstrated that a consolidation following vertebroplasty caused slight variations of intradiscal pressures and stresses. If a kyphoplasty was performed after a mild collapse of the vertebral body, a 25% stress reduction on endplates was found. In cases of severe collapse, when a partial height restoration was achieved, a 15% stress reduction was obtained, while with a full recovery of the anterior wall of the collapsed vertebra, there was a further reduction of 40%.
Conclusions
To reduce the stresses on the adjacent endplates and the risk of fracture, the results suggest a kyphoplasty is to be preferred, trying to restore the initial vertebral body height.
Introduction
Vertebral compression fractures (VCFs) are one of the most frequent consequences of osteoporosis and occur mainly in the thoracolumbar junction (1-2-3-4-5-6-7).
Two minimally invasive techniques consisting of the percutaneous injection of bone cement into the fractured vertebral body (VB) have been developed: vertebroplasty (VP) and kyphoplasty (KP). While VP is used to stabilize the fracture, KP allows the restoration of the VB height, using the mechanical action of a balloon inserted with a catheter before injecting the cement. These techniques have good outcomes in the short-term: there is a decrease in pain, as quantified with visual analog scale (VAS) scores, and a low rate of complications (1, 2, 4, 5, 7-8-9). Moreover, KP improves the wedge angle (2°-8°) and the VB height (2-8 mm) (2, 4, 5, 8). However, it is difficult to determine which technique is more effective, mainly because KP is more recent than VP, and long-term clinical follow-ups are not available yet.
After these treatments, a new VCF is often reported (3%-52% of cases). Its location is most often (60%-70%) adjacent to the operated VB (8, 10). Adjacent vertebral fractures are probably due to increased stiffness, load transferring, shifted body weight and progression of osteoporosis, as already demonstrated (11, 12).
Most of the clinical studies available do not clarify where the fractures start and distinguish only between fractures above or below the treated level. Fribourg et al found that 90% of the subsequent fractures were adjacent (60% above, 25% below and 5% between) (10). In a study by Trout et al, 41.4% of 186 fractures occurred in vertebrae adjacent to the VB treated with VP, while 50.6% of the adjacent fractures were cephalic to the treated vertebra. The authors remarked that VBs adjacent to those treated with VP showed a higher fracture risk (13).
Few authors have reported that the structures where new fractures could start are the endplates (EPs), highlighting the importance of reducing local stresses to reduce fracture risk. Another clinical study found that the majority of spontaneous and incidental fractures (57% of 274 and 59% of 186, respectively) occurring in osteoporotic patients before VP were located along the superior EP. Furthermore, 41.4% of 186 incident fractures occurred adjacent to treated vertebral levels (mainly above). Some authors have suggested that EP fractures can be an indicator of force distribution in the spine after VP (14).
Computational models have been used to study different aspects of VP and KP: the efficacy of VP according to damage, cement quantity and the effect of disc degeneration (15), the effect of position and volume of the injected cement (12), the influence of different type of augmentation and the role of cement on the load transfer in single functional spinal units (FSUs) (16).
Dabirrahmani et al developed a L2-L4 osteoporotic model with a weakened anterior wall to evaluate the importance of height restoration, stiffness and volume of cement following KP (17). Rohlmann et al used a 3-dimensional, nonlinear model of L1-L5 to estimate the muscular forces during standing (for an intact lumbar spine, after VP and KP) and to determine intradiscal pressure (IDP) and maximum stress in the vertebral EPs before and after augmentation (11, 18). The same model was used in a probabilistic study to evaluate the effects of fracture shape, amount and distribution of cement, elastic modulus of bone cement and cancellous bone and fracture localization on the stresses after VP (19).
The present work is part of meaning that it is an ongoing project a project aimed at developing a validated finite element model of the thoracolumbar junction, with the highest incidence of wedge fractures observed in T9-L4 (1, 3, 6). The goals of this study were to validate a T9-T11 model and to evaluate the biomechanical outcomes for VP and KP by means of a computational comparative analysis to study the stresses arising within the adjacent anatomical structures.
Methods
A 3-dimensional, nonlinear finite element model of T9-T11 was created from computed tomography (CT) scans (512 × 512 pixels/slice, slice thickness of 0.625 mm; BrightSpeed scanner; General Electric Medical System) of a healthy human male without spinal pathology (age 40). The geometry of the VBs was extracted by thresholding the gray value scales. The anterior part of each VB was modeled considering both the cortical and trabecular bone (Tab. I) and meshed using hexahedral elements, while the posterior processes were meshed using tetrahedral elements. The mechanical properties of the osteoporotic bone were reduced with respect to the normal values, keeping the same percentage decrease reported by Chae and colleagues (23).
Material properties used for each structure, with literature references
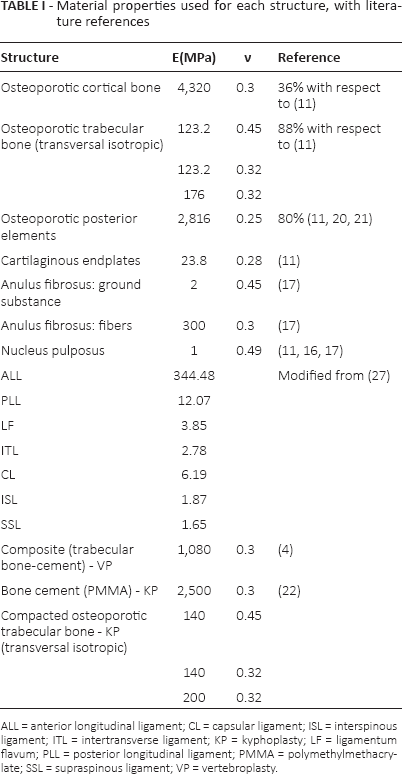
ALL = anterior longitudinal ligament; CL = capsular ligament; ISL = interspinous ligament; ITL = intertransverse ligament; KP = kyphoplasty; LF = ligamentum flavum; PLL = posterior longitudinal ligament; PMMA = polymethylmethacrylate; SSL = supraspinous ligament; VP = vertebroplasty.
Intervertebral discs (IVDs) were obtained by extruding the adjacent EPs, and their height was in accordance with anatomical data (24). The IVDs were divided into the nucleus pulposus (NP) and anulus fibrosus (AF) with a volumetric ratio of 3:7 according to Kapandji (25), while the center of the NP was located slightly posterior from the center (26). The NP and AF were meshed in ICEM CFD 12.1 (© ANSYS Inc) using hexahedral elements. Four composite rebar layers were embedded in an isotropic solid matrix: Two bundles of tension-only linear elastic fibers, having an orientation angle of ± 30° with respect to the transverse plane were assumed for each layer (17). A cartilaginous EP of 0.7 mm was considered on the upper and lower surfaces of each IVD (20, 21). Ligaments were modeled using tension-only spring elements: the anterior longitudinal (ALL), posterior longitudinal (PLL), intertransverse (ITL), flavum (LF), capsular (CL), interspinous (ISL) and supraspinous (SSL) elements. Literature stiffness values (27) were readjusted in the validation step to match data describing the range of motion (ROM) of the thoracic spine.
A mesh convergence analysis was performed by monitoring the stress values on EPs, and a good compromise between accuracy of the solution and computational cost was found. The number of elements of the complete T9-T11 model was 435,688.
To validate the stiffness of a VB, the compression of T10 was simulated and compared with literature data (28). In further simulations on T9-T11, the stresses on the cortical bone (29) and the IDP (11, 16), were compared with works considering thoracolumbar FSUs. The kinematics of each FSU was validated in flexoextension, lateral bending and axial rotation, applying pure moments up to 10 Nm. The moment/angle curves were obtained (calculating the ROM and the stiffness of the FSUs) and compared with literature data (22, 30, 31). To investigate the outcome of surgical procedures in terms of stress on adjacent structures, we hypothesized 2 initial cases of patients who underwent a VCF causing a collapse of T10 and leading to a wedged shape (1-2-3-4-5-6-7). These reference conditions were simulated assuming a 25% reduction (mild collapse, 13° wedge angle) of the anterior VB height with respect to the intact vertebra or a 50% (severe collapse, 26°) reduction (Fig. 1).
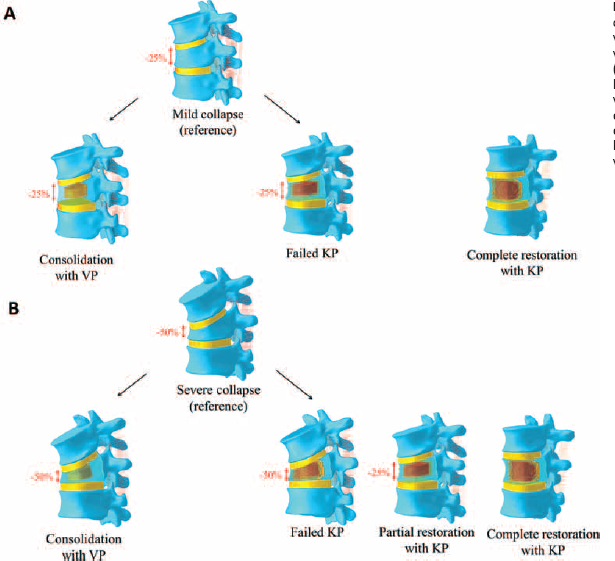
Representation of the clinical cases simulated: a mild (
These clinical situations can be treated using VP or KP. VP allows for the consolidation of the fracture by bone cement injection. Thus, we simulated it with a composite material core within T10 VB, with mechanical properties in accordance with Chae et al (23). KP can potentially restore the anterior VB height with a balloon expansion followed by cement injection. The balloon expansion was described assuming a compaction of the trabecular bone of 2.5 mm radially to an inner cement core and mechanical properties according to Sun and Liebschner (12). The quantity of polymethylmethacrylate (PMMA) injected was about 20% of the total VB volume (12, 19), corresponding to 3-4 mL, as used in clinical practice (2, 5). In the case of a mild collapse of T10, we simulated a failed or a complete restoration of the VB height, while in the severe case, we reproduced a failed restoration, a partial height restoration of 25% (wedge angle of 13°) and an ideal complete restoration.
Each model was loaded according to Rohlmann et al (11). A follower load (FL) of 200 N that takes into account the local muscle forces was applied just behind the center of the VB (Fig. 2): its position was optimized for each FSU to minimize any rotation about the anatomic planes (rotation <5% of the total ROM). An upper body weight (FBW) of 100 N was then applied anteriorly. The FBW load was reduced with respect to that used by Rohlmann and colleagues (11, 18, 32, 33), considering that the loads on the thoracic segments are less than those born by the lumbar spine (34). The lever arm of each force was recalculated considering the natural curvature of the thoracic spine (11). The condition of standing was obtained applying the FL and the upper body weight. The flexion induced on the spine was compensated for by applying an extension, representing the contraction of the dorsal muscles. Since force on the erector spinae (FES) increases with the degree of collapse of T10, its contribution to the axial compression of the thoracic segment was taken into account and summed to the initial value of the FL.
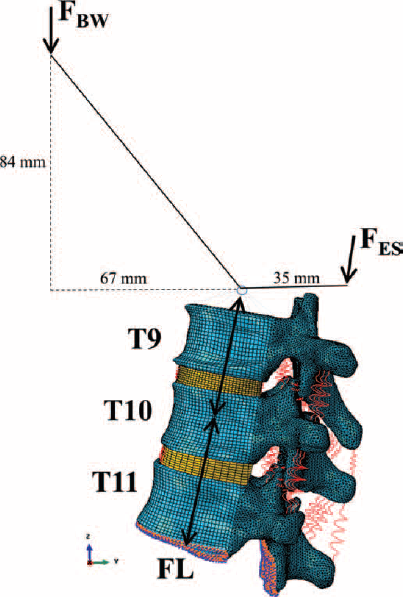
Scheme of loads applied on the thoracic segment as suggested by Rohlmann et al (11). The lever arms were measured from CT data. BW = body weight; ES = erector spinae; FES = force on the erector spinae; FL = follower load; F_BW = body weight force.
Therefore, the total FL applied on the intact model was 351 N, while on the models representing a mild and severe collapse of the VB, a FL of 374 N and 395 N, respectively, was used. The inferior EP of T11 and the lower facet joint were completely constrained. The outcomes of different clinical scenarios were compared in terms of stresses arising on the structures adjacent to the treated level. To investigate the hypothesis that adjacent fractures could originate from high stresses on the EPs (14), we investigated the von Mises stress in these tissues and the IDP. The results are reported as absolute values and discussed as percentage stress or IDP reduction with respect to the initial reference condition.
Results
The validation ensured that the stress on bony structures and the IDP values were consistent with literature data. The predicted compressive stiffness (31.3 kN/mm) was comparable to the 35.0 ± 9.7 kN/mm reported by Dall'Ara et al (28). Moreover, the local strain values experimentally measured during compressive tests on the surface of T10 by Hongo et al (29) using strain gauges were in good agreement with our predictions (Fig. 3a). The IDP values obtained with our intact model (0.89 MPa) were of the same order of magnitude as those calculated in previous computational works reporting values between 0.45 and 0.65 MPa (11, 16). The kinematic of both FSUs was in good agreement with the in vitro kinematics, considering the moment/angle curves (22, 30) and the total ROM (30, 32) (Fig. 3b, c).
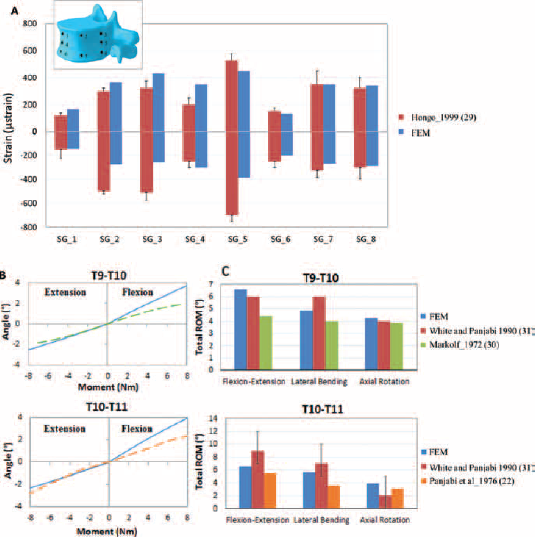
Validation of strain values (
The results of the simulation of the first clinical case (Fig. 4a) demonstrated that a consolidation following VP caused a slight increase of the IDP (1.9% and 1.1% above and below T10, respectively), while the stress values on the EPs decreased by 0.6%-1.9%. A failed KP produced almost the same outcome (maximum IDP increase: 2.3%; maximum stress decrease on the EPs: 2.2%) as VP, while with a total restoration of the anterior VB height, there was a 7.6% decrease of IDP in both discs, and the maximum von Mises stress on the adjacent EPs decreased by up to 12%-31%.
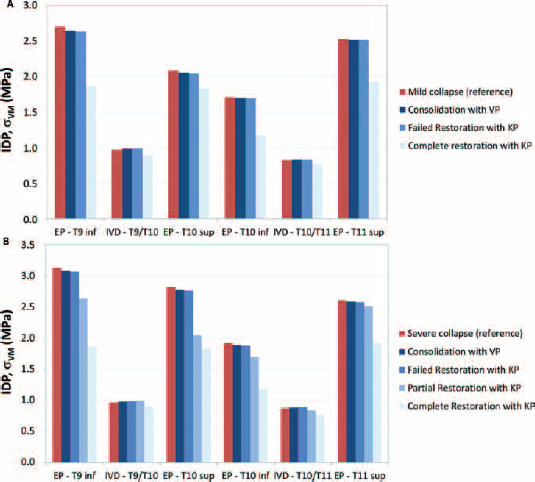
Absolute values of von Mises stresses in the endplates (EPs) and intradiscal pressure (IDP) predicted in the initial untreated condition of mild collapse (
Concerning the severe collapse (Fig. 4b), we found that a consolidation following VP produced an increase of the IDP by 2.5% and 1.4% above and below T10, respectively, while the stress values on the EPs decreased by 0.8%-1.7%.
A KP resulting in an augmentation without any height improvement led to the same results as the consolidation case (maximum IDP increase: 3%; maximum stress decrease on the EPs: 2.2%). KP with a 25% restoration of the anterior VB height led to a 3% increase and a 4% decrease of IDP in the superior and inferior discs, respectively, while the maximum von Mises stress on the adjacent EPs decreased by up to 11.7%-27.7% just below and above the treated level. A total restoration achieved with KP allowed for a reduction of the IDP values (7% above and 14.5% below T10), while the reduction of von Mises stress in each EP was greater than in the previous case (between 35.6% and 67.7%).
Discussion
Clinical experience has demonstrated a high incidence of VCF affecting the thoracolumbar spine (1-2-3-4-5-6-7). Two surgical techniques are mainly used: VP consolidates the fracture by cement injection, while KP tries to restore VB height inflating a balloon before augmentation. Many studies have reported a significant number of adjacent fractures after treatment (8, 10, 11-12-13-14, 35). The aim of this study was to investigate the stresses acting on the tissues surrounding a collapsed VB after surgery, with a numerical comparative analysis.
The validation step provided a reliable model with stress in the bone and the IDP values in good agreement with the literature data (11, 16, 29). Our values were of the same order of magnitude, and any observed differences would probably be due to variations in geometry, mechanical properties and level considered.
The kinematics were validated comparing the ROM of each FSU with the experimental data available to date in the literature. The observed discrepancies can be discussed considering that experimental measurements may be affected by intrinsic errors and imprecisions, thus limiting their accuracy. In this light, the experimental data used as a validation were quite old, so it can be inferred that the testing equipment was less accurate than modern devices. Moreover, only limited data, without dispersion or standard deviations, were published, probably due to the low number of specimens considered. Thus, the overall kinematic response of our model can be considered acceptable.
Our investigation highlighted the importance of restoring the height of a collapsed VB, to reduce the stresses on the adjacent structures: as the surgical procedure allows the achievement of a less prominent wedged shape, the stress significantly decreases in the adjacent EPs, especially superiorly. This effect is mostly due to the variation in the shape of the treated VB. We predicted an average stress reduction of about 23% in case of a successful KP leading to a 25% restoration starting from a mild collapse (75% of the original intact height) (Fig. 5a). In their study, Rohlmann et al (11) found the same trend for the same percentage restoration, but starting from a 35% collapse (65% of the original intact height). In the case of a severe collapse (50% of the original intact height), with a partial height restoration, an average stress reduction of 15% was calculated, while with a full recovery of the anterior wall of the fractured vertebrae, there is a further stress reduction of about 40% (Fig. 5b).
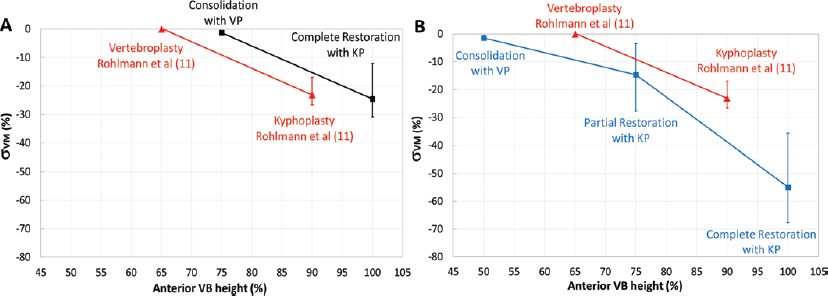
Percentage decrease of von Mises stress as a function of the anterior vertebral body (VB) height predicted after treatment with vertebroplasty (VP) or kyphoplasty (KP). Zero percent corresponds to the initial untreated condition of mild (
The simulated scenarios represent the extremes of clinical conditions. According to clinical intraoperative measurements on collapsed vertebrae treated with different procedures, a certain amount of height restoration is achieved only in 66% of treated patients (8). Even if clinical data are obtained using different methods and hard to compare in terms of type of collapse, the most probable initial scenario would be a collapsed VB having a 21%-63% reduction of the anterior height (8); in this light, the initial conditions (25% and 50%) we simulated are reasonable. Considering that treatment using VP or KP could lead to a 7%-28.8% height restoration (8), the most realistic situation after surgery would be to represent something between a consolidation (or a failed KP) and a 25% height restoration (complete restoration according to a mild collapse, and a partial restoration for a severe collapse).
The connection between height restoration and increased fracture risk on the adjacent spinal levels is not well understood. Aquarius et al (35) proposed that restoring the VB height is important to eliminate the occurrence of off-axis loads in neighboring vertebrae: this would change sagittal alignment, finally reducing the fracture risk on adjacent vertebrae (35).
An open question regarding VP and KP is which technique is to be preferred. Dabirrahmani et al (17) noted that the EPs of the treated vertebra are the most prone to fracture, followed by those of the superior and inferior level. Trout et al reported that implanting cement in a VB during VP could result in altered forces within the spine and lead to an increased incidence of fractures of the cephalic endplate (14). In our study, we found that the components bearing higher stresses were above the fracture, but further investigation, with a model considering more FSUs, is needed to better understand adjacent fractures.
We also found a minimal difference between the initial condition, the results of consolidation with VP and failed KP, demonstrating that the presence of bone cement in the treated VB is negligible. VP produces a consolidation of the vertebra with a negligible decrease of stresses on the EPs (less than 2%). The good postoperative results may be due to mechanisms other than mechanical stabilization of the fracture, such as thermal injury to the nerve endings resulting in immediate pain relief for the patient (36).
Some limitations affected our model: the validation was performed comparing the ROM of the single FSU only with the few available data. Only a standing condition was simulated: this scenario is not clinically relevant, since the most critical condition for the spine involves high degrees of flexion or weight carried with the upper limbs. Future investigations will take into account these conditions.
It must be considered that this is only a preliminary part of a project aimed at the reconstruction of the whole thoracolumbar junction (T9-L4). With a complete model, it will be possible to include in the analysis all of the segments with the highest incidence of vertebral fractures and to simulate the effect of VP or KP on different FSUs.
A numerical model of T9-T11 was validated and used to simulate different degrees of wedge collapse of T10 VB. VP and KP were simulated and the stress distributions on the EPs were investigated. In the case of mild collapse after KP, we noticed an average von Mises stress reduction on the EPs of about 25%. In the case of a severe collapse, when there is a partial height restoration, an average stress reduction of 15% was calculated, while with a full recovery of the anterior wall of the fractured vertebra there was a further stress reduction of about 40%. In both clinical cases, VP produced negligible variations in the state of stress. Thus, to reduce the stresses and consequently the risk of fracture, the results suggest a KP is better than a VP, trying to restore the initial (uncollapsed) VB height.
Footnotes
Financial support: The current study was not supported by any funding.
Conflict of interest: The authors declare that they have no conflict of interests with any subject discussed within the current study.