
Abstract
Purpose
The aim of the study is to report our first impressions about Adherus, a novel dural sealant, used in neurosurgical endoscopic transnasal procedures.
Methods
We retrospectively reviewed the clinical and surgical records of the first 11 patients with intraoperative high-flow cerebrospinal fluid leak treated with the aid of Adherus at our center between February and October 2014. The healing at the level of the dural plasty was monitored and evaluated radiologically and with regular endoscopic inspections.
Results
With a median follow-up of 210 days, no postoperative CSF leak or surgical site infections were found in any of the cases.
Conclusions
Based on our preliminary experience, this new dural sealant seems to provide an effective aid in dural plasty during endoscopic transphenoidal procedures.
Keywords
Introduction
Cerebrospinal fluid (CSF) leak is the most common complication of transphenoidal endoscopic surgery and even in very experienced hands a 100% success rate in dural repair is not achieved (1). High-flow CSF leaks are obviously the most challenging kind and a lot of techniques and materials have been used in order to obtain a so-called watertight closure (2-3-4). Different dural sealants employed in reinforcing the closure have been already examined (5-6-7-8-9) but there are few studies that evaluate the use of this type of sealants in transphenoidal endoscopic surgery (10) and no study at all about sealants with a polytheyleneimine (PEI) component. The aim of this study is to report our first impressions regarding the effectiveness of a new dural sealant (Adherus, HyperBranch Medical Technology, Durham, NC, USA) in endoscopic transphenoidal surgery.
Material and methods
We retrospectively analyzed the surgical and clinical records of all the cases with a high-flow intraoperative CSF leak for which we employed the Adherus sealant during endoscopic transphenoidal surgery. From February 2014 to October 2014 we retrieved 11 cases. In 8 cases, the suprasellar arachnoidal spaces were opened. These included 1 patient with Rathke Cleft Cyst, 2 patients with a recurrent nonfunctioning pituitary adenoma, and 5 patients with a pituitary adenoma extended into the suprasellar region. In the other 3 cases, the third ventricle was opened: these included 2 patients with a craniopharyngioma and 1 patient with a recurrent GH secreting pituitary adenoma. All patients signed the preoperatory consent form.
Endoscopic surgical technique
A third-generation cephalosporin was given 1 h before surgery. In nonrecurrence cases, a bilateral paraseptal sphenoidotomy was performed with a rigid 4 mm 0° scope. A septoplasty or ethmoidectomy was performed when septal spur or other anatomical variants blocked direct access to the sphenoid sinuses, otherwise the removal of the right middle turbinate and a gentle lateralization of the left middle turbinate was enough to approach the sphenoid. Before enlarging the sphenoidotomy inferiorly, a subperiosteal dissection of the mucosa of the superior choanal edge was performed in order to preserve the septal branches of the sphenopalatine arteries. These are usually located under the tail of the superior turbinate. We thus preserved the vascularization of the Hadad-Bassagasteguy flap. The intersphenoidal septa, roustrum sphenoidalis, and the posterior third of the nasal septum were removed to get wide control over the sella and to permit a 4-hand technique (11). In recurrence cases, the previous access was used to expose the sellar floor, which was drilled with a diamond burr until the periostium was visualized. A wider opening, if needed, was achieved with piecemeal bone removal from one cavernous sinus to the other. A “U” or “crux” incision of the periosteum with a microscalpel was performed. Whenever possible, an extracapsular dissection and a complete exeresis of the lesion was performed, with preservation of the normal gland and pituitary stalk. In all cases, the diaphragma sellae was opened and in 3 cases it was also necessary to open the third ventricle to achieve complete removal of the lesions. The skull base plasty was then performed with an autologous tissue: mucosa of the middle turbinate or fascia lata. Adherus sealant was then used to reinforce the plasty.
After effective hemostasis and thorough drying of the surgical field with the aid of aspiration and cottonoids, we applied the sealant in a “single shot” fashion, covering not only the plasty surface but also exceeding its boundaries on the adjacent nasal tissue. We waited approximately 2 min to check the effectiveness of the gelification of the sealant and to inspect for immediate leakages. No Valsalva maneuvers were performed routinely. No other reinforcement materials were employed other than bilateral nasal tampons.
Postoperative management
No postoperative lumbar drainage was placed. A postoperative computer tomography (CT) scan of the head and paranasal sinuses or of the cervical spine was obtained within 24 h. No postoperative antibiotics were used. Nasal packings were removed 2 days after surgery. A clinical, radiological, and endoscopic follow-up was performed to evaluate the healing at the level of the dural plasty.
Illustrative case
A 51-year-old man presented with an incidental diagnosis of suprasellar lesion. The magnetic resonance imaging (MRI) of his head showed an extraassial lesion in the intrasellar and suprasellar left regions, isohyperintense in all sequences with no contrast enhancement and a small portion of hypointensity in T1 sequences (Fig. 1).
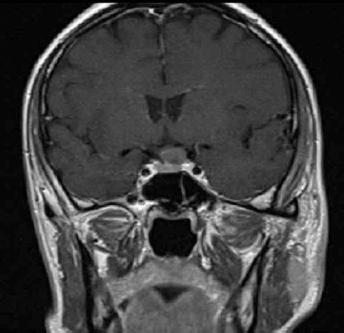
Coronal T1 preoperative MR showing an extraassial lesion in the left intrasellar and suprasellar regions.
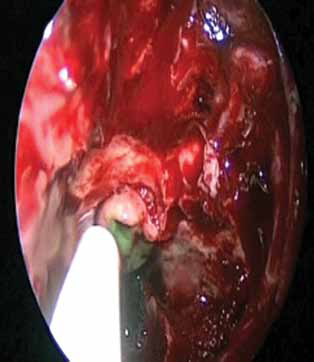
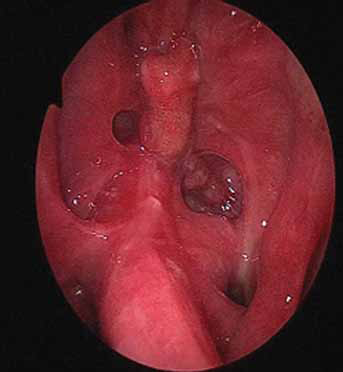
This radiograph could be indicative of Rathke Cleft Cyst, craniopharyngioma, or other rarer suprasellar lesions. Preoperatory pituitary hormones were normal. He underwent endoscopic transsphenoidal total resection of the lesion. The intraoperative appearance of the lesion was that of an elastic cyst in contact with the pituitary stalk. Suprasellar cisterns were opened and a high-flow CSF leak occurred. Dural plasty was performed, as described, with mucosa of the middle turbinates and Adherus sealant (Figs. 2-5).

Intraoperative endoscopic view of the defect.

Intraoperative endoscopic view of the dural plasty.
Intraoperative endoscopic view during the delivery of Adherus sealant.
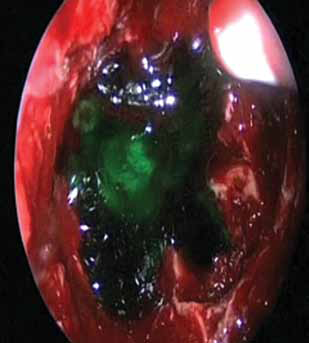
Intraoperative endoscopic view once the dural sealant is applied.
A histological examination of the collected material was conducted for Rathke Cleft Cyst. On postoperative day 5 the patient was discharged. An MRI scan and an endoscopic evaluation 3 months after surgery showed complete resection of the cyst and good healing of the nasal mucosa (Figs. 6 and 7).
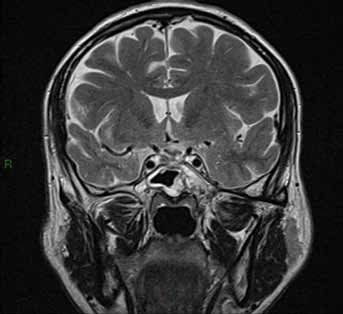
Coronal T2 postoperative MR showing complete resection of the cyst.
3-month postoperative endoscopic evaluation showing good healing of the nasal mucosa.
Results
We reported no major complications during the delivery of the sealant. The postoperative CSF leak and infection rates were 0%. No other complications were reported. In particular, at the first postoperative endoscopic evaluation, no misplacing of the dura repairing material was noted. The healing of the dural plasty and of the nasal mucosa was monitored during the following weeks and no differences were observed between the group of patients in which Adherus was used and all the other patients that underwent endoscopic transphenoidal surgery during the same period. In specific, no particular inflammatory reaction or healing problems were noted in the patients treated with this sealant. The complete reabsorption of Adherus was achieved in a mean time of 50 days (40-60) The mean follow-up of the patients was 210 (330-90) days.
Discussion
Currently, endoscopic transphenoidal surgery for sellar and parasellar tumors is widely used and these lesions are successfully removed through this route (12). Postoperative CSF leaks are a potentially dangerous complication and can have serious consequences like meningitis. For this reason, especially in the case of high-flow CSF leaks, good reconstruction of the iatrogenic skull base for dural and arachnoidal defects is mandatory for a successful operation. Many dural repair techniques have been described but in recent years the vascularized pedicled nasoseptal flap has gained popularity for endoscopic repair of skull base dural defects and success rates are reported to be between 89% and 95% (13, 14). Potential complications for this technique have also been reported (15). Our reconstruction technique for high-flow CSF leaks consists of a multilayered closure with mucosa of the middle turbinate or fascia lata and a final layer of a dural sealant (Adherus). When not used or devascularized in a previous surgery, the septal flap is preserved and can be used in the event of revision surgery.
All dural sealants commercially available form a polyethylene glycol (PEG)- based hydrogel. Adherus surgical sealant was also designed with a polytheyleneimine (PEI) crosslinking component that has already been used and recognized for its antimicrobial properties. We believe that this feature may limit or prevent infections at the surgical site. Another special feature of this dural sealant is its slow rate of degradation, which may contribute to providing a watertight closure for at least 40 days while the dura heals.
We do not report any complications in our small series. However, a larger population would be needed to confirm our data.
Conclusion
This new dural PEG-PEI sealant seems to be effective for dural closure, especially in endoscopic transphenoidal surgery; its antimicrobial properties may limit or prevent infections. Further prospective, randomized, controlled, double-blinded studies should be performed to validate our results.
Footnotes
Financial support: The authors received no financial support for this study.
Conflict of interest: The authors report no conflict of interest concerning the materials or methods used in this study or regarding the findings presented in this paper.