
Abstract
Purpose
Local neuropeptide release has a critical role in the initiation and progression of an inflammatory response. This study investigated the effects of different restorative materials on periodontium in this regard, by evaluating their neuropeptide-producing effects on gingival crevicular fluid (GCF).
Methods
The study included 14 patients suitable for metal-ceramic, composite and amalgam restorations. Four weeks after periodontal therapy, the restorations were performed. Study groups were constituted regarding the tooth/restoration surfaces contacting gingiva in each patient: 1 ceramic surface of a metal-ceramic crown (ceramic group), its opposite metal surface (metal group), 1 composite surface (composite group), its opposite enamel surface (opposite-composite group), 1 amalgam surface (amalgam group), its opposite enamel surface (opposite-amalgam group) and 1 nonrestored enamel surface (enamel group). Four weeks after dental restorations, clinical data and GCF were obtained from the group sites. Clinical data, GCF volume and its proinflammatory cytokine profile were utilized to evaluate the periodontal health. GCF levels of substance P (SP), neurokinin A (NKA) and calcitonin-gene related peptide (CGRP) were determined by ELISA for revealing the neuropeptide levels.
Results
GCF volume was found to increase in all groups compared with the enamel group (p<0.05). SP and NKA levels were higher in the ceramic, composite and amalgam groups than those in the enamel group (p<0.05). SP and NKA levels were also higher in the composite and amalgam groups than those in the opposite-composite/amalgam groups (p<0.05).
Conclusions
These results suggest that ceramic, composite and amalgam materials may uniquely trigger local neuropeptide release in periodontium.
Introduction
Local neurogenic responses are known to be involved in the mechanically and/or microbiologically induced inflammatory reactions of periodontium (1, 2). In this process, the neurons of gingivomucosal nerves locally release neuropeptides to modify the periodontal inflammatory response, and this reaction is termed as neurogenic inflammation (1). Substance P (SP) and neurokinin A (NKA) are members of the tachykinin family of neuropeptides (3) which are derived from the same gene (4, 5) and have similar roles (6). These peptides are stored in the secretory granules of sensory unmyelinated c-type fibers, and they also present both in the primary sensory neurons and their peripheral branches (7). SP and NKA have been suggested as neurogenic inflammatory markers in the pathogenesis of periodontal disease (1, 3, 8). Calcitonin-gene related peptide (CGRP) is another neuropeptide produced by the alternative processing of the calcitonin gene mRNA transcription (9), which is released from different sources other than neurons (10, 11). CGRP generally interfaces with SP in the peripheral endings of sensory neurons to potentiate the release and effects of SP in the neurogenic inflammation (7, 12). It has been demonstrated that CGRP has a direct vasodilatory effect (13), and/or it prolongs the SP reactions (14).
It is generally considered that placing the restoration margins subgingivally should be avoided, wherever possible, since this phenomenon may trigger periodontal disease (15, 16). Subgingival restorations may unfavorably lead to dental biofilm accumulation which consequently stimulates gingival inflammatory response (15-16-17). Thus, subgingival restorations may provide a less suitable environmental condition for gingival health compared with the supragingival ones and unrestored tooth surfaces (15-16-17). It is suggested that the material type is closely related to gingival/periodontal inflammatory response around the subgingival restorations, regardless of plaque-induced reactions (18, 19). Therefore, it may also be essential to determine the adverse effects, biocompatibility and toxicity of restorative materials, when locating them adjacent and/or subjacent to gingiva to meet aesthetical demands.
Although inflammatory effects of restorative materials on periodontium were also revealed histopathologically (16, 19), most studies have investigated periodontal inflammation by means of clinical examination (17, 20-21-22-23-24-25). Few clinical studies have considered biochemical alterations for revealing the periodontal inflammatory process around restored teeth (26, 27). The relationship between subgingival restorations and gingival inflammation has been generally evaluated by the clinical status of gingival (28, 29). As a diagnostic method, biochemical analyses of gingival/periodontal reactions may be more sensitive than clinical examination, particularly for considering the early signs of inflammation. Currently, there are insufficient data on the interaction between restorative materials and gingival/periodontal reactions with regard to their effects on neurogenic inflammation.
Therefore, this study aimed to evaluate the unique effects of different restorative materials on periodontal neurogenic inflammation by evaluating local neuropeptide production in gingival crevicular fluid secondary to restorative dental treatment.
Materials and Methods
Study Population
Male patients ≥35 years old referred for restorative dental treatment were selected for the study population. The selection criteria at baseline were (i) no systemic problems and not having undergone any type or course of drug usage; (ii) having 1 molar tooth suitable for metal-ceramic crown restoration, 2 premolar teeth with mesio-occlusal or disto-occlusal caries suitable for composite and amalgam restorations and 1 tooth without dental caries or any endodontic problem; (iii) not to be in contact with each other; and (iv) not having any periodontitis or periodontal destruction in those teeth. The study protocol was in accordance with the Helsinki Declaration (1975, revised in 2002), and it was approved by the relevant human ethics committee.
Clinical Procedures and Group Characterization
Patients who met the selection criteria received phase I periodontal treatment for 4 weeks and underwent oral hygiene reinforcement for 4 weeks. At the end of this procedure, the gingival/periodontal conditions of all patients were re-examined by Silness-Löe Plaque Index (PI) (30), Löe-Silness Gingival Index (GI) (31) and probing pocket depth (PPD). PI, GI and PPD measurements were performed at 6 sites (mesiobuccal, midbuccal and distobuccal/lingual sites) per tooth in each patient by a calibrated investigator. To prevent or minimize the effects of plaque-induced reactions, the participant patients were included in the study when their full-mouth and relevant teeth PI and GI scores were <1 and their full-mouth and relevant PPD values were <3 mm. Three teeth to receive the restorations and 1 healthy tooth were enrolled for the study in each patient.
The study groups were constituted by split-mouth randomization regarding the tooth and restoration surfaces that contacted gingiva in each patient. Thus, 7 groups were included in the study: 1 ceramic surface of a metal-ceramic crown (ceramic group), its opposite metal surface (metal group), 1 composite surface (composite group), its nonrestored opposite enamel surface (opposite-composite group), 1 amalgam surface (amalgam group) and its nonrestored opposite enamel surface (opposite-amalgam group) and 1 nonrestored enamel surface (enamel group). The sample sizes of the groups were determined in accordance with the 5% significance and 90% power levels.
Afterwards, 3 teeth in each patient were treated with the planned restorative materials. For the metal-ceramic crowns, all teeth were prepared with diamond burs using a high-speed hand piece under water coolant, and preparations were ended as knife-edge at the gingival margin (Fig. 1). Metal framework adjustments of these crowns were made 1 day later, and the final metal-ceramic crowns were cemented with polycarboxylate cement 2 days after the adjustment of metal frameworks. Feldspathic ceramic material (VMK 95; Vita Zahn Fabric, Bed Sakingen, Germany) and metal-alloy (Wiron 99; Bego, Bremen, Germany) were used in the metal-ceramic crown restorations. Amalgam and composite treatments were performed on the day of metal-ceramic crown cementation. Mesio-occlusal or disto-occlusal cavities were prepared with diamond burs using a high-speed hand piece under water coolant. Cavity isolation was achieved by cotton rolls and saliva ejector, and then a retraction cord was placed into the gingival sulcus to avoid bleeding in the restoration area, and the cavities were filled with amalgam (Filtek Z250; 3M ESPE, St. Paul, MN, USA) (Fig. 2) or composite (Filtek Z250; 3M ESPE, St. Paul, MN, USA) (Fig. 2) materials. The dental restorations were done by 2 investigators.

Radiograph of crown restoration (tooth no. 16) of a patient.
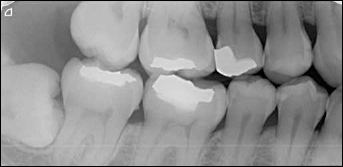
Radiograph of amalgam (tooth no. 15) and composite restoration (tooth no. 44).
Following restorative treatments, an extra oral hygiene reinforcement was performed for 4 weeks to maintain the periodontal health in each patient. Periodontal status of the group teeth was then recorded at the contact sites using the above-mentioned clinical parameters. Gingival crevicular fluid (GCF) samples were collected from the groups for the biochemical analyses (Fig. 3). Except for PI, all clinical parameters were measured after GCF sampling, to prevent possible alterations in GCF secondary to clinical examination. Alterations in the GCF volumes were also utilized in the clinical examination.
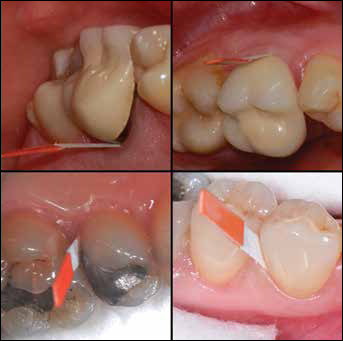
Collection of gingival crevicular fluid (GCF) samples from restorations.
GCF Sampling and Analysis
GCF levels of SP, NKA and CGRP were determined by enzyme-linked immunosorbent assay (ELISA) to determine the local neuropeptide production. Moreover, a proinflammatory cytokine analysis of GCF was also performed for interleukin-1α (IL-1α), interleukin-1β (IL-1β) and prostaglandin E2 (PGE2) to evaluate the inflammatory status of periodontium during data collection.
GCF samples were obtained from the gingival crevices of the contact sites determined in each group. These surfaces were dried gently with an air syringe for 5 seconds, the teeth were isolated by cotton rolls, and GCF was sampled with paper strips (Periopaper®; Ora Flow Inc., Amityville, NY, USA). Two paper strips were placed into each crevice at the same time and utilized per 1 tested tooth. They were inserted carefully until mild resistance was felt and left there for 30 seconds. All strips were placed at the same time to obtain the GCF samples simultaneously. Care was taken to prevent GCF stimulation due to any mechanical irritations. The absorbed GCF volume of each strip was determined by a volume quantifying device (Periotrons 8000; Pro Flow Inc., Amityville, NY, USA), and the strips were stored at −80°C until the laboratory procedures. One investigator collected the GCF samples.
GCF elution from the paper strips was performed by a modification of the protocol described by Curtis et al (32). Briefly, the strip pairs were put into 400-μL Eppendorf tubes containing 100 μL of 2% bovine serum albumin in phosphate-buffered saline (PBS), and then they were incubated for 60 minutes at 4°C. These tubes were placed in 1.5-mL microcentrifuge tubes, and centrifugation was done at 10,000 g for 5 minutes at 4°C, after creating a hole at the bottom of each Eppendorf tube, to provide GCF elution into each microcentrifuge tube. The procedure was repeated twice, 200-μL samples were collected and made up to 500 μL by addition of 300 μL of PBS for each sample. ELISA was performed to detect the neuropeptide and proinflammatory cytokine levels in these samples using the commercial ELISA kits for SP (Cayman Chemical Company, Ann Arbor, MI, USA), NKA (Phoenix Pharmaceuticals Inc., Burlingame, CA, USA), CGRP (Phoenix Pharmaceuticals Inc., Burlingame, CA, USA), IL-1α (RayBiotech Inc., Norcross, GA, USA), IL-1β (DIAsource ImmunoAssays, Nievelles, Belgium) and PGE2 (Cayman Chemical Company, Ann Arbor, MI, USA). These procedures were performed by 1 blinded investigator. The absorbance values were 400-420 nm for SP; 450 nm for NKA, CGRP, IL-1 α and IL-1 β; and 412 nm for PGE2.
Statistical Analysis
Statistical analysis was performed using a statistical software program (SPSS version 12.0; SPSS, Chicago, IL, USA). Normality of the data was evaluated by Shapiro-Wilk test, the differences were evaluated by Kruskal-Wallis test, and subsequent intergroup differences were analyzed by Mann-Whitney U test. Numerical values were given as medians (min-max).
Results
Fourteen patients with an age range of 35-45 years participated in the study, and thus each group included 14 sites in 14 patients (7 sites per mouth and a total of 98 sites). The clinical parameters and proinflammatory cytokine levels of GCF reflected periodontal health 4 weeks following restorations. There were no statistically significant differences among the PI, GI and PPD levels of the groups (p>0.05) (Tab. I). The proinflammatory cytokine analysis of GCF also demonstrated similar IL-1α, IL-1β and PGE2 levels between the study groups for the same period (p>0.05) (Tab. I). However, the GCF volumes were statistically significantly different among the study groups (p<0.05) (Tab. I). It was higher in the ceramic (p=0.001), metal (p=0.014), composite (p=0.000), opposite-composite (p=0.046), amalgam (p=0.000) and opposite-amalgam (p=0.009) groups than in the enamel group.
COMPARISON OF PI, GI, PPD, GCF VOLUME AND IL-α, IL-1β, PGE2 AMONG THE STUDY GROUPS
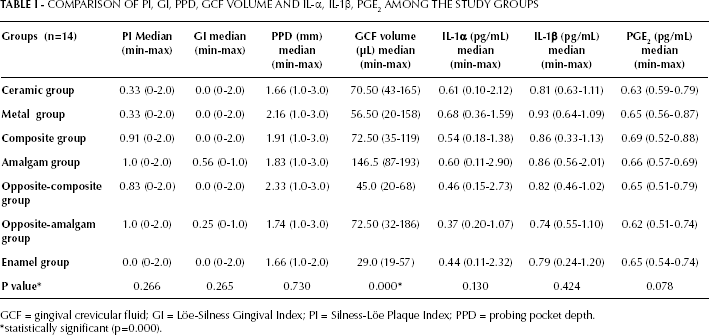
GCF = gingival crevicular fluid; GI = Löe-Silness Gingival Index; PI = Silness-Löe Plaque Index; PPD = probing pocket depth.
statistically significant (p=0.000).
Of the neuropeptides, SP and NKA demonstrated statistically significant differences among the study groups (p=0.000). SP levels of the ceramic, amalgam and composite groups were higher than that of the enamel group (p<0.05) (Fig. 4). SP was also higher in the composite group than in the opposite-composite group, and in the amalgam group than in the opposite-amalgam group (p<0.05) (Fig. 4). Similar SP levels were noted between the enamel and metal groups and between the opposite-composite and opposite-amalgam groups (p>0.05) (Fig. 4).
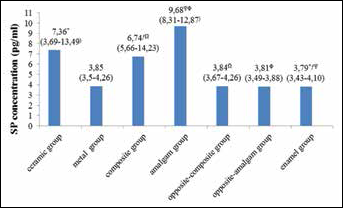
Intergroup differences for substance P (SP) between the restoration and enamel sites. *, ƒ, Ω, Ψ, Φ: P=0.000 (Mann-Whitney U test).
NKA was higher in the ceramic, composite and amalgam groups than in the enamel group (p<0.05) (Fig. 5). NKA level of the composite group was higher than that of the opposite-composite group, and NKA level of the amalgam group was higher than that of the opposite-amalgam group (p<0.05) (Fig. 5). It was similar between the enamel and metal groups and between the opposite-composite and opposite-amalgam groups (p>0.05) (Fig. 5). CGRP levels were similar in all of the study groups (p>0.05) (Fig. 6).
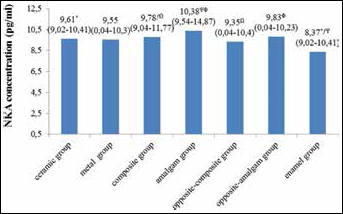
Inter-group differences for neurokinin A (NKA) between the restoration and enamel sites. *P=0.007, ƒP=0.001, ΩP=0.042, ΨP=0.000, ΦP=0.044 (Mann-Whitney U test).
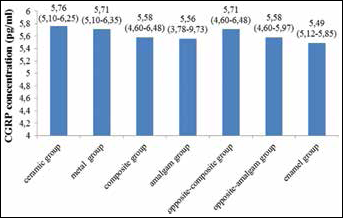
Comparison of calcitonin-gene related peptide (CGRP) levels among the study groups. P=0.213 (Kruskal-Wallis test).
Discussion
In the present study, periodontal responses to different types of restorative materials were investigated by evaluating local neuropeptide production in periodontium following dental restorations with these materials. The results revealed that GCF levels of some neuropeptides increased at the restoration sites, and they were higher than those of the nonrestored enamel sites, although there were no clinical and biochemical signs of gingival/periodontal inflammation in the meantime. To the authors’ knowledge, this study is one of the first investigations by means of such a finding for restorative materials.
We used retraction cord instead of dental dam in the present study. Dental dam utilization is the ideal to restore teeth, and it is particularly essential in investigating the quality of a restoration (i.e., microleakage studies). The important point is the properties of surface of the restoration and the relationship with gingiva in the present study.
Qualitative and quantitative analyses of GCF were utilized in addition to clinical examination for revealing the inflammatory status of the sites more sensitively. The proinflammatory cytokine analysis of GCF was similar in all groups and reflected a healthy gingival/periodontal condition – as was true for the clinical assessments. However, GCF volumes of the restoration sites were higher than those of the enamel sites. It is well known that increased GCF volume may be a pathobiological sign of the gingival/periodontal inflammatory process that is closely related with the diseased gingiva/periodontium (33, 34). But, some investigations have also reported that there may be an increase in the GCF volume of restored teeth compared with natural teeth, despite any differences in their gingival inflammatory status (23, 27). Such a finding, therefore, suggests that restorative materials may trigger GCF increases even in the absence of plaque-induced reactions, which may be an outcome of the neurogenic inflammatory process in periodontal tissues. This phenomenon may also be regarded as a subclinical susceptibility to pathological periodontal conditions.
Except for those of the metal group, GCF levels of SP and NKA were higher in all of the restoration groups those in the nonrestored enamel groups. Neuropeptides in general and tachykinins (SP and NKA) in particular are involved in the physiology of the inflammatory process (3, 7, 35). The possible roles of SP and NKA in the gingival inflammatory reactions have also been demonstrated previously (1, 3, 8, 34, 36). Therefore, it may be suggested that the ceramic, composite and amalgam materials may not be as inert as enamel and the metal-alloys for periodontal tissues, at least for the materials used in this study.
CGRP levels of all groups were found to be similar in the study. There are contradictory findings regarding the CGRP profile in the inflammatory process of periodontal tissues. Lundy et al (12) reported decreased CGRP levels in the GCF samples of gingivitis and periodontitis sites compared with the gingivally/periodontally healthy sites, while some authors demonstrated unchanged gingival CGRP production in periodontitis (36, 37). Dumitrescu et al (38) observed increased CGRP production on the first days of the disease, which decreased gradually by 10 days. Our results may be considered to be compatible with the findings of this study and may suggest that CGRP may not have an active role in the later phases of gingival inflammation.
In cell cultures, metal-alloys used for prosthetic restorations were reported to increase proinflammatory cytokines such as IL-6 and PGE2 (39, 40). Schmalz and Garhammer (41) have suggested that metal ions may have the potential to interfere with the cell metabolism, influencing the expression of substances such as cytokines which play an essential role in the inflammatory process. However, there are no former data about the correlation between metal prosthodontic materials and neurogenic inflammation or neuropeptide levels in periodontal tissues. The present study is the first investigation in this regard, and it has been demonstrated that prosthetic metals do not affect and/or trigger periodontal neuropeptide levels.
In the present study, SP and NKA were higher in the ceramic sites than in the enamel sites. Our understanding of the effects of ceramics on gingival tissues has generally been based on the comparison of GI scores in previous studies (28, 29, 42). In contrast to these studies, we selected teeth with similar GI scores and without clinical evidence of periodontal disease, to reveal the unique effects of different restorative materials on gingival neuropeptide levels. Thus, we aimed to investigate whether they have the potential to trigger neuropeptides in healthy gingiva which may cause susceptibility to gingival inflammatory reactions.
Data on the interaction between composite material and gingival conditions are controversial. Most of investigations have revealed that composite resins are not implicated in gingival inflammatory reactions such as gingivitis (17, 20, 21, 26, 43, 44). On the other hand, some studies have reported certain gingival inflammatory signs – i.e., GCF increases on the seventh and 14th days of experimental gingivitis (20, 45), gingival inflammation adjacent to the composite class V restorations (46) and increased bleeding on probing and greater probing depth adjacent to the composite restorations (47). The present study revealed increased SP and NKA levels in the composite sites compared with the enamel sites. This finding suggests that composite resin material may have the potential to induce inflammatory reactions due to its effects on neurogenic inflammation.
Evident inflammatory conditions have been reported around the gingival sites of amalgam restorations after 3-12 months even with effective plaque control regimens (22, 48). Gomes et al (19), in their histological dog study, found more inflammatory infiltration in the gingival crevices adjacent to amalgam and composite restorations. Again, amalgam was suggested to be more potent for inflammatory infiltration compared with composite material following dental plaque accumulation (19). There were higher SP and NKA levels around the amalgam restorations of the present study, which was in agreement with these previous studies, supporting their findings of increased neuropeptides as the markers of neurogenic inflammation.
In conclusion, these study results suggest that ceramic, composite and amalgam materials may trigger local neuropeptide production in periodontium even in the absence of plaque-induced reactions. In this respect, they may also increase susceptibility to periodontal inflammatory reactions by stimulating periodontal neurogenic inflammation. Therefore, periodontal maintenance of restored teeth may be of unique clinical importance, at least for the present types of dental materials.