
Abstract
Background:
Bladder cancer (BC) represents the most common neoplasm of the urinary tract. Although cystoscopy and urine cytology represent the gold standard methods to monitor BC, both procedures have limitations. Therefore, the identification of reliable biomarkers for early and noninvasive detection of BC is urgently required.
Methods:
In this study, we analyzed nicotinamide N-methyltransferase (NNMT) expression in urine samples from 55 BC patients and 107 controls, using real-time polymerase chain reaction (PCR). Receiver operating characteristic (ROC) analysis was used to identify the best cutoff value to discriminate BC patients from healthy donors, and to evaluate the diagnostic accuracy of a urine-based NNMT test.
Results:
The results demonstrated that urinary NNMT expression was significantly (p<0.05) higher in BC patients. Moreover, a significant (p<0.05) inverse correlation was found between NNMT expression and histological grade. The ROC analysis revealed that a ΔCq of 13.3 was the best cutoff value, since it was associated with the highest combination of sensitivity and specificity. Moreover, the area under the curve (AUC) value was 0.913 (p<0.05), indicating the excellent diagnostic accuracy of a urine-based NNMT test.
Conclusions:
Our data indicate that NNMT is a promising biomarker that could be used to support the early and noninvasive diagnosis of BC.
Introduction
Among neoplasms of the urinary tract, bladder cancer (BC) is the most common and represents the main cause of morbidity and mortality. BC has the ninth highest incidence rate of cancers worldwide, with an estimated 386,000 newly diagnosed cases and 150,000 deaths in 2008 (1). Urothelial carcinoma (UC) is the prevalent histological type and represents more than 90% of all BCs, while approximately 5% are squamous cell carcinomas, less than 2% are adenocarcinomas and the remaining forms are other rare subtypes (2).
Among patients with newly diagnosed UC, around 80% have non-muscle-invasive BC (NMIBC), while 20% are diagnosed with muscle-invasive BC (MIBC). BC recurrence rate is the highest of any solid tumor; indeed, 60%-70% of patients with NMIBC suffer a relapse, and in 11% of these recurrences, the tumor progresses to a muscle-invasive form. Since MIBC is related to the presence of occult distant metastases in almost 50% of patients, this tumor form contributes to the vast majority of cancer-specific deaths (3).
Given the frequent recurrence of NMIBC and consequent cancer progression after transurethral resection, patients with bladder UC undergo periodic examinations, with the frequency of those examinations based on the risk factors linked to the disease. Currently, the combination of cystoscopy and urine cytology is considered the gold standard both for primary detection of BC and for patient follow-up. However, both procedures have drawbacks and limitations. Cystoscopy is an expensive and invasive procedure which may often lead to patient pain and discomfort. Conversely, although urine cytology is not invasive, it shows a variable sensitivity for detection of tumors, depending on their histological grading. In particular, it shows high sensitivity for high-grade tumors and low sensitivity for detecting well or moderately differentiated cancers. Therefore, more sensitive and noninvasive methods for BC detection are urgently required, and would be of great benefit to both patients and the health care system.
In recent years, great efforts have been made to identify reliable peripheral markers that are able to reflect changes in neoplastic tissue and may be used for early and noninvasive detection of bladder UC (4). Among the advanced technologies used for cancer biomarker discovery, polymerase chain reaction (PCR) represents a powerful tool, since it can be performed starting from a small amount of cellular material obtained from urine. Moreover, the detection method is accurate, quantitative and inexpensive (5). The possibility to perform a urine-based test would be helpful for the follow-up of patients with NMIBC, since it could significantly decrease the number of cystoscopies required, with an ensuing decrease of costs and patient discomfort (6).
In the present work, we focused on nicotinamide N-methyltransferase (NNMT), an enzyme that catalyzes the N-methylation of nicotinamide, pyridine and structurally related compounds, playing a pivotal role in the detoxification of xenobiotics (7). NNMT was found to be up-regulated in several neoplasms. In our previous studies, we reported NNMT up-regulation in renal cell carcinoma (RCC) (8), in oral squamous cell carcinoma (OSCC) (9-11), and in non-small cell lung cancer (NSCLC) (12).
NNMT overexpression in clear cell RCC (ccRCC) exhibited an inverse correlation with tumor size, supporting the hypothesis that this enzyme could participate in tumor growth (8). In OSCC, NNMT up-regulation was inversely correlated with pT, lymph node metastasis, pathological stage and histological grade, suggesting that the enzyme could be involved in tumor expansion and differentiation, and might represent a prognostic marker (9, 10). Furthermore, short hairpin RNA (shRNA)-mediated gene silencing of NNMT reduced both cell proliferation and anchorage independent cell growth of KB, PE/CA-PJ15 and A549 cancer cells, suggesting that the enzyme could play a key role in tumorigenicity and could be a potential molecular target for anticancer therapy (13-15).
In a recent report, we evaluated NNMT expression in tumor and nontumor tissue samples obtained from patients affected by bladder UC, using quantitative real-time PCR (qPCR), Western blot analysis and catalytic activity assay. Moreover, NNMT messenger (RNA) (mRNA) and protein levels were measured in urine specimens from a small cohort of BC patients and healthy controls. The results revealed a marked NNMT up-regulation in bladder UC compared with normal-looking tissue. In addition, urinary NNMT expression levels were statistically significantly higher in patients with bladder UC than in control subjects (16).
The purpose of this study was to investigate urinary NNMT up-regulation in patients with bladder UC compared with controls, to evaluate whether urine NNMT expression level determination could be the basis for a reliable urine-based test for early and noninvasive diagnosis of BC. Therefore, NNMT mRNA levels were determined by qPCR in a large cohort of bladder UC patients and healthy participants. Subsequently, we also analyzed the relationship between tumor characteristics and urinary NNMT expression. Then, receiver operating characteristic (ROC) analysis was used to identify the best cutoff value to discriminate bladder UC patients from healthy donors, and to estimate the diagnostic accuracy of the urine-based NNMT test.
Methods
Patients and urine sample collection
Spontaneously voided urine samples were collected from 55 patients with bladder UC, before endoscopic treatment with transurethral resection, at the Urology Section of the Department of Clinical Sciences (Polytechnic University of Marche, Ancona, Italy), between January 2012 and July 2014, and from 107 age- and sex-matched healthy volunteers. The study was conducted according to the Declaration of Helsinki and all patients provided informed consent. The 2010 TNM classification system was used to assign the pathological stage to the tumors. Both the 1973 and 2004 WHO classifications were used to assign tumor grade. Table I lists the characteristics of the 55 patients.
Bladder UC patients and clinicopathological findings
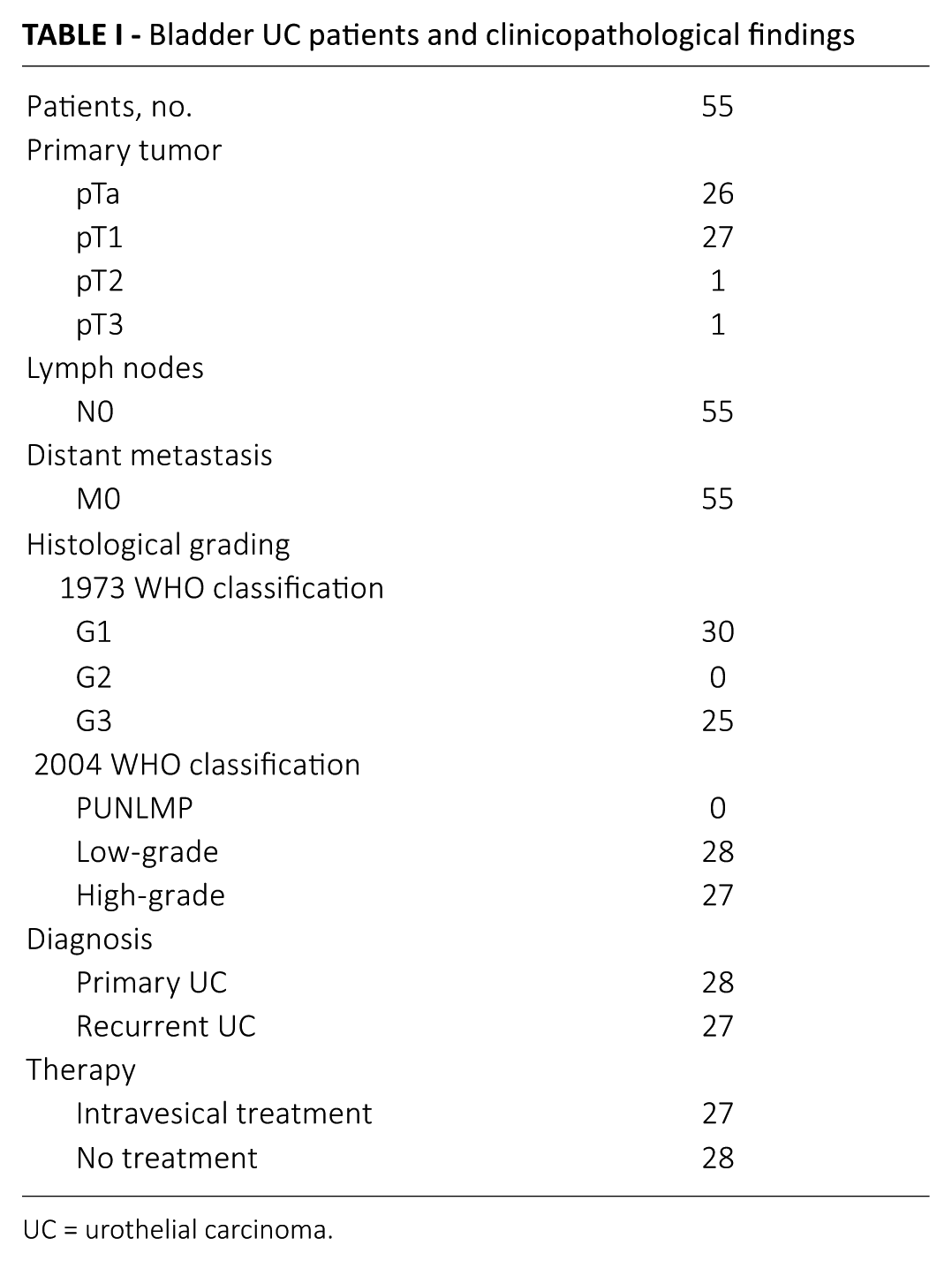
UC = urothelial carcinoma.
Urine samples (50-100 mL) were centrifuged at 1,200g for 15 minutes at 4°C to collect exfoliated cells. The cell pellet obtained from the urine was used for RNA isolation, cDNA synthesis and subsequent qPCR analysis.
RNA extraction and cDNA synthesis
The RNeasy Micro Kit (Qiagen, Hilden, Germany) was used to purify total RNA from exfoliated urinary cells, according to the manufacturer’s instructions. M-MLV reverse transcriptase (Promega, Madison, WI, USA) was used to reverse transcribe RNA in a final volume of 25 μL for 60 minutes at 37°C.
Real-time quantitative PCR
To examine NNMT gene expression in pathological and control samples, qPCR analyses were performed using the CFX96 Real-Time PCR Detection System (Bio-Rad Laboratories, Hercules, CA, USA). The cDNA, produced as described in the above paragraph, was used as the template for qPCR. To avoid an amplification of contaminating genomic DNA in the cDNA preparation that could lead to false-positive results, all primers were designed to flank an intron. PCR efficiency was tested for the 2 primer pairs and found to be close to 1. The primers used were (forward) 5’-GAATCAGGCTTCACCTCCAA-3’ and (reverse) 5’-TCACACCGTCTAGGCAGAAT-3’ for NNMT, and (forward) 5’-TCCTTCCTGGGCATGGAGT-3’ and (reverse) 5’- AGCACTGTGTTGGCGTACAG-3’ for β-actin.
qPCR was performed running 2 genes in duplicate for 40 cycles at 95°C for 30 seconds and 58°C for 30 seconds, using SsoFast EvaGreen Supermix (Bio-Rad Laboratories, Hercules, CA, USA). All samples were tested in triplicate, and β-actin was used as the reference gene for data normalization, to correct for variations in RNA quality and quantity. We monitored direct detection of PCR products by measuring the fluorescence produced by EvaGreen dye binding to double-strand DNA after every cycle. These measurements were then plotted against cycle numbers. The parameter quantification cycle (Cq) was defined as the cycle number at which the first detectable increase above the threshold in fluorescence was observed. The expression level of NNMT in urine samples from healthy controls and patients with bladder UC was expressed as ΔCq value, where ΔCq = Cq (NNMT) − Cq (β-actin). A small ΔCq represented a high NNMT expression level, while a large ΔCq value was attributable to a low expression level. Fold changes in relative gene expression were calculated by 2-ΔΔCq where ΔΔCq = (mean ΔCq of patients with bladder UC) – (mean ΔCq of healthy subjects). Mean ΔCq was calculated as the average of all ΔCq values within each group of samples (BC patients and controls).
Statistical analysis
Data were analyzed using IBM SPSS Statistics, version 19 (IBM Corp., New York, NY, USA). Significant differences between groups were determined using the Kruskal-Wallis and the Mann-Whitney U-test. Correlations between variables were assessed by Spearman test. A p value <0.05 was considered as statistically significant.
ROC analysis was used to evaluate the clinical performance of a urine-based NNMT test, in terms of diagnostic accuracy. Diagnostic accuracy measures the capacity of the test to discriminate between bladder UC patients and healthy individuals. The ROC analysis was carried out to identify the sensitivity and the specificity associated with different ΔCq values and to determine the best discriminatory cutoff point. The ROC curve is a graphical illustration of the entire spectrum of sensitivity and specificity pairs and is obtained by plotting sensitivity against 1–specificity. The area under the curve (AUC) is a measure of the discriminatory power of a urine-based NNMT test and ranges between 1 (perfect discrimination, 100% sensitivity and 100% specificity) and 0.5 (no discrimination, 50% sensitivity and 50% specificity). The best ΔCq cutoff value to distinguish patients with bladder UC from healthy controls was assessed as the maximum sum of sensitivity and specificity.
Results
Analysis of urinary NNMT by quantitative real-time PCR
qPCR was used to quantitatively evaluate NNMT expression in spontaneously voided urine samples from 55 patients with bladder UC and 107 healthy volunteers. Differential gene expression measurements revealed a statistically significant (p<0.0001) up-regulation of urinary NNMT (9.59-fold increase) in BC patients compared with healthy controls (Fig. 1).
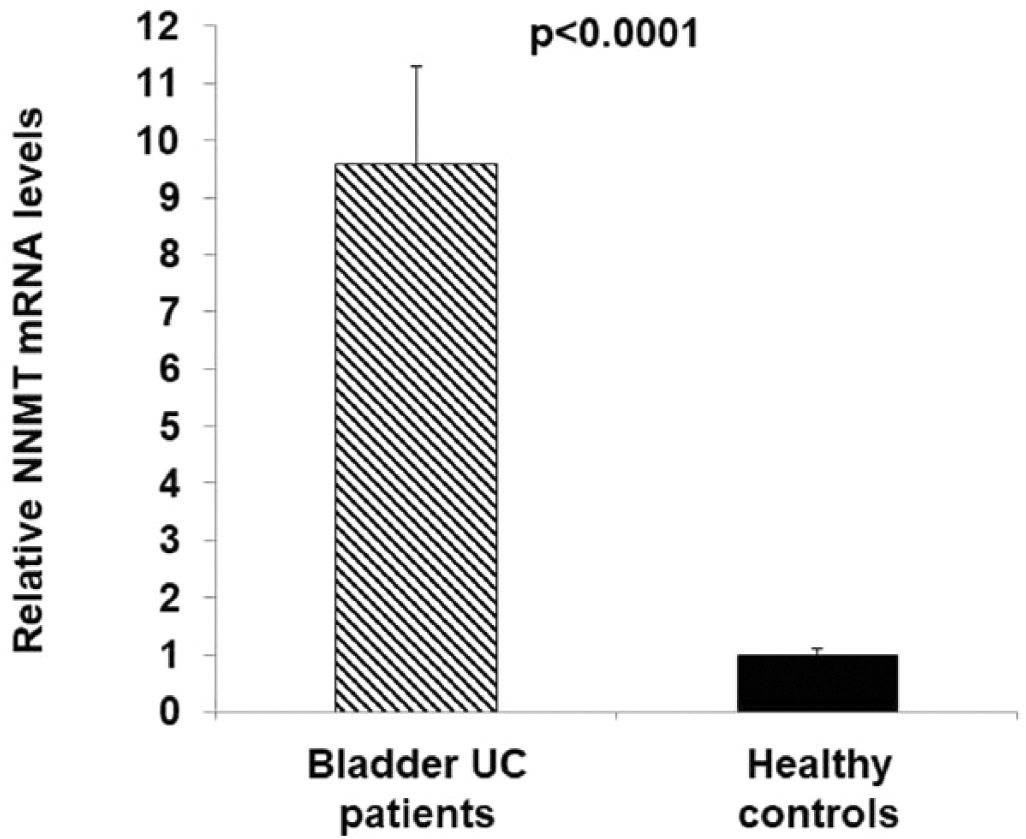
Quantitative real-time PCR analysis of nicotinamide N-methyltransferase (NNMT). NNMT expression levels were determined in urinary samples from 55 patients with bladder urothelial carcinoma (UC) and 107 healthy participants, as described in “Materials and methods.” All values are expressed as means ± standard deviation.
Urinary NNMT expression levels and clinicopathological parameters
First, we analyzed the relationship between NNMT expre- ssion and clinicodemographic data of healthy controls. In particular, we considered smoking habits, exposure to BC environmental factors, age, sex, other urological diseases, systemic morbidities and the use of medications. The results showed that there were no significant correlations between ΔCq values and age (p = 0.329), sex (p = 0.352), smoking (p = 0.237), environmental risk factors (p = 0.896), benign prostatic hyperplasia (p = 0.924), systemic diseases (p = 0.276) or medications (p = 0.234).
Subsequently, we explored the link between tumor factors and ΔCq values of patients with bladder UC. The clinicopathological parameters analyzed in this work were sex, age, histological grade and pT. In addition, we distinguished between patients who received intravesical treatment (mitomycin, epirubicin and bacillus Calmette-Guérin) and untreated patients, and between primary and recurrent tumors. Statistical analysis revealed that there was no statistically significant correlation between NNMT expression level and sex (p = 0.893), age (p = 0.866) or pT (p = 0.579). Moreover, no significant difference in NNMT expression was found between untreated and previously treated patients (p = 0.883), and between primary and recurrent UC (p = 0.842). Interestingly, a statistically significant (p<0.05) inverse correlation was found between NNMT expression and histological grade, either assigned with the 1973 (Fig. 2A) or the 2004 (Fig. 2B) WHO classifications.
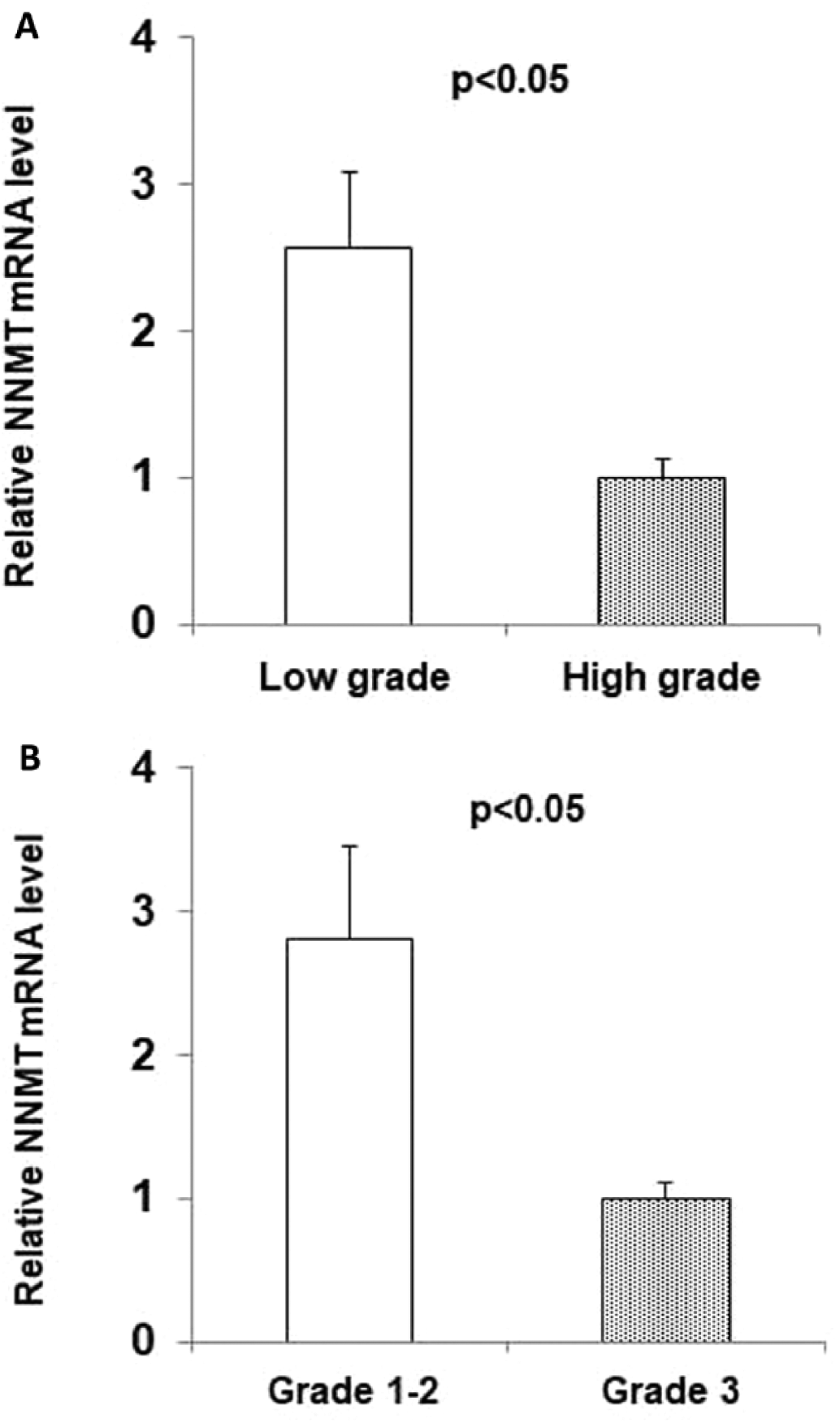
Correlation between nicotinamide N-methyltransferase (NNMT) expression level and histological grade. A statistically significant inverse correlation was found between NNMT expression and histological grade assigned according to either the 1973 (
Statistical evaluation of diagnostic performance
ROC analysis was carried out to determine the diagnostic accuracy of a urine-based NNMT test and to identify the best cutoff value to discriminate bladder UC patients from healthy participants.
The ROC curve showed the relationship between specificity and sensitivity of urinary NNMT measurements for the detection of patients with bladder UC. The ROC plot was drawn with data obtained from 55 patients and 107 controls, and the diagnostic accuracy of the test was expressed as the AUC. The AUC was 0.913 (Fig. 3), and the best ΔCq cutoff value was 13.3, since it was associated with the highest combination of sensitivity (84%) and specificity (84%) (p<0.0001). Sensitivity decreased as specificity increased, with every increasing cutoff value (Tab. II).
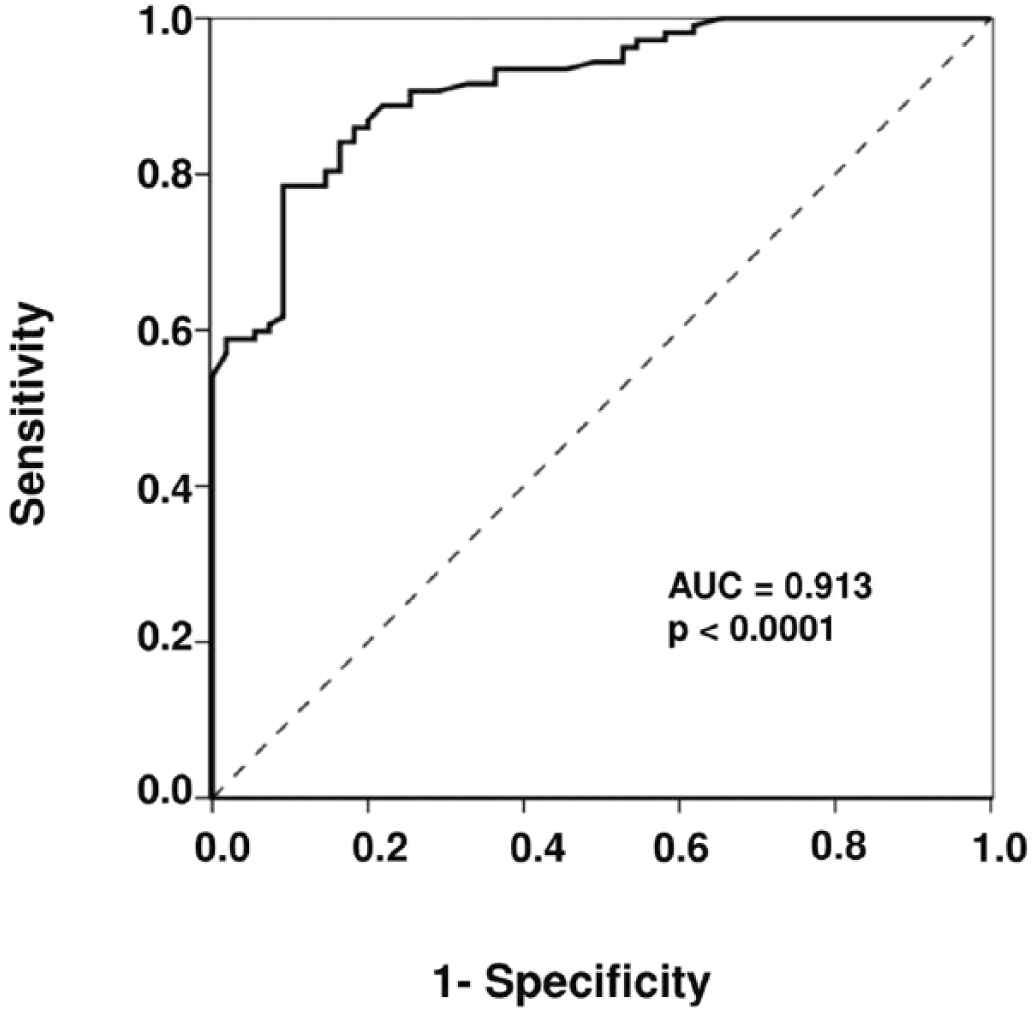
Receiver operating characteristic (ROC) curve of nicotinamide N-methyltransferase (NNMT) as urinary biomarker for detection of bladder urothelial carcinoma. The ROC analysis was performed to evaluate the diagnostic accuracy of a urine-based NNMT test. The ROC curve was obtained by plotting the sensitivity against 1-specificity at different cutoff values. The clinical performance of the test was measured by the area under the curve (AUC) value.
Sensitivity and specificity of urinary NNMT for detecting bladder UC
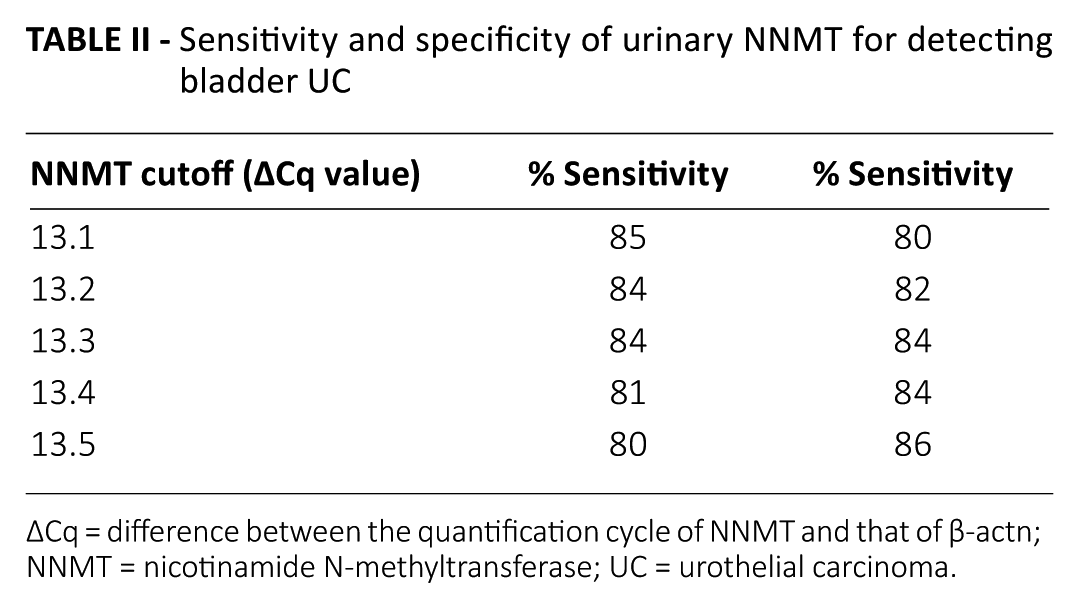
ΔCq = difference between the quantification cycle of NNMT and that of β-actn; NNMT = nicotinamide N-methyltransferase; UC = urothelial carcinoma.
Discussion
Although significant advances have been made in the discovery of the molecular mechanisms underlying bladder carcinogenesis, the management of UC patients remains a clinical challenge and represents an important economic problem for health care systems (17). Since superficial BC displays a very high recurrence rate, patients undergo periodic invasive and expensive cystoscopies. Due to the high expenses resulting from the surveillance and follow-up of NMIBC patients, BC is considered to be the most expensive tumor to treat (18).
As already reported, BC diagnosis and surveillance is mainly based on cystoscopy and urine cytology. However, both methods have significant limitations, since urine cytology has a low sensitivity for low-grade tumors, while cystoscopy is uncomfortable for patients. To address these important issues, new diagnostic tools have been investigated, either to reduce the number of cystoscopies needed or to increase the sensitivity of BC detection. On one side, important advances have been carried out concerning imaging technology. Fluorescence cystoscopy has been shown to augment detection levels for papillary and flat lesions, thus improving the completion of bladder resection, compared with the standard procedure in white light. Moreover, narrow-band imaging cystoscopy may increase the sensitivity of the standard endoscopic procedure by increasing the contrast between abnormal lesions and normal bladder tissue (19, 20). On the other side, in the last decade, intensive research has been focused on urine-based biomarkers, aiming to identify molecules that could have a potential for an early and noninvasive diagnosis of BC.
To date, several commercially available tests, based on the assessment of proteins detectable in urine, can be used to support standard procedures concerning both diagnosis and follow-up of BC. A laboratory-based microplate enzyme immunoassay is used to detect urine levels of nuclear matrix protein 22 (NMP22). NMP22 is overexpressed in malignant urothelial cells compared with their normal counterparts. On apoptotic stimulus, this protein is released into urine, and patients with BC display high concentrations of NMP22. Similarly, the BLCA-4 assay has been set up to evaluate nuclear matrix protein BLCA-4, which is up-regulated in urine of BC patients. BTA assays (BTA stat and BTA TRACK) are currently used for detecting UC associated with the release of basement membrane fragments into urine. Both tests have been developed to detect human complement factor H-related protein (hCFHrp) and complement factor H. Cytokeratin fragments in urine are assayed by UBC (cytokeratin 8 and 18 fragments) and CYFRA 21-1 (cytokeratin 19 fragments) tests.
Furthermore, a dot-blot assay has been developed to evaluate urine amounts of the inhibitor of apoptosis survivin, which is overexpressed in BC (21). However, despite their US Food and Drug Administration (FDA) approval, none of these tests has been included in clinical guidelines, since they have not achieved acceptance as standard diagnostic procedures.
In this work, qPCR was used to analyze the expression levels of NNMT in exfoliated cells collected from urinary samples obtained from patients with BC and healthy donors, to investigate the potential role of the enzyme for early and noninvasive diagnosis of this neoplasm. The results showed that NNMT expression was significantly higher in urines from patients with BC compared with those of controls. Moreover, statistical analyses revealed an inverse correlation between tumor enzyme levels and histological grade, and demonstrated the excellent diagnostic accuracy of a potential urine-based NNMT test.
NNMT catalyzes the N-methylation of nicotinamide, pyridine and analogs, using S-adenosyl-L-methionine as methyl donor (7). NNMT is mainly expressed in the liver where it plays a leading role among xenobiotic/drug-metabolizing enzymes (22). NNMT overexpression has been detected in many neoplasms, such as glioblastoma multiforme (23), gastric cancer (24), papillary thyroid cancer (25), RCC (8), OSCC (9-11) and pancreatic (26), bladder (16) and lung (12) cancers. Among nonneoplastic disorders, NNMT was found to be up-regulated in Parkinson’s disease (27), chronic obstructive pulmonary disease (28) and atherosclerosis (29).
Although NNMT overexpression has been reported in several pathological disorders, few studies have explored the implications of alterations in enzyme expression associated with disease, and the involvement of NNMT in cancer cell metabolism remains partly undisclosed. Kim et al explored the role of the enzyme in skeletal myoblast cultures and found that NNMT overexpression triggered a significant increase in cell proliferation and migration, and reduced cell death induced by reactive oxygen species exposure. Therefore, NNMT up-regulation, leading to increased myogenesis and antioxidant defenses, may represent a strategy to react to oxidative stress (30). NNMT knockdown in a human BC cell line was associated with significant reduction of cell migration, thus playing a key role in cancer invasion and metastasis (31). Since NNMT up-regulation has been reported to be associated with a high invasiveness in ccRCC cell lines, Tang et al investigated the role of the enzyme in cellular invasion, and found that NNMT knockdown suppressed the invasive capacity of ccRCC cells, while its overexpression led to increased invasion of HEK293 cells. Moreover, NNMT down-regulation efficiently suppressed metastasis formation and tumor growth of ccRCC cells in vivo (32). In SH-SY5Y, a tumor-derived human dopaminergic neuroblastoma cell line with no endogenous NNMT expression, both NNMT overexpression and N1-methylnicotinamide treatment significantly reduced cell death, increased intracellular ATP content, ATP/ADP ratio and Complex I activity, and protected cells from the toxicity of the Complex I inhibitors 1-methyl-4-phenylpyridinium ion (MPP+) and rotenone (33). A recent study showed that NNMT down-regulation significantly decreased cell growth in vitro, inhibited tumorigenicity in vivo and induced apoptosis in Bcap-37 and MDA-MB-231 human breast cancer cell lines. Interestingly, the opposite effect was observed by overexpressing NNMT in MCF-7 and SK-BR-3 breast cancer cell lines which do not possess constitutive NNMT expression (34). In our recent paper, we demonstrated that NNMT knockdown in PE/CA-PJ15 human oral cancer cells led to a significant decrease of tumorigenicity, both in vitro and in vivo (14).
NNMT catalyzes the formation of N1-methylnicotinamide that is predominantly excreted into urine and partly enzymatically converted to N1-methyl-2-pyridone-5-carboxamide and N1-methyl-4-pyridone-5-carboxamide, which are also excreted into urine. Therefore, N-methylation represents a metabolic pathway for nicotinamide excretion and plays a fundamental role in regulating the intracellular levels of this compound. In this regard, NNMT participates in nicotinamide homeostasis, modulating its excretion after N-methylation, and its overexpression may affect all essential events in which nicotinamide takes part. Moreover, nicotinamide is a precursor of β-nicotinamide adenine dinucleotide (NAD), which takes part in several biological processes that affect energy cycling and cellular metabolism. Nicotinamide is a strong inhibitor of enzymes such as histone deacetylases (sirtuins), implicated in mediating gene silencing, longevity and genome stability, and poly(ADP-ribose) polymerases (PARPs), which are involved in DNA damage response (35). NNMT overexpression was found to be associated with enhanced radiation resistance of a tumorigenic clone of retroviral immortalized human mesenchymal stem cells. In light of the above considerations, the absence of PARP inhibition caused by nicotinamide, which is depleted as a consequence of NNMT catalytic activity, may be responsible for elevated radiation resistance (36). In chronic lymphocytic leukemia cells, the deacetylating activity of endogenous SIRT1 is blocked by nicotinamide treatment, causing an inhibition of cell proliferation and the activation of apoptosis. Furthermore, the effects of the DNA damaging agent etoposide, which operates through a p53-mediated apoptotic pathway, are enhanced by exposure to nicotinamide. In this regard, enzyme activity of NNMT, decreasing nicotinamide intracellular concentrations, could play a key role in both tumor growth and chemoresistance (37).
NNMT activity may also be involved in the regulation of N1-methylnicotinamide endogenous levels. This compound was found to have antithrombotic (38), vasoprotective (39), gastroprotective (40), antiinflammatory (41) and neuroprotective (42) effects. It would be interesting to speculate whether N1-methylnicotinamide is able to exert a cytoprotective effect neutralizing anticancer drugs in tumor cells. From this perspective, the evident NNMT overexpression observed in tumors, which leads to high intracellular levels of N1-methylnicotinamide, could represent an adaptive advantage for cancer cells.
To our knowledge, this is the first study to evaluate the diagnostic accuracy of a urine test based on the expression analysis of NNMT mRNA levels in exfoliated cells from urine samples obtained from a large cohort of bladder UC patients and healthy individuals. The results confirmed urinary NNMT overexpression in BC and showed a significant inverse correlation between enzyme expression levels and histological grade. Most importantly, ROC analysis demonstrated that the best ΔCq cutoff value was associated with elevated levels of sensitivity and specificity, illustrating the high discriminatory power of a urine-based NNMT test to distinguish between BC patients and controls. These data indicate that NNMT is a promising biomarker that could be used to support the early and noninvasive diagnosis of BC.
However, to assess whether a NNMT-based urine test is applicable for BC detection, additional aspects should be explored. First, patients affected with urinary tract diseases different from BC (e.g., cystitis) should be included in the control group, to evaluate the effect of both inflammation and hematuria on NNMT expression. Second, although the results obtained from ROC analyses were statistically significant, the established cutoff value needs to be validated in a different and larger cohort of pathological samples prior to future clinical applications. Furthermore, it should be interesting to perform both urine cytology and NNMT expression measurement in the same cohort of BC patients, to compare the diagnostic value of both evaluation methods. The potential development of a urine-based test would lead to an opportunity for long-term follow-up, creating the prospect of verifying the existence of a link between NNMT expression levels and response to treatment and/or disease outcome, thus establishing its role as a prognostic marker.
Footnotes
Acknowledgements
We would like to offer our sincere thanks to Giacomo Regnicolo, past president of Infinito Vita SMS, for his special support and encouragement at all stages of the project.
We are indebted to Barbara Taglienti and Roberta Di Foglio, and to Croce Gialla of Recanati and Croce Verde of Macerata for their help in collecting urine samples.
This paper is dedicated to the memory of my husband, Andrea L. Tranquilli.
Monica Emanuelli
Abbreviations
AUC Area under the curve
BC Bladder cancer
ccRCC Clear cell ccRCC
MIBC Muscle-invasive bladder cancer
MPP+ 1-methyl-4-phenylpyridinium ion
NAD β-nicotinamide adenine dinucleotide
NMIBC Non-muscle-invasive bladder cancer
NNMT Nicotinamide N-methyltransferase
NSCLC Non-small cell lung cancer
OSCC Oral squamous cell carcinoma
PARPs Poly(ADP-ribose) polymerases
PCR Polymerase chain reaction
qPCR Quantitative real-time PCR
RCC Renal cell carcinoma
ROC Receiver operating characteristic
UC Urothelial carcinoma
Disclosures
Financial support: This work was partially supported by Infinito Vita SMS (Recanati, Italy), and a fellowship (D.S.) was sponsored by the Fondazione Umberto Veronesi.
Conflict of interest: The authors declare they have no competing interests.