
Abstract
Background:
The objective of this study was to examine the prognostic significance of carbonic anhydrase IX (CAIX), an endogenous marker for tumor hypoxia; the cellular tumor antigen p53; and the apoptosis regulator Bcl-2, in triple-negative breast cancer (TNBC) patients.
Methods:
Immunohistochemically determined expression of CAIX, p53, Bcl-2 and proliferation factor Ki-67, analyzed in 64 paraffin-embedded TNBC tissue samples, was used to assess their relation to clinicopathological variables and prognostic implications for overall survival (OS).
Results:
Bcl-2 expression was negatively correlated with histological grade of tumor, while expression of p53 was positively correlated with the same clinical variable (p = 0.036 and p = 0.033, respectively). The p53 expression was also positively correlated with tumor size (p = 0.010). Survival analysis showed that patients with high Bcl-2 expression (above cutoff value determined by receiver operator characteristic [ROC] curve analysis) had shorter OS (p = 0.020). The same was observed for patients with tumors larger than 5 cm (p = 0.034) or positive lymph nodes (p = 0.004). Among all 3 examined markers, multivariate analysis showed that only Bcl-2 expression was a strong independent prognostic indicator for decreased OS (hazard ratio [HR] = 15.16, 95% confidence interval [95% CI], 2.881-79.727, p = 0.001).
Conclusions:
Elevated expression of Bcl-2 was an independent prognostic factor for poorer OS in TNBC and as such a significant marker for tumor aggressiveness.
Keywords
Introduction
Breast cancer is still the most commonly diagnosed cancer in women and the second leading cause of cancer death among women in more developed countries (1). Although the improvements in early detection and treatment strategies have resulted in decreased mortality, more reliable prognostic and predictive markers of breast cancer are still the most important goals of breast cancer research (2). Breast cancer is a heterogeneous disease, with a high degree of diversity between and within tumors as well as among cancer-bearing patients (3). Between 12% and 17% of all breast cancers are represented by so-called triple-negative breast cancer (TNBC), which is characterized by the lack of expression of estrogen, progesterone and human epidermal growth factor receptor 2 (HER2). It is among the most aggressive subtypes, with high rates of tumor recurrence and poor overall survival (OS) of patients (4). Nevertheless, TNBC is still poorly characterized molecularly and lacks definitive prognostic markers and selective targeted therapies (5).
A hypoxic microenvironment is considered to be a critical factor in solid tumor progression and metastasis (6). Complete absence of oxygen (anoxia) in most cells leads to a rapid cell cycle arrest, no matter at what stage the cells are in. In hypoxic conditions, for the purpose of DNA damage repair, the cells accumulate tumor suppressor protein p53 via hypoxia-inducible factor 1 (HIF-1). In the case of irreversible DNA damage, p53 accumulation leads to programmed cell death (apoptosis). Hypoxia also activates p53-independent mechanisms of apoptosis, including the activation of B-cell lymphoma 2 (Bcl-2) protein (7). Prolonged hypoxia can lead to cellular changes ultimately resulting in a more aggressive clinical phenotype and poor prognosis (8).
HIF-1A and other hypoxia-inducible genes, along with their downstream gene products such as vascular endothelial growth factor A (VEGF-A), are known for their ability to serve as prognostic indicators for breast cancer (9). One such downstream target of HIF-1A is carbonic anhydrase IX (CAIX), a zinc metalloenzyme involved in hydration of carbon dioxide to carbonic acid, which thus affects cell metabolism and pH regulation. Its expression often serves as an endogenous marker for tumor hypoxia, with various prognostic values in different breast cancer subtypes (10).
Tumor suppressor protein p53, “the guardian of the genome”, is inactivated in the majority of cancers, while in breast cancers p53 is mutated in almost 30% of cases, with an increased frequency in TNBCs (11). It was also shown that p53 status was a strong prognostic factor for decreased relapse-free survival and OS only in TNBC patients treated with adjuvant anthracycline-based chemotherapy, which could suggest a need for aggressive or alternative treatment (12).
Oncoprotein Bcl-2 is an important antiapoptotic protein and its carcinogenic potential has been demonstrated in lymphomas where Bcl-2 overexpression blocks apoptosis and cooperates with c-MYC in B-cell transformation (13). Opposite from what would be expected, increased Bcl-2 expression was shown to be an independent indicator of favorable prognosis and good outcome for all types of early-stage breast cancer (14). On the other hand, its decreased expression was a good predictive factor for better chemotherapy response in breast cancer patients (15).
Proliferation marker protein Ki-67 is present during all active phases of the cell cycle, and immunohistochemical assessment of its expression is commonly used to determine the growth fraction of a given neoplastic cell population (16). In addition, it can be used for breast cancer prognosis and is prediction of relative responsiveness or resistance to chemotherapy or endocrine therapy (17).
In our previous study we have shown that high expression of CAIX was a strong independent prognostic indicator for shorter OS and recurrence-free survival (RFS) for patients with invasive ductal breast carcinoma (18). The objective of this study was to examine the expression of the hypoxic marker CAIX relative to expressions of the apoptosis regulator Bcl-2, tumor suppressor protein p53 and proliferative index Ki-67, to examine the role of hypoxia in TNBC.
Methods
Study population
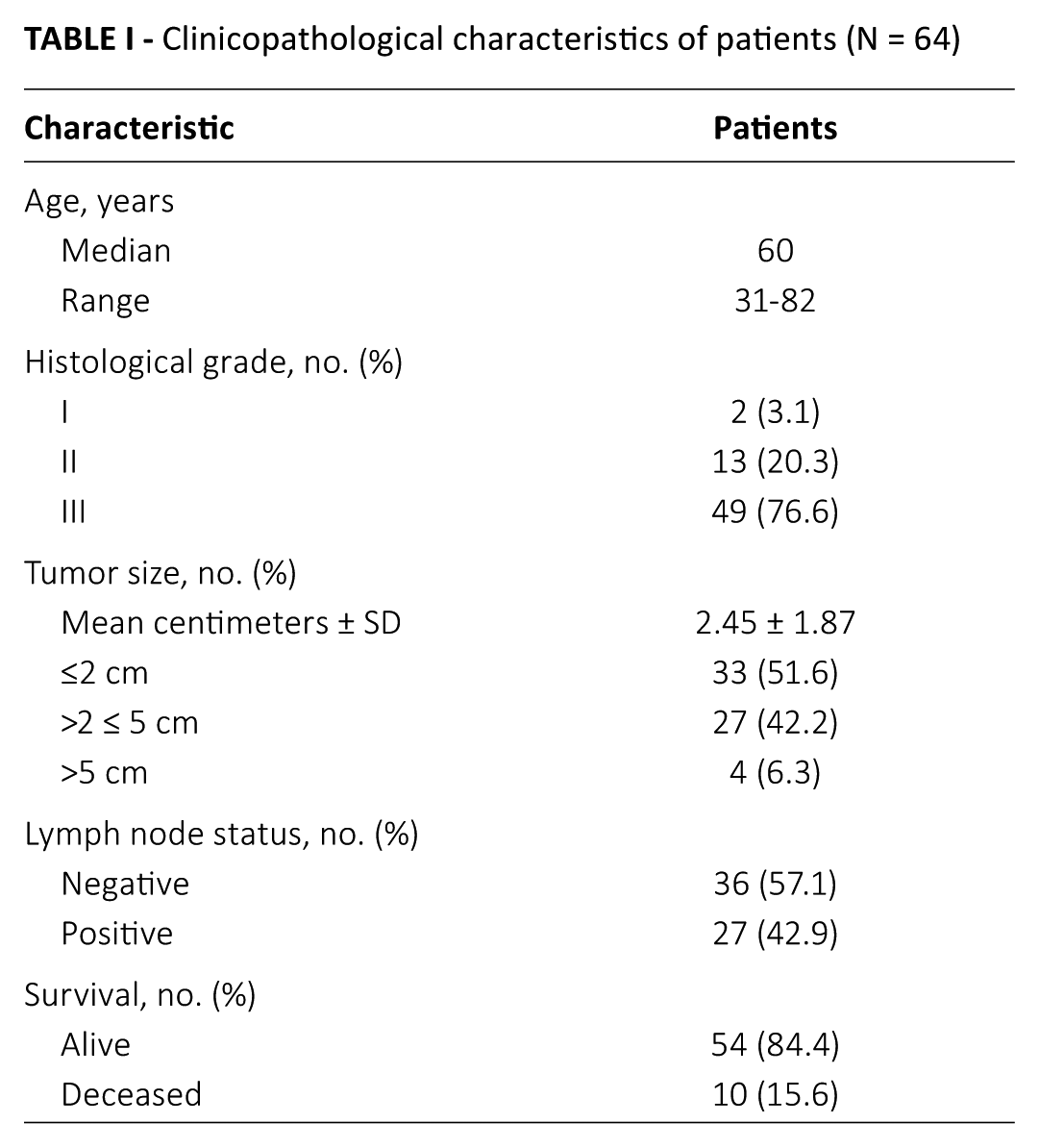
Sixty-four female patients with TNBC operated on at the University Hospital for Tumors, Zagreb, in the period from 2007 to 2011, were included in this study. Patients’ characteristics are listed in Table I. Their median age was 60 years (range 32-81 years). The median follow-up of patients at the time of analysis was 55.5 months (range 5-90 months). OS time was measured from the date of surgery to the time of death or last follow-up observation. All tumor samples were collected in accordance with the Declaration of Helsinki and following the ethical principles approved by the institutional ethical board of the Sestre Milosrdnice Clinical Hospital Center, Zagreb, with informed consent obtained from each patient.
Clinicopathological characteristics of patients (N = 64)
Tissue microarray preparation
Tissue microarrays (TMAs) were prepared using the Tissue-Tek Quick-Ray System (Sakura Finetek USA, Torrance, CA, USA). The system consists of a hollow tip and preformed recipient paraffin block with 60 gaps. In the areas of biopsies with tumor tissue, 3 cylinders 2 mm in diameter were drilled with the hollow tip and placed in a recipient paraffin block. Each completely filled recipient block was placed into a base mold and heated at 60°C for 30 minutes, with the addition of paraffin wax evenly inside the cartridge. Four paraffin sections 2- to 3-μm thick were cut per tumor sample, and each paraffin ribbon was stretched at 55°C in a water bath, placed on a glass microscope slide and dried at 55°C for 1 hour in an air incubator. Before immunohistochemical staining, sections were deparaffinized in xylene and decreasing concentrations of alcohol (100%, 95%, 70%), and rehydrated in distilled water. To reveal epitopes masked during the preparation, sections submerged in Target Retrieval Solution with Tris/EDTA buffer, pH 9.0 (Dako, Glostrup, Denmark) were heated at 97°C for 20 minutes in a water bath.
Immunohistochemical staining
Deparaffinized and unmasked sections of tumor tissues were treated with 3% hydrogen peroxide for 5 minutes to inhibit endogenous peroxidase. Tissue sections were rinsed with phosphate-buffered saline and incubated for 30 minutes with primary antibodies in specified dilutions (v/v): for cellular marker of hypoxia carbonic anhydrase IX (1:100; ab15086; Abcam, Cambridge, MA, USA), for marker of apoptosis Bcl-2 (1:100; M0887; Dako, Glostrup, Denmark), for cellular tumor antigen p53 (1:50; M7001; Dako, Glostrup, Denmark) and for proliferation factor Ki-67 (1:100; M7240; Dako, Glostrup, Denmark). The resulting antigen-antibody complex was treated with EnVision FLEX, High pH/HRP reagent (Dako, Glostrup, Denmark) for 30 minutes. The specific antigen-antibody reaction became visible after incubation with DAB+ chromogen (Dako, Glostrup, Denmark) for 10 minutes. Slides were counterstained with hematoxylin for 2 minutes. All staining steps were carried out in an automated Dako Autostainer machine (Dako, Glosrup, Denmark).
Quantification of immunohistochemical staining
Slides were evaluated by an experienced pathologist. Results of immunohistochemical analyzes were expressed by their immunoreactivity score (IS) presented as the product of staining intensity and the percentage of stained tumor cells (cytoplasm or nucleus). The staining intensity was determined as follows: no staining = 0, weak staining = 1, intermediate staining = 2, or heavy staining = 3. The cutoff values used to dichotomize the IS of each marker into 2 groups – low and high – were determined using receiver operator characteristic (ROC) curve analysis (19). Samples with more than 20% positively stained tumor cells on Ki-67 were considered to have a high expression level (20).
Statistical analysis
Pearson’s chi-square test was used to assess the association and distribution of categorical variables. OS curves were calculated with the Kaplan-Meier method and compared by the log-rank test. The Cox proportional hazards regression model with forward stepwise variable selection was used for multivariate analysis. A 2-tailed p value less than 0.05 was considered statistically significant. Statistical analyses were performed using MedCalc for Windows, version 14.8.1 (MedCalc Software, Mariakerke, Belgium).
Results
Levels of CAIX, Bcl-2, p53 and Ki-67 expression and their relation to clinicopathological variables
Expression of CAIX was membranous, Bcl-2 cytoplasmic, while p53 and Ki-67 showed nuclear staining in tumor cells (Fig. 1). Cutoff values for dichotomization of CAIX, Bcl-2 and p53 IS were 60, 180 and 270, respectively. Immunohistochemical staining showed high CAIX expression in 49/64 samples (77%), high Bcl-2 in 7/64 samples (11%), high p53 expression in 27/64 samples (42%) and high Ki-67 expression in 53/64 samples (83%) of TNBC.
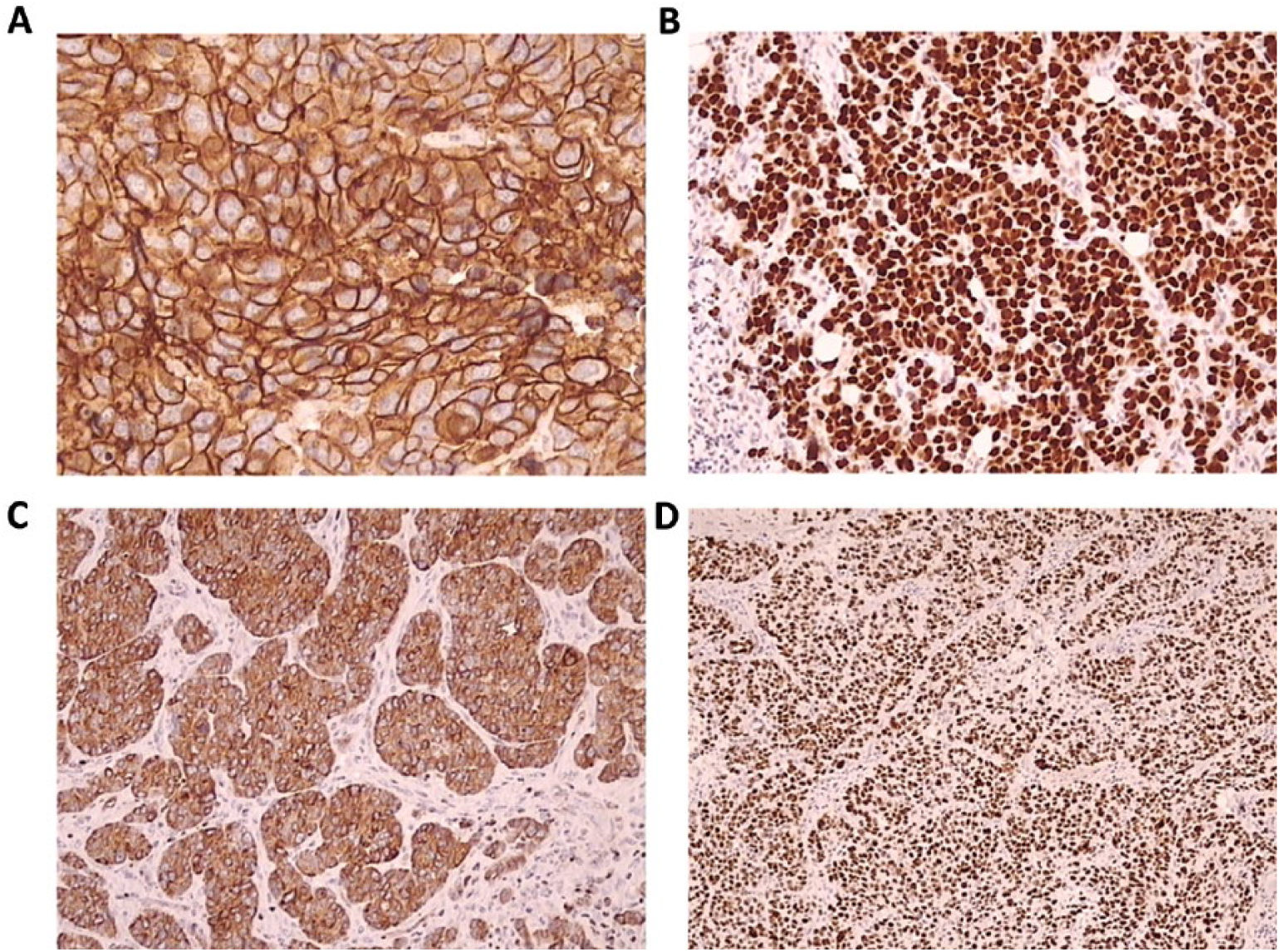
Representative photomicrographs depicting high immunohistochemical expression (brown) of examined markers in triple-negative breast cancer tissue. (
We analyzed the correlation of these 4 markers with pathological variables in TNBC patients (Tab. II) and found that Bcl-2 and p53 expressions were correlated with histological grade of tumor (p = 0.036 and p = 0.033, respectively). Low Bcl-2 expression was mostly observed in grade III tumor samples, which also showed high expression of p53. The p53 expression was also positively correlated with tumor size (p = 0.010). Expression of both CAIX and Ki-67 was not correlated with any of the clinicopathological characteristics of the TNBC patients examined. We also did not observe any correlation between markers’ expression levels (data not shown).
Levels of marker expression in relation to clinicopathological characteristics of patients
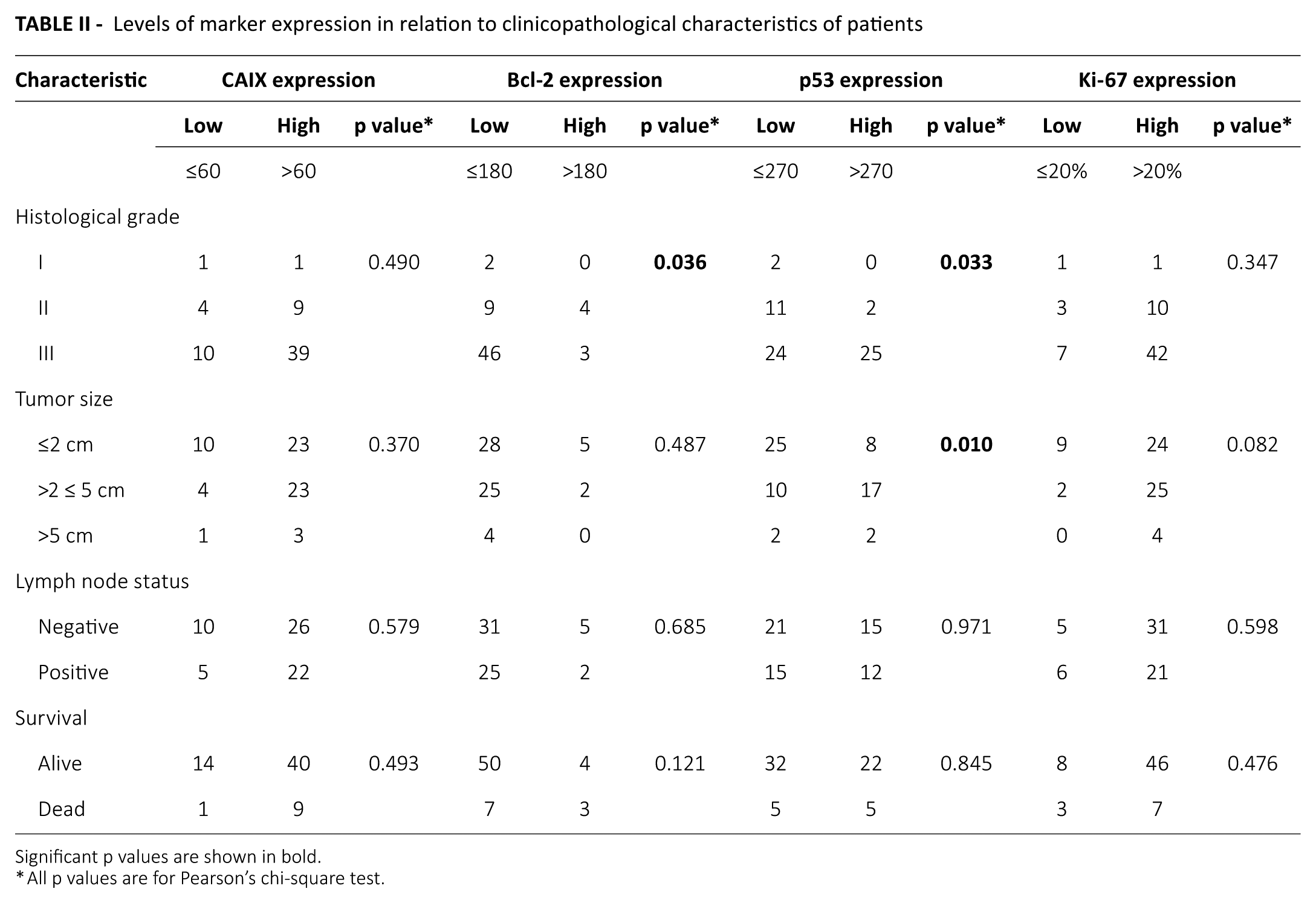
Significant p values are shown in bold.
All p values are for Pearson’s chi-square test.
Relationship of tumor marker expression and clinicopathological characteristics with survival
Ten patients (16%) died during follow-up period. The cause of death was primary tumor recurrence. To examine the importance of markers with regard to OS, survival curve analysis was performed. Kaplan-Meier plots showed that patients with high Bcl-2 expression had shorter OS (log-rank p = 0.020) (Fig. 2A). The same was observed for patients with tumor larger than 50 mm (p = 0.034) and for patients with positive lymph nodes (p = 0.004) (Fig. 2B and C). There was no significant correlation between expression of other examined tumor markers and patients’ survival (data not shown).
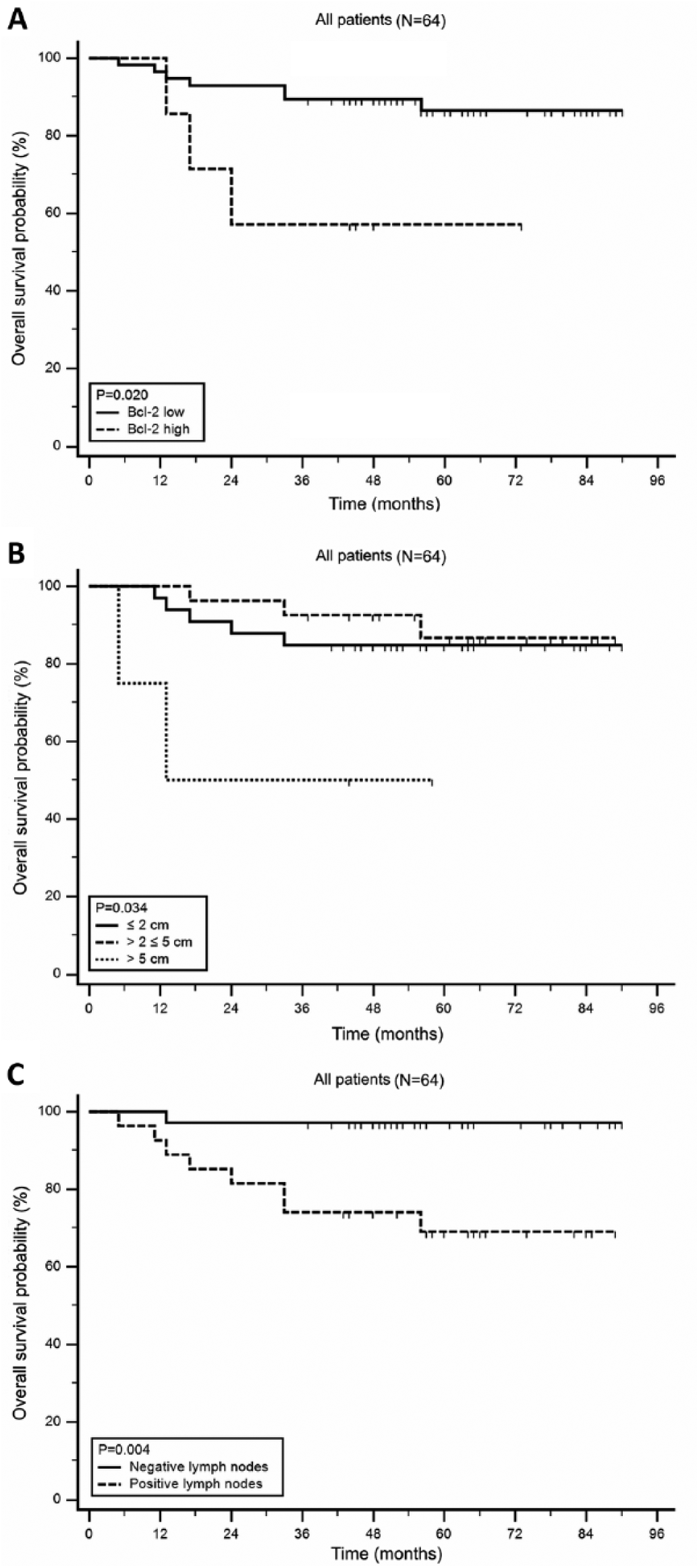
Kaplan-Meier survival curves illustrating overall survival (OS) for triple-negative breast cancer patients (N = 64). (
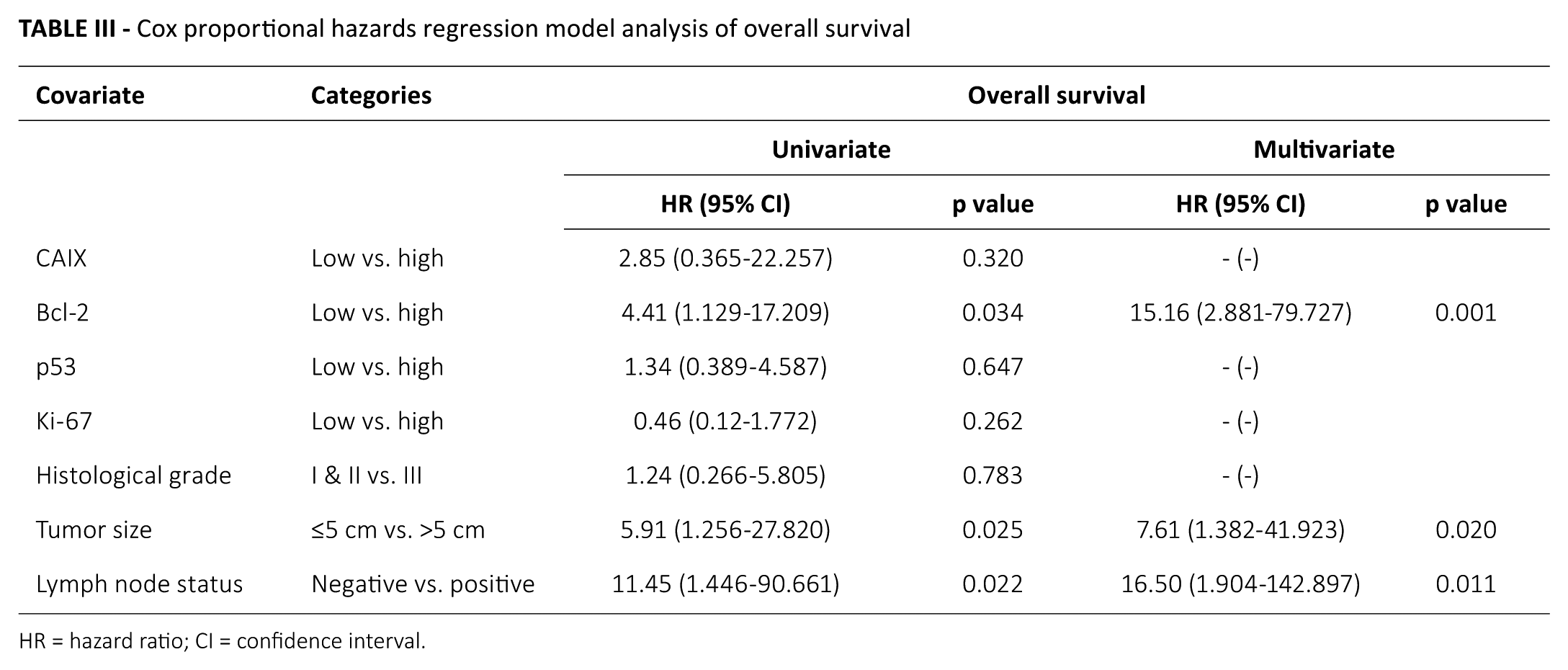
To examine the independent prognostic significance of clinicopathological variables and markers expression, multivariate analysis was performed. Only variables with significant (p<0.05) univariate impact were used in the multivariate analysis (Tab. III). Markers’ expression, histological grade, tumor size and lymph node status were used as binary categories. Multivariate analysis showed that high Bcl-2 expression (hazard ratio [HR] = 15.16, 95% confidence interval [95% CI], 2.881-79.727, p = 0.001), positive lymph node status (HR = 16.50, 95% CI, 1.904-142.897, p = 0.011) and tumor larger than 5 cm (HR = 7.61, 95% CI, 1.382-41.923, p = 0.020) were independent prognostic indicators for decreased OS for patients with TNBC.
Cox proportional hazards regression model analysis of overall survival
HR = hazard ratio; CI = confidence interval.
Discussion
TNBCs express heterogeneous clinical and molecular characteristics (4). Due to the lack of hormonal and HER2 receptor expression, TNBCs often do not respond to standard breast cancer treatments and have worse prognosis (21). Therefore, it is of great clinical importance to identify new molecular biomarkers which could be used for prognosis and for selecting appropriate therapeutic regimens (22). In this study, we examined the expression of a hypoxic marker, CAIX, in relation to expressions of an apoptosis regulator, Bcl-2; tumor suppressor protein, p53; and proliferative index, Ki-67, to clarify the role of hypoxia in TNBC.
It was previously shown that hypoxia could be specifically linked with triple-negative subtypes of breast cancer (23), so high expression of the endogenous tumor hypoxia marker CAIX, which was present in 77% of our samples, could verify this. Since tumor hypoxia can negatively influence treatment outcome, its targeting could be a potential therapeutic strategy for TNBCs (24). Although it has previously been shown that CAIX expression could also be associated with worse prognosis for TNBC patients (25, 26), our study did not repeat this finding.
The value of the apoptosis regulator Bcl-2 as a prognostic factor for TNBC seems to be ambiguous. As extensively reviewed by Bouchalova et al (27), most clinical studies have shown that increased expression of Bcl-2 is connected with better OS for TNBC. This “paradoxical” beneficial effect of an antiapoptotic protein could be explained by its nonapoptotic functions in cell cycle control or by its interactions with other members of the Bcl-2 family of apoptotic regulators, especially with proapoptotic proteins (28). Nevertheless, in our study we showed the opposite – name, that high Bcl-2 expression was significantly correlated with shorter OS (Fig. 2A). Even more, in multivariate analysis, together with 2 traditional prognostic factors in breast carcinoma – lymph node status and tumor size – high Bcl-2 expression was found to be an independent prognostic marker for decreased OS for patients with TNBC (Tab. III). The similar results have been published recently, where the authors postulated that Bcl-2 expression could be used as a selection criterion for anthracycline-based chemotherapy for patients with TNBC (29). The observation that Bcl-2 expression decreases with malignant progress, which can be represented by the higher histological tumor grade, has been previously made in invasive ductal breast carcinoma (30), as well as in ovarian tumors (31) and follicular lymphomas (32).
Positive immunohistochemical staining for p53 protein indicates gain of function of TP53 gene mutations that result in protein inactivity, increased stability and high expression levels of p53 protein (33). Our study showed that high expression of cellular tumor antigen p53 was present in 42% of our samples. This could be used for stratification of this heterogeneous subtype of breast cancers into subgroups according to prognosis and chemotherapeutic response (34). It was shown that p53 positivity in TNBC correlates with poor survival, worse response to therapy and is more common in younger patients (35, 36). Our study could not corroborate the usefulness of p53 expression as a prognostic biomarker for OS in TNBC patients. On the other hand, we showed that p53 expression was positively correlated with both tumor grade and size. The correlation between histological tumor grade and p53 expression has been previously observed in African American women with breast cancer (37), but not in patients with visceral metastasis breast cancer (38). Additionally, the correlation between tumor size and p53 expression was found in patients with invasive ductal carcinoma without axillary lymph node involvement (39), but again not in visceral metastasis breast cancer patients (38). It is proposed that p53 mutations occur more frequently in advanced stages of tumor development, when the tumor is bigger and less differentiated (11).
Immunostaining for nuclear protein Ki-67 is routinely used as a marker for dividing cells, and thus determined proliferating index is commonly used as a prognostic factor in cancer studies (16). About 83% of our samples had high proliferating index (>20% positively stained tumor cells on Ki-67), and it is generally considered that TNBC is associated with higher Ki-67 expression compared with non-TNBCs (40). In addition, Keam et al (40) also showed that high Ki-67 expression was significantly associated with poorer OS in TNBC patients. Our study did not confirm this finding, probably due to the smaller sample size and different cutoff point (20% vs. 10%).
As a conclusion, in our study, a high proportion of TNBC samples showed high expression of the hypoxic marker CAIX, as well as tumor suppressor protein p53 and proliferation index Ki-67. Increased expressions of CAIX, p53 and Ki-67 were not connected with decreased patient survival. However, patients with high tumor Bcl-2 expression had shorter OS, and expression of antiapoptotic protein Bcl-2 was an independent prognostic indicator for OS for patients with TNBC. With the cutoff value of Bcl-2 expression, we were able to distinguish TNBC patients with better or worse prognosis. For further characterization of this subgroup of TNBC, additional molecular biomarkers should be studied, such as BRCA1 and BRCA2 genes.
Footnotes
Disclosures
Financial support: This work was supported by a grant from the Ministry of Science, Education and Sports of the Republic of Croatia (grant no. 074-0982464-1187).
Conflict of interest: The authors declare they have no conflict of interest.
Meeting presentation: The results published in this paper were presented at the 11th Central European Oncology Congress (CEOC) in Opatija, Croatia, June 17-20, 2015, and the 10th European Breast Cancer Conference (EBCC-10) in Amsterdam, Netherlands, March 9-11, 2016.