
Abstract
Background
Colon cancer–associated transcript 2 (CCAT2) as a long noncoding RNA (IncRNA) is overexpressed and plays a significant prognostic role in patients with tumors. The present study aimed to comprehensively evaluate the clinical value of CCAT2 in the Chinese population, as a potential prognostic marker in multiple cancers.
Methods
A systematic search of eligible studies was conducted in the PubMed, Web of Science, Cochrane Library, Wanfang and the China National Knowledge Infrastructure databases as of March 31, 2017. Approximately 1,711 tumor patients from 16 eligible studies were selected. Analyses of the pooled data were performed, and the odds ratio (OR) or hazard ratio (HR) and the 95% confidence interval (95% CI) were calculated and summarized to evaluate the strength of this association using a fixed- or random-effects model.
Results
Overall analyses showed that increased CCAT2 expression was associated with a higher risk of lymph node metastasis (LNM), an increased potential for distant metastasis (DM) and higher clinical stage (p<0.001 for LNM, p = 0.001 for DM, p<0.001 for clinical stage). HR and the 95% CI for overall survival (OS) were assessed to pool the effect size using a fixed-effects model. A significant association was observed between increased CCAT2 expression and poor OS (pooled HR = 1.91, 95% CI, 1.63-2.22, p<0.001).
Conclusions
These results indicate that CCAT2 is a biomarker to predict tumor progression and a potential prognostic marker in multiple cancers. Additional well-designed clinical studies are needed to validate these findings.
Introduction
Long noncoding RNAs (IncRNAs) make up a group of non-protein-coding RNAs (ncRNAs) of more than 200 nucleotides in length (1). LncRNAs play a pivotal role in tumor development, cell proliferation, metastasis, invasion, migration and prognosis (2-6).
Identified as a novel IncRNA in 2013, colon cancer–associated transcript 2 (CCAT2) is transcribed from 8q24, encompassing the rs6983267 SNP (7). CCAT2 is overexpressed in microsatellite-stable (MSS) colorectal cancer samples (7). Accumulating studies have suggested that as an oncogene, CCAT2 is involved in various biological and pathological processes, including tumor metastasis, growth, apoptosis, chromosomal instability and energy metabolism (7-11). In breast cancer, CCAT2 might represent a useful predictive marker of clinical outcomes (shorter overall survival [OS] and metastases-free survival) (8), and CCAT2 has also been implicated in up-regulating migration and down-regulating chemosensitivity to 5-fluorouracil (5′FU) in a rs6983267-independent manner (8). Another study showed that CCAT2 promoted tumor growth by regulating the Wnt signaling pathway in breast cancer (12). Redis et al demonstrated that CCAT2 regulated cancer energy metabolism in an allele-specific manner through binding to the cleavage factor I (CFIm) complex with distinct affinities, and this metabolism regulation system was present in 61% of the 18 colorectal cancer cases studied (10).
Until recently, many publications have suggested CCAT2 as an outstanding prognostic marker in many types of cancers in Chinese patients (11, 13-21). Based on the relationship between high CCAT2 levels and human cancer prognosis, we summarized all available data, including those from recently published studies, to more accurately clarify the prognostic value of CCAT2 in various cancers in the Chinese population. This meta-analysis also analyzed the association between CCAT2 expression and clinicopathological parameters, including differentiation grade, lymph node metastasis (LNM), distant metastasis (DM) and clinical stage, thereby enriching the robustness and comprehensiveness of the present study.
Methods
Literature search and study selection
A pair of investigators independently searched for eligible studies to evaluate the clinicopathological and prognostic value of CCAT2 in Chinese patients with cancer, using the PubMed, Web of Science, Cochrane Library, Wanfang and China National Knowledge Infrastructure databases. They also screened abstracts and the full text, and extracted data (G.-W.T. and N.L.). Disagreements were resolved through discussion, with input from other investigators. The search strategy included the following search terms: (“Colon cancer associated transcript 2” or “CCAT2”) and (“cancer” or “carcinoma” or “tumor” or “neoplasm”). Studies published up to March 31, 2017 were identified.
Inclusion and exclusion criteria
Previous studies matching the following criteria were included in the present study: (i) patients with any type of cancer; (ii) the relationship between CCAT2 and clinicopathological parameters (differentiation grade, LNM, DM and clinical stage) was evaluated; (iii) the relationship between CCAT2 and OS was evaluated in the Chinese population; (iv) the hazard ratio (HR) was evaluated using multivariable logistic regression analyses, or the study had Kaplan-Meier curves for extracting the HR; and (v) patients were divided into high and low CCAT2 expression groups. The exclusion criteria included the following: (i) letters, reviews, case report or laboratory studies; (ii) insufficient information for data extraction; (iii) studies with duplicate data or repeat analyses; and (iv) studies of populations other than the Chinese population.
Data extraction and quality assessment
The data from all eligible studies were independently reviewed and extracted by 2 investigators. The extracted data from each study included the first author, year of publication, country of origin, total number of cases, cancer type, cutoff value, HR and 95% CIs for OS, differentiation grade, LNM, DM, and clinical stage (the last combined the TNM stage and the FIGO stage). For studies that did not provide the HR directly, we extracted the HR from the Kaplan-Meier curves according to the method of Tierney et al (22). The Newcastle-Ottawa scale (NOS) was used to assess the quality of all included studies to assess the prognostic significance of CCAT2. Discrepancies between the 2 investigators were resolved by discussion with a third investigator.
Statistical analysis
The meta-analysis was performed using STATA software version 12.0 (StataCorp LP, College Station, TX, USA). The odds ratio (OR) and hazard radio with 95% confidence interval (95% CI) were calculated. The heterogeneity of the pooled results was measured using Cochran's Q test and Higgins' I-squared statistic. Subgroup analysis was performed based on sample size and cancer type, and meta-regression analysis was used to explore the source of the observed heterogeneity. A random-effects model (DerSimonian-Laird method) was used to determine the pooled HRs when p<0.1 or I 2 >50%; otherwise, a fixed-effects model (Mantel-Haenszel method) was applied (23, 24). Publication bias was identified using Begg's test (25) and the “trim and fill” method (26), which estimates the number of missing studies. Furthermore, a sensitivity analysis was used to examine the stability of the pooled results.
Results
Search results and study characteristics
As shown in Figure 1, we identified 78 publications potentially related to CCAT2 expression and cancer. After reviewing the titles and abstracts, we excluded 53 studies, applying the exclusion criteria. For example, Zhou et al, which only investigated the molecular function of CCAT2 in hepatocellular carcinoma (9), was excluded. After reading the full text, 16 studies were included in the present meta-analysis (excluding the 2 publications (10, 27) examining populations other than the Chinese population). The major characteristics of all eligible studies are shown in Tables I and II.
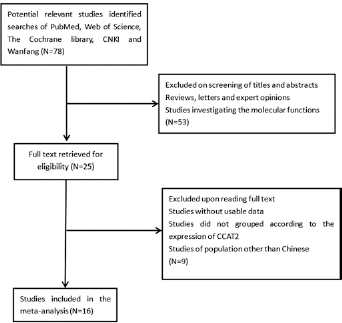
Flow chart of the selection of the included literature. CNKI = China National Knowledge Infrastructure.
Basic characteristics of the included studies for assessing the prognostic significance of CCAT2
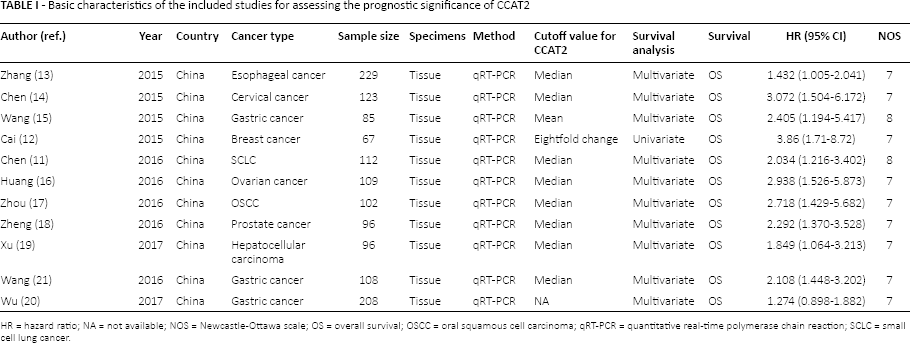
HR = hazard ratio; NA = not available; NOS = Newcastle-Ottawa scale; OS = overall survival; OSCC = oral squamous cell carcinoma; qRT-PCR = quantitative real-time polymerase chain reaction; SCLC = small cell lung cancer.
Clinical characteristics of the included studies for assessing the clinicopathological significance of CCAT2
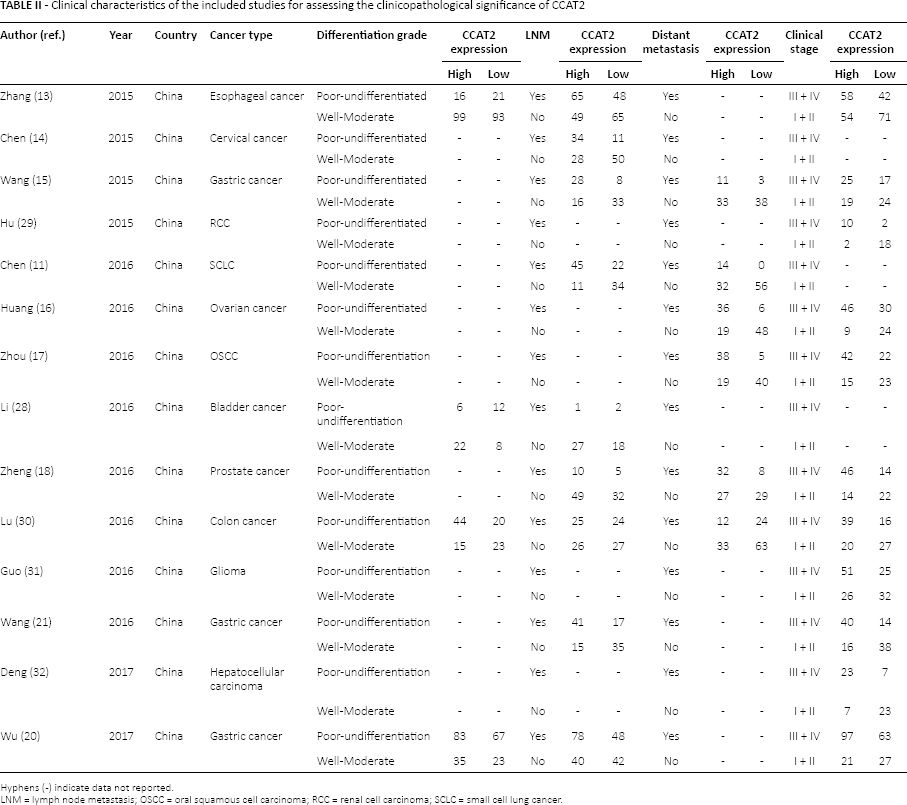
Hyphens (-) indicate data not reported.
LNM = lymph node metastasis; OSCC = oral squamous cell carcinoma; RCC = renal cell carcinoma; SCLC = small cell lung cancer.
A total of 1,711 Chinese patients with 13 different cancers were included in this meta-analysis, which included esophageal cancer (13), cervical cancer (14), gastric cancer (15, 20, 21), small cell lung cancer (SCLC) (11), ovarian cancer (16), oral squamous cell carcinoma (OSCC) (17), bladder cancer (28), prostate cancer(PC) (18), breast cancer (12), renal cell carcinoma (RCC) (29), colon cancer (30), glioma (31) and hepatocellular carcinoma (19, 32). Among the 16 publications, 11 studies assessed the relationship between CCAT2 and prognosis in the Chinese population. Only a single study obtained a HR value, which was extracted from the Kaplan-Meier curve. A total of 4 publications assessed the relationship between CCAT2 and differentiation grade; 9 publications assessed the relationship between CCAT2 and LNM; 6 publications reported the relationship between CCAT2 and DM; and 11 publications reported the relationship between CCAT2 and clinical stage. The sample sizes ranged from 32 to 229. The NOS scores were ≥7 for all included publications.
Quantitative meta-analysis
Correlation of CCAT2 with clinicopathological parameters
The overall analysis showed a significant association between CCAT2 and clinicopathological parameters (LNM, DM and clinical stage). The data demonstrated that higher CCAT2 expression was associated with higher risk of LNM (OR = 2.70, 95% CI, 1.60-4.54, p<0.001), increased potential for DM (OR = 6.36, 95% CI, 2.11-19.19, p = 0.001) and higher clinical stage (OR = 3.44, 95% CI, 2.34-5.04, p<0.001) (Fig. 2). However, CCAT2 expression was not associated with differentiation grade (Fig. 2B).
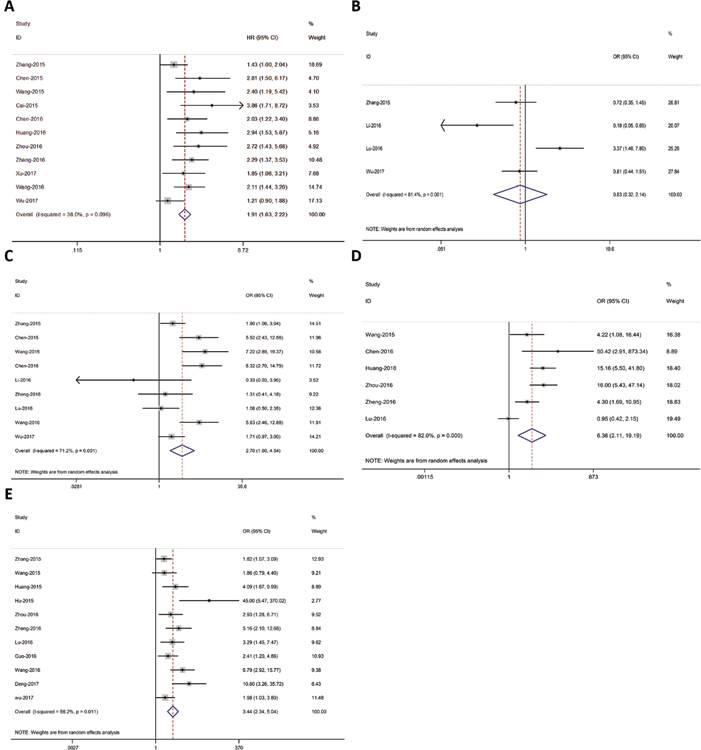
Forest plots of CCAT2 and overall survival (OS) and clinicopathological parameters. (A) Forest plot of CCAT2 expression and OS. (B) Relationship between CCAT2 expression and differentiation grade. (C) Relationship between CCAT2 expression and lymph node metastasis (LNM). (D) Relationship between CCAT2 expression and distant metastasis (DM). (E) Relationship between CCAT2 expression and clinical stage.
Impact of CCAT2 on survival in various tumors in the Chinese population
A total of 11 publications assessed the association between CCAT2 and prognosis in various tumors in the Chinese population. The pooled data indicated that the various tumors in Chinese patients with higher CCAT2 levels had poorer prognoses (HR = 1.91, 95% CI, 1.63-2.22, p<0.001, I 2 = 38.0%; Fig. 2). The p value of the Q test for heterogeneity was 0.096.
Subsequently, we performed a subgroup analysis based on sample size and different cancer types. The results were not significantly changed in the sample size subgroup analysis. In cancer type subgroup analysis, regardless of the cancer system analyzed (digestive system, urinary and genital system or other system), the results indicated that higher CCAT2 expression could predict poorer OS. The subgroup analysis further revealed that the observed heterogeneity could be reduced, particularly in the cancer type subgroup analysis (see Supplementary Table I, available online at www.biological-markers.com – Subgroup analysis of CCAT2 on OS in different types of cancer).
Heterogeneity, publication bias and sensitivity analysis
Heterogeneity was observed for almost all terms. We performed meta-regression analyses to explore the source of this heterogeneity. The results showed that sample size (p = 0.283) and cancer type (p = 0.052) were not the source of the observed heterogeneity. Begg's test was performed to assess the publication bias in all included studies to evaluate OS, differentiation grade, LNM, DM and clinical stage. The statistical data did not reveal any significant publication bias for differentiation grade (p = 0.734), LNM (p = 0.602) or DM (p = 0.452), but significant publication bias was observed for OS (p = 0.02) and clinical stage (p = 0.002) (Tab. III; and see Supplementary Figure 1, available online at www.biological-markers.com – Funnel plots for publication bias).
Results of meta-analysis and publication bias test
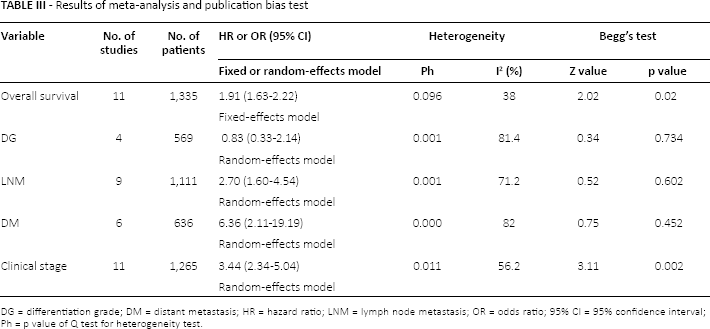
DG = differentiation grade; DM = distant metastasis; HR = hazard ratio; LNM = lymph node metastasis; OR = odds ratio; 95% CI = 95% confidence interval; Ph = p value of Q test for heterogeneity test.
Further, we used the trim and fill method to estimate the number of missing studies. The number of missing studies was 4 for OS and 2 for clinical stage (see Supplementary Figure 1A, E, available online at www.biological-markers.com – Funnel plots for publication bias). Sensitivity analysis was performed through the sequential omission of individual publications. The results were not significantly altered for any study factor after sequentially excluding each study (Supplementary Figure 2, available online at www.biological-markers.com - Sensitivity analysis of the stability of the results).
Discussion
In recent years, the revolutionary findings in human genome analyses have illuminated ncRNAs as a significant part of the human genome, compared with the 2% of protein-coding RNAs (33). As new members of the ncRNA group, IncRNAs have been shown to play significant roles in malignancies. Typically, these molecules exert effects on several cellular levels, such as transcription, posttranscription and chromatin organization, and the mechanisms through which these molecules significantly affect carcinomas are numerous (34). IncRNAs combine with DNA, RNA and protein molecules as a vital bridge to regulate gene expression in cis or trans (35). For example, H19 prevents miR-17-5p from up-regulating YES1, and simultaneously, cell cycle progression is inhibited (36). Antisense RNA is a category of IncRNAs transcribed from the corresponding sense transcript. Since MDC1 was identified as a tumor-suppressor gene (37), in glioma, there was a positive relationship between the IncRNA MDC1-AS and the antisense transcript of MDC1. Moreover, MDC1-AS can not block the cell cycle of glioma cells without MDC1 (38). However, the underlying mechanism of IncRNAs and the clinical and prognosis value of their expression remain elusive.
CCAT2 is a recently identified oncogenic IncRNA whose aberrant up-regulation has been detected in various cancers, including colorectal cancer (CRC) (7), lung cancer (11, 39), gastric cancer (15), breast cancer (8, 12) and hepatocellular cancer (9). Recently, the mechanism of CCAT2 in tumorigenesis has been extensively investigated. In CRC, Ling et al reported that CCAT2 promotes tumor cell invasion and metastasis by activating the MYC gene and Wnt signaling, which supports cell proliferation, metastasis and cancer metabolism (7). Consistent with the results in CRC, the abnormal expression of CCAT2 has also been shown to influence Wnt signaling in breast tumors (12). Zhang et al also showed that esophageal squamous cell carcinoma (ESCC) patients with high levels of CCAT2 and MYC amplification have the worse prognoses (13), likely reflecting the fact that CCAT2 and MYC are both located on chromosome sub-subband 8q24.21. A study reported that CCAT2 plays a crucial role in hepatocellular carcinoma cell proliferation, migration and apoptosis (9). In PC, the up-regulation of CCAT2 promoted metastasis by affecting the epithelial-mesenchymal transition (EMT) (18). Based on these studies and reflecting its functions, CCAT2 might be one of the crucial factors for tumorigenesis and a new target for tumor therapy.
We performed a comprehensive meta-analysis to assess the relationship between higher CCAT2 levels and clinicopathological and outcome features in various tumors in patients in the Chinese population. In the present study, we combined the outcomes for 1,711 patients from 16 available studies, and the results indicated that a high CCAT2 level was significantly associated with poor OS (HR = 1.91, 95% CI, 1.63-2.22, p<0.001) in different tumors in the Chinese population. A significant relationship was detected between CCAT2 levels and clinicopathological features (LNM, DM and clinical stage). Sensitivity analysis showed that there was no single study affecting the results of the present meta-analysis. Therefore, these results are stable.
Although these results are consistent with those of previous meta-analyses (40-42), the present study still has several strengths through careful retrieval and in-depth statistical analysis. To our knowledge, this study is the most comprehensive meta-analysis evaluating the relationship between CCAT2 and cancers in the Chinese population, including assessing the associations between increased CCAT2 levels, clinicopathological data and OS. First, the number of included studies was 16, which is more than the number of studies included in previous meta-analyses. Thus, the present study incorporated evidence from more recent studies and was more comprehensive. Second, we added new knowledge of the relationship between increased CCAT2 level and differentiation grade, although the results were negative. Moreover, in-depth statistics were analyzed in the present study. We used subgroup analysis, meta-regression and the trim and fill method to obtain a more comprehensive meta-analysis.
Nevertheless, there were some limitations to the present study that should be carefully considered. First, we extracted the HR from a survival curve in one study rather than directly obtaining this value from the original study, which might have affected the results. Second, the p value of heterogeneity was in Table III. We conducted a meta-regression analysis to identify the source of the observed heterogeneity, and determined that neither cancer type nor sample size was the source. The observed heterogeneity may reflect other factors. However, we could not identify the source factors, because we did not have access to all other factors in the original source data. Furthermore, cutoff values were different, and there was no accepted and validated method to assess CCAT2 expression. These factors may have contributed to the observed heterogeneity. Third, studies with negative results are generally less likely to be published. Among the included studies, almost all studies had positive results, and publication bias regarding OS and clinical stages were determined using Begg's test. Therefore, we the estimated the number of missing studies using the trim and fill method. The number of missing studies was 4 for OS and 2 for clinical stage. Therefore, whether CCAT2 is a potential prognostic predictor in Chinese patients with cancer still needs further investigation.
With respect to clinical utility, CCAT2 overexpression is associated with poor clinical outcomes in multiple cancer types. For LNM in NSCLC, CCAT2 alone had low predictive efficiency. When CCAT2 combined with carcinoembryonic antigen (CEA) can significantly improve the predictive efficiency (39). In gastric cancer, the combination of CCAT2 and 4 other IncRNAs (TINCR, AOC4P, BANCR and LINC00857) can improve diagnostic accuracy (43). However, almost all studies did not include an independent cohort for validation. Therefore, multicenter, well-designed clinical trials are needed to focus on the clinical utility of CCAT2 as a biomarker.
In conclusion, based on the summarization of all available evidence, the present meta-analysis showed that higher CCAT2 levels are significantly associated with poor OS in Chinese patients with cancer. If replicated in additional large-scale well-designed studies, these findings may support the use of CCAT2 as a biomarker in tumors.
Footnotes
Financial support: This work was financially supported by grants from the National Natural Science Foundation of China (No. 81071650; 30973503), the Special Foundation for Science and Technology Program in Liaoning Province, China (2013225303-103; 2011404013-3) and the Supporting Project for Climbing Scholars in Liaoning Provincial Universities, China (2009-2012).
Conflict of interest: The authors declare they have no competing financial interests.