AGENAS National Agency for Regional Health Services, Rome, Italy
Regional Center for Biomarkers, Azienda ULSS 3 Serenissima - formerly Azienda ULSS 12 Veneziana, Venice, Italy
On behalf of and in collaboration with
Regione del Veneto, IOV - Istituto Oncologico Veneto - I.R.C.C.S., AIOM (Associazione Italiana di Oncologia Medica), SIBioC - Medicina di Laboratorio (Società Italiana di Biochimica Clinica e Biologia Molecolare Clinica), AIRO (Associazione Italiana di Radioterapia Oncologica), ELAS-Italia (European Ligand Assay Society Italia), FADOI (Federazione delle Associazioni dei Dirigenti Ospedalieri Internisti), SICO (Società Italiana di Chirurgia Oncologica), SIGO (Società Italiana di Ginecologia e Ostetricia), SIMG (Società Italiana di Medicina Generale), SIUrO (Società Italiana di Urologia Oncologica), AVAPO Venezia Onlus (Associazione Volontari per l'Assistenza di Pazienti Oncologici)
Steering Committee
Mario Braga, Massimo Gion, Carmine Pinto, Bruno Rusticali, Holger Schünemann, Tommaso Trenti
For complete contributors' affiliations see end of article (pp. e178-e181)
Scientific Committee
Aline S.C. Fabricio, Evaristo Maiello, Anne W.S. Rutjes, Valter Torri, Quinto Tozzi, Chiara Trevisiol
For complete contributors' affiliations see end of article (pp. e178-e181)
Multidisciplinary panel of experts
Salvatore Alfieri(5), Emiliano Aroasio(3,5), Alessandro Bertaccini(3,5), Francesco Boccardo(3,5), Roberto Buzzoni(3,5), Maurizio Cancian(5), Ettore D. Capoluongo(5), Elisabetta Cariani(5), Vanna Chiarion Sileni(3,5), Michela Cinquini(1,3,5), Giuseppe Civardi(5), Renzo Colombo(3,5), Mario Correale(3,5), Gaetano D'Ambrosio(5), Bruno Daniele(3,5), Marco Danova(3,5), Giovanna Del Vecchio Blanco(3,5), Francesca Di Fabio(3,5), Massimo Di Maio(3,5), Ruggero Dittadi(3,5), Massimo Falconi(3,5), Andrea Fandella(3,5), Tommaso Fasano(5), Simona Ferraro(3,5), Antonio Fortunato(3,5), Bruno Franco Novelletto(5), Angiolo Gadducci(3,5), Luca Germagnoli(3,5), Maria Grazia Ghi(3,5), Davide Giavarina(3,5), Marién González Lorenzo(2,5), Stefania Gori(3,5), Fiorella Guadagni(3,5), Cinzia Iotti(3,5), Tiziana Latiano(1,3,5), Lisa Licitra(3,5), Tiziano Maggino(5), Gianluca Masi(5), Paolo Morandi(3,5), Maria Teresa Muratore(3,5), Gianmauro Numico(5), Valentina Pecoraro(2,5), Paola Pezzati(3,5), Silvia Pregno(5), Giulia Rainato(4), Stefano Rapi(3,5), Francesco Ricci(3,5), Lorena Fabiola Rojas Llimpe(3,5), Laura Roli(1,5), Giovanni Rosti(3,5), Tiziana Rubeca(3,5), Giuseppina Ruggeri(5), Gian Luca Salvagno(5), Maria Teresa Sandri(5), Giovanni Scambia(3,5), Mario Scartozzi(3,5), Vincenzo Scattoni(3,5), Giuseppe Sica(3,5), Alessandro Terreni(3,5), Marcello Tiseo(3,5), Paolo Zola(5) For complete contributors' affiliations see end of article (pp. e178-e181)
Contributions of panel members
(1) Search and selection of guidelines
(2) Appraisal of guidelines through the AGREE II tool
(3) Assessment of the rate of utilization of a subset of guidance documents in clinical practice
(4) Synthesis of recommendations and other information concerning tumor markers into summary tables
(5) Assessment of correctness and completeness of the information summarized in the tables
External validation
Interregional Biomarkers Working Group, instituted by the Health Commission of the Italian Permanent Conference for Relations between State, Regions and the Autonomous Provinces of Trento and Bolzano. Antonino Iaria (Calabria), Vincenzo Montesarchio (Campania), Tommaso Trenti (Emilia Romagna), Laura Conti (Lazio), Luigina Bonelli and Gabriella Paoli (Liguria), Mario Cassani (Lombardia), Lucia Di Furia (Marche), Emiliano C. Aroasio (Piemonte), Mario Brandi (Puglia), Marcello Ciaccio and Antonio Russo (Sicilia), Gianni Amunni (Toscana), Emanuela Toffalori (P.A. Trento), Basilio Ubaldo Passamonti (Umbria), Claudio Pilerci and Francesca Russo (Veneto), Annarosa Del Mistro (IOV IRCCS, Veneto)
Executive secretary
Ornella Scattolin
Funding
AGENAS Agenzia Nazionale per i Servizi Sanitari Regionali
Azienda ULSS 12 Veneziana
IOV - Istituto Oncologico Veneto - I.R.C.C.S.
AIOM (Associazione Italiana di Oncologia Medica)
SIBioC - Medicina di Laboratorio (Società Italiana di Biochimica Clinica e Biologia Molecolare Clinica)
ELAS-Italia (European Ligand Assay Society Italia)
SIUrO (Società Italiana di Urologia Oncologica)
AVAPO Venezia Onlus (Associazione Volontari per l'Assistenza di Pazienti Oncologici)
This study was helpful in the exploration of unmet needs in tumor marker application in the frame of an AIRC 5×1000 research project, from which it was partially supported (Italian Association for Research on Cancer - AIRC; Grant Special Program Molecular Clinical Oncology, 5×1000, No. 12214).
The authors would like to thank the following cultural associations in Venice for their support
Associazione “Un amico a Venezia”, “Chiostro Tintorettiano di Venezia”, “I ragazzi di don Bepi”, SKÅL International Venezia for their support.
This guide is published in Italian as:
Gion M, Trevisiol C, Rainato G, Fabricio ASC. Marcatori circolanti in oncologia: guida all'uso clinico appropriato. I Quaderni di Monitor. Roma, IT: AGENAS, Agenzia Nazionale per i Servizi Sanitari Regionali, 2016.
Contents
Introduction e150
Take-home messages
Users' instructions e151
Head and neck cancer e152
Lung cancer e153
Melanoma e155
Mesothelioma e157
Thyroid cancer, differentiated e159
Thyroid cancer, medullary (MTC) e161
Detailed summary tables
Users' instructions e163
Head and neck cancer e164
Lung cancer e165
Melanoma e166
Mesothelioma e167
Thyroid cancer, differentiated e169
Thyroid cancer, medullary (MTC) e172
Selected guidelines (by cancer site) e175
Contributors e178
Introduction
This is the last part of a guide to the appropriate clinical use of circulating tumor markers (TMs). The full document was published in Italy in October 2016 by the Italian National Agency for Regional Health Services (AGENAS) on behalf of and in collaboration with 9 Italian scientific societies representative of a range of stakeholders (1). The publication of the document in English was planned in 3 parts: the first, concerning malignancies of the gastrointestinal tract, was published in December 2016 (2); the second, published in February 2017 (3), addressed urogenital tract malignancies and breast cancer; the third, appearing in the present issue, refers to head-and-neck, thyroid and thoracic malignancies and melanoma.
Rationale
The number of TM tests requested is considerably higher than expected based on the cancer prevalence, and this shows the low compliance of physicians to clinical practice guidelines (CPGs). Barriers preventing clinicians from adherence to CPG recommendations include discrepancies between the cautious position of CPGs and the encouraging results of primary studies. In fact, the evidence provided by primary studies tends to focus on the diagnostic accuracy of the tests rather than on patient outcomes, the latter being a prerequisite for good-level evidence in guideline development. While awaiting the incorporation of higher-quality evidence into comprehensive guidelines, efforts should be made to improve the adherence to existing CPGs. A project was developed to summarize recommendations on circulating TMs offered by available CPGs on solid tumors, in order to provide all possible evidence-based choices concerning TMs to anyone facing a clinical question in which the use of a TM could be considered.
The implicit goal of the present guidance document is to “stimulate discussion and promote commentaries and debate, with the ultimate ambition of improving the appropriate use of TMs but also optimizing the proposed model of comparative summary of the available evidence to facilitate extensive dissemination and consultation of the guidance provided” (4).
Methods
The structured and rigorous methodology adopted for the extraction and synthesis of relevant information from selected guidelines has been previously described in detail (2). In brief, a systematic search for CPGs was performed and a standardized set of selection criteria was used to identify potentially relevant publications. Only documents containing recommendations for clinical practice were included. A total of 1,181 potentially relevant documents were selected from 8,266 identified records. Full-text reports were obtained for 559 guidance documents concerning 20 different malignancies. The selected documents were further appraised for adherence to the standards of the Institute of Medicine (IOM), which require CPGs to be based on systematic review of existing evidence (5), and clustered into 2 groups: 127 documents in which recommendations were generated through systematic review (CPGs) and 432 guidance documents without evidence of systematic review (Other Guidance Documents – OGDs). CPGs were further assessed with the Appraisal of Guidelines for Research & Evaluation (AGREE II) tool in order to facilitate comparison of the quality of the summarized CPGs. OGDs produced by authoritative institutions or medical societies are currently used by clinicians in their daily practice. All OGDs were therefore presented to the panel members with a request to indicate those actually used in clinical practice. When 25% or more of the panel members declared that a given guidance document was used in clinical practice, it was retained. In all, 111 of 432 OGDs qualified for inclusion. Circulating biomarkers measured in body fluids (serum or plasma/urine) were considered.
Results
The tabulation of the information was structured by individual malignancies; within each malignancy, the information was clustered according to a set of clinical questions established as being common to all malignancies. All information extracted from the guidance documents was synthesized in 4 rounds (levels) of increasing simplification. The last 2 levels of synthesis are the Take-Home Messages and Detailed Summary Tables. The former are intended for use by health care providers in their clinical practice with the goal of improving the appropriateness of TM use; the latter are addressed to policy makers for potential adaptation to their own context, and to educators, allowing them to design teaching programs consistent with the available evidence.
Take-home messages
Users' instructions
Definition and target audience
Take-Home Messages are presented in table format for every tumor type, summarizing essential information to support decision-making in clinical practice. They are intended for use by health care providers.
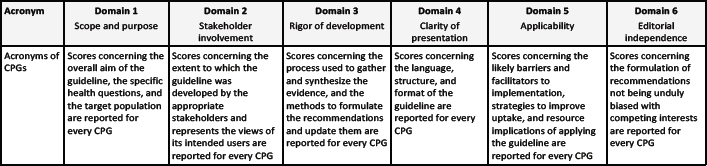
Agree evaluation
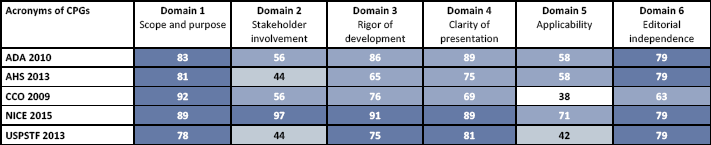
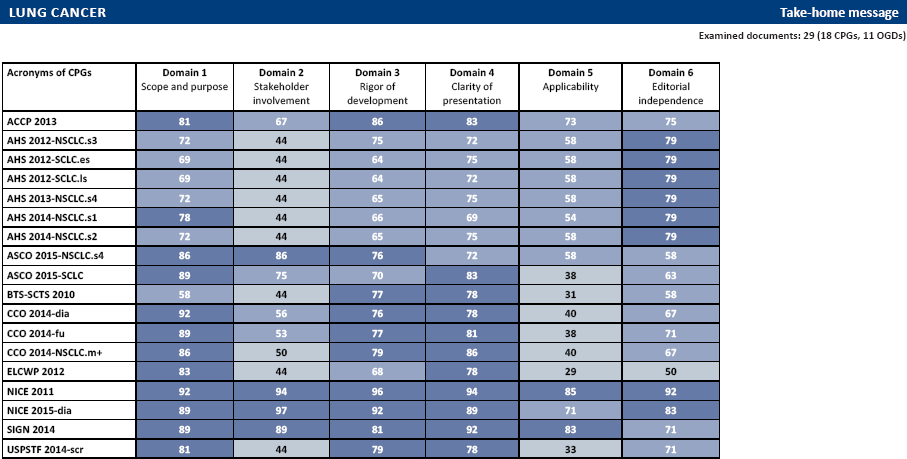
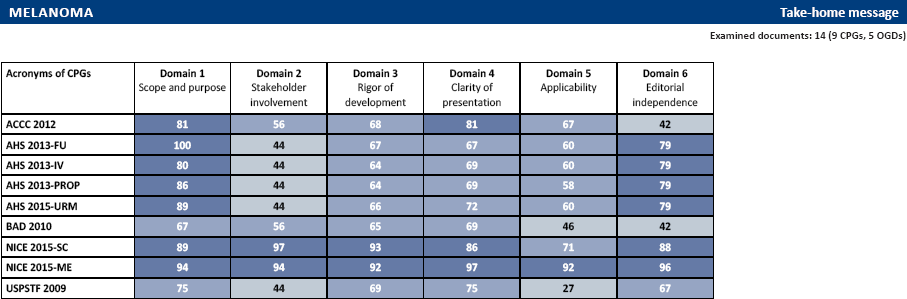
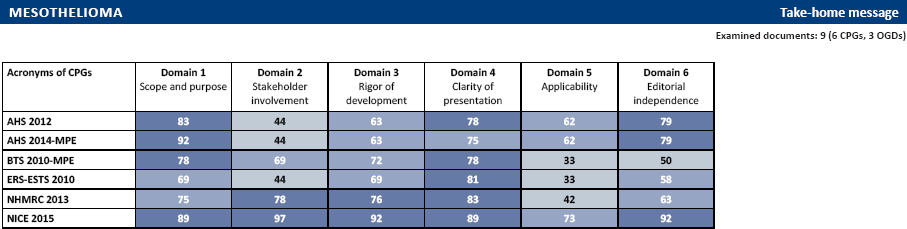
CPGs concerning every malignancy were also assessed with the Appraisal of Guidelines for Research & Evaluation (AGREE II) tool. A higher score equals a better quality of the domain. The results are reported after the Take-Home Message tables.
Acronym
Domain 1 Scope and purpose
Domain 2 Stakeholder involvement
Domain 3 Rigor of development
Domain 4 Clarity of presentation
Domain 5 Applicability
Domain 6 Editorial independence
Acronyms of CPGs
Scores concerning the overall aim of the guideline, the specific health questions, and the target population are reported for every CPG
Scores concerning the extent to which the guideline was developed by the appropriate stakeholders and represents the views of its intended users are reported for every CPG
Scores concerning the process used to gather and synthesize the evidence, and the methods to formulate the recommendations and update them are reported for every CPG
Scores concerning the language, structure, and format of the guideline are reported for every CPG
Scores concerning the likely barriers and facilitators to implementation, strategies to improve uptake, and resource implications of applying the guideline are reported for every CPG
Scores concerning the formulation of recommendations not being unduly biased with competing interests are reported for every CPG
The scores of the 6 domains were subdivided into quartiles and marked in different colors as shown in the following table:
0-25th percentile
26th-50th percentile
51th-75th percentile
76th-100th percentile
Additional notes
Take-Home Messages are reported in alphabetical order.
Information from OGDs on a specific clinical question were only reported in the Take-Home Messages if the clinical question was considered by CPGs. Descriptions regarding these OGDs can, however, be found in the Detailed Summary Tables.
References concerning both CPGs and OGDs are reported after the Detailed Summary Tables, divided by type of malignancy and cited with the acronyms used in the Tables.
Detailed summary tables
Users' instructions
Definition and target audience
Take-Home Messages are presented in table format for every tumor type, summarizing essential information to support decision-making in clinical practice. They are intended for use by health care providers.
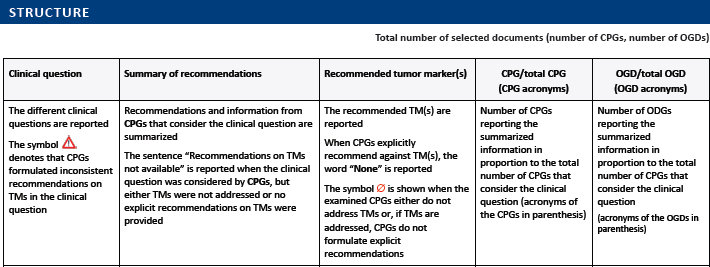
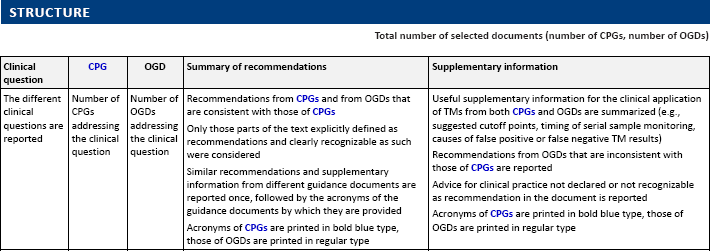
Structure
Total number of selected documents (number of CPGs, number of OGDs)
Clinical question
CPG
OGD
Summary of recommendations
Supplementary information
The different clinical questions are reported
Number of CPGs addressing the clinical question
Number of OGDs addressing the clinical question
Recommendations from CPGs and from OGDs that are consistent with those of CPGs
Only those parts of the text explicitly defined as recommendations and clearly recognizable as such were considered
Similar recommendations and supplementary information from different guidance documents are reported once, followed by the acronyms of the guidance documents by which they are provided
Acronyms of CPGs are printed in bold blue type, those of OGDs are printed in regular type
Useful supplementary information for the clinical application of TMs from both CPGs and OGDs are summarized (e.g., suggested cutoff points, timing of serial sample monitoring, causes of false positive or false negative TM results)
Recommendations from OGDs that are inconsistent with those of CPGs are reported
Advice for clinical practice not declared or not recognizable as recommendation in the document is reported
Acronyms of CPGs are printed in bold blue type, those of OGDs are printed in regular type
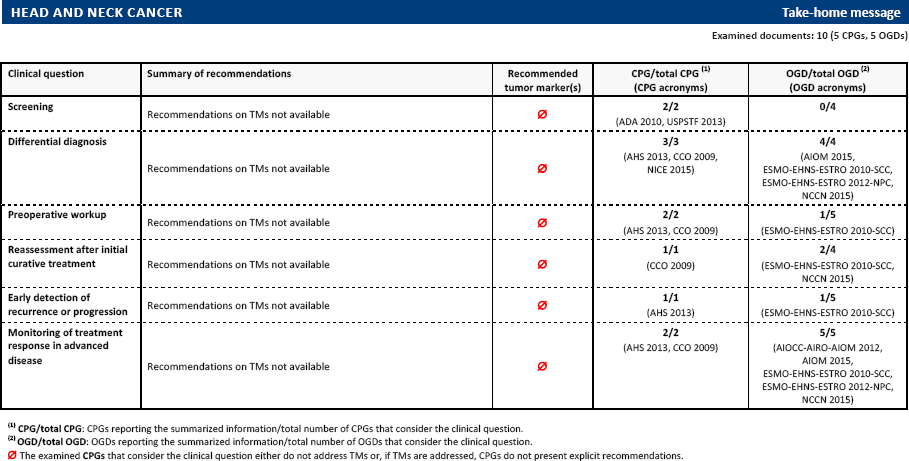
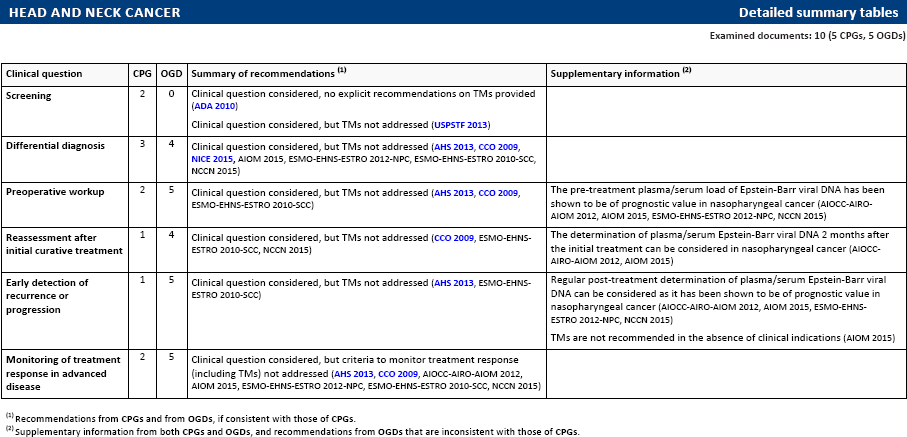
Clinical question considered, but TMs not addressed (AHS 2013, CCO 2009, ESMO-EHNS-ESTRO 2010-SCC)
The pre-treatment plasma/serum load of Epstein-Barr viral DNA has been shown to be of prognostic value in nasopharyngeal cancer (AIOCC-AIRO-AIOM 2012, AIOM 2015, ESMO-EHNS-ESTRO 2012-NPC, NCCN 2015)
Reassessment after initial curative treatment
1
4
Clinical question considered, but TMs not addressed (CCO 2009, ESMO-EHNS-ESTRO 2010-SCC, NCCN 2015)
The determination of plasma/serum Epstein-Barr viral DNA 2 months after the initial treatment can be considered in nasopharyngeal cancer (AIOCC-AIRO-AIOM 2012, AIOM 2015)
Early detection of recurrence or progression
1
5
Clinical question considered, but TMs not addressed (AHS 2013, ESMO-EHNS-ESTRO 2010-SCC)
Regular post-treatment determination of plasma/serum Epstein-Barr viral DNA can be considered as it has been shown to be of prognostic value in nasopharyngeal cancer (AIOCC-AIRO-AIOM 2012, AIOM 2015, ESMO-EHNS-ESTRO 2012-NPC, NCCN 2015)
TMs are not recommended in the absence of clinical indications (AIOM 2015)
Monitoring of treatment response in advanced disease
2
5
Clinical question considered, but criteria to monitor treatment response (including TMs) not addressed (AHS 2013, CCO 2009, AIOCC-AIRO-AIOM 2012, AIOM 2015, ESMO-EHNS-ESTRO 2012-NPC, ESMO-EHNS-ESTRO 2010-SCC, NCCN 2015)
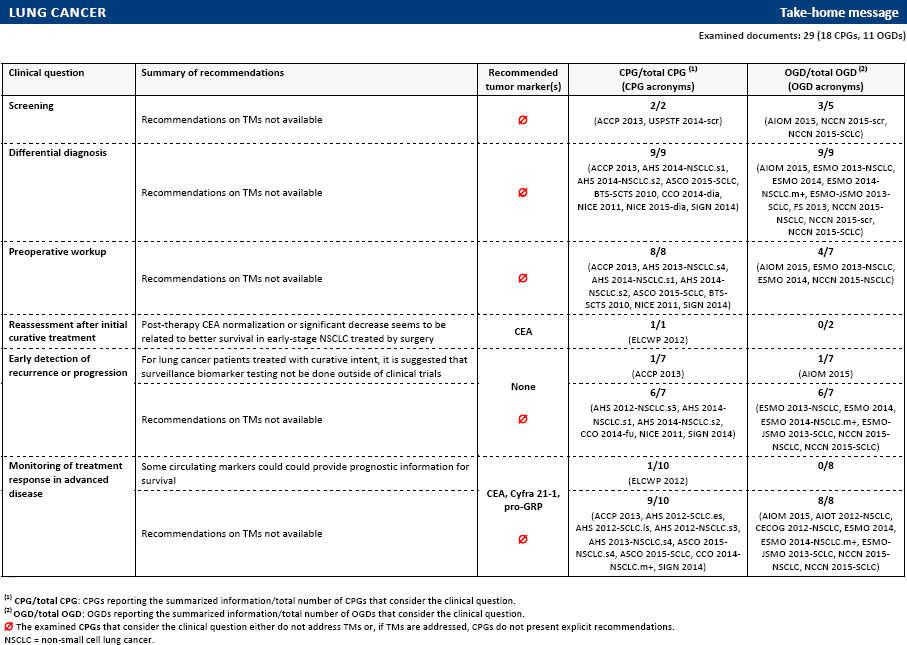
Recommendations from CPGs and from OGDs, if consistent with those of CPGs.
Supplementary information from both CPGs and OGDs, and recommendations from OGDs that are inconsistent with those of CPGs.
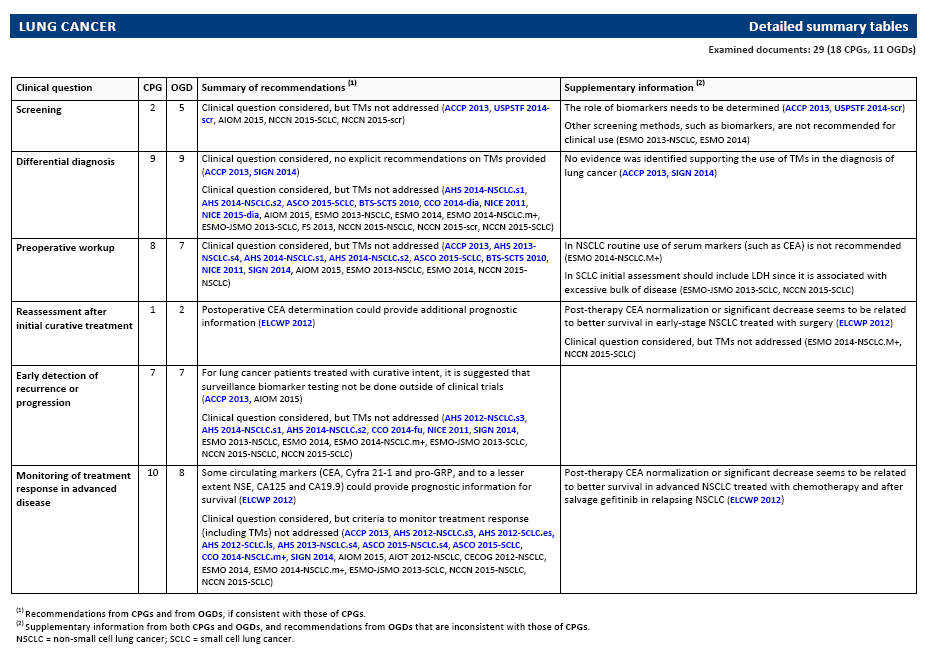
In NSCLC routine use of serum markers (such as CEA) is not recommended (ESMO 2014-NSCLC.M+)
In SCLC initial assessment should include LDH since it is associated with excessive bulk of disease (ESMO-JSMO 2013-SCLC, NCCN 2015-SCLC)
Reassessment after initial curative treatment
1
2
Postoperative CEA determination could provide additional prognostic information (ELCWP 2012)
Post-therapy CEA normalization or significant decrease seems to be related to better survival in early-stage NSCLC treated with surgery (ELCWP 2012)
Clinical question considered, but TMs not addressed (ESMO 2014-NSCLC.M+, NCCN 2015-SCLC)
Early detection of recurrence or progression
7
7
For lung cancer patients treated with curative intent, it is suggested that surveillance biomarker testing not be done outside of clinical trials (ACCP 2013, AIOM 2015)
Monitoring of treatment response in advanced disease
10
8
Some circulating markers (CEA, Cyfra 21-1 and pro-GRP, and to a lesser extent NSE, CA125 and CA19.9) could provide prognostic information for survival (ELCWP 2012)
Post-therapy CEA normalization or significant decrease seems to be related to better survival in advanced NSCLC treated with chemotherapy and after salvage gefitinib in relapsing NSCLC (ELCWP 2012)
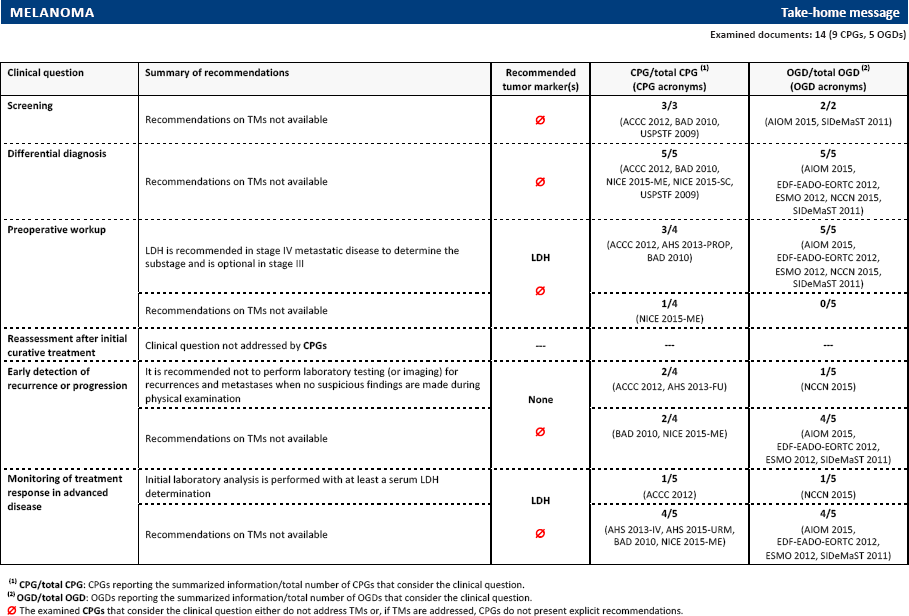
Recommendations from CPGs and from OGDs, if consistent with those of CPGs.
Supplementary information from both CPGs and OGDs, and recommendations from OGDs that are inconsistent with those of CPGs.
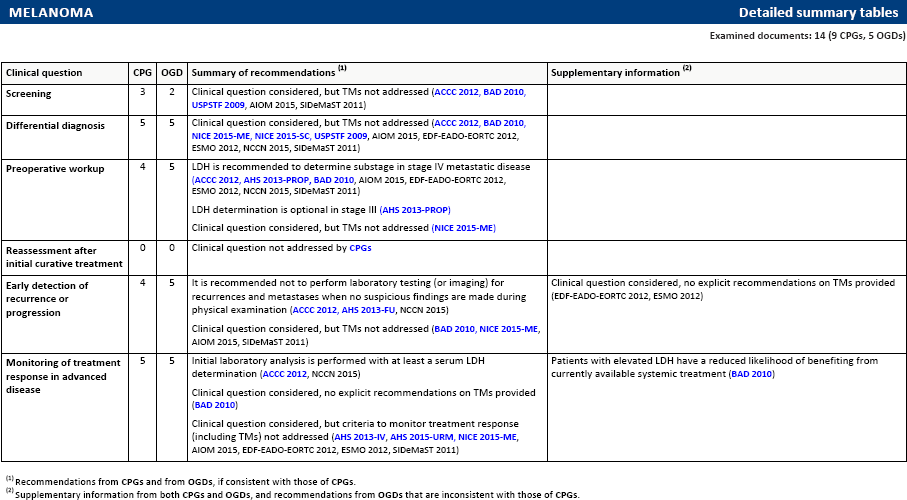
Clinical question considered, but TMs not addressed (ACCC 2012, BAD 2010, USPSTF 2009, AIOM 2015, SIDeMaST 2011)
Differential diagnosis
5
5
Clinical question considered, but TMs not addressed (ACCC 2012, BAD 2010, NICE 2015-ME, NICE 2015-SC, USPSTF 2009, AIOM 2015, EDF-EADO-EORTC 2012, ESMO 2012, NCCN 2015, SIDeMaST 2011)
Pre-Operative workup
4
5
LDH is recommended to determine substage in stage IV metastatic disease (ACCC 2012, AHS 2013-PROP, BAD 2010, AIOM 2015, EDF-EADO-EORTC 2012, ESMO 2012, NCCN 2015, SIDeMaST 2011)
LDH determination is optional in stage III (AHS 2013-PROP)
Clinical question considered, but TMs not addressed (NICE 2015-ME)
Reassessment after initial curative treatment
0
0
Clinical question not addressed by CPGs
Early detection of recurrence or progression
4
5
It is recommended not to perform laboratory testing (or imaging) for recurrences and metastases when no suspicious findings are made during physical examination (ACCC 2012, AHS 2013-FU, NCCN 2015)
Clinical question considered, but TMs not addressed (BAD 2010, NICE 2015-ME, AIOM 2015, SIDeMaST 2011)
Clinical question considered, no explicit recommendations on TMs provided (EDF-EADO-EORTC 2012, ESMO 2012)
Monitoring of treatment response in advanced disease
5
5
Initial laboratory analysis is performed with at least a serum LDH determination (ACCC 2012, NCCN 2015)
Clinical question considered, no explicit recommendations on TMs provided (BAD 2010)
Clinical question considered, but criteria to monitor treatment response (including TMs) not addressed (AHS 2013-IV, AHS 2015-URM, NICE 2015-ME, AIOM 2015, EDF-EADO-EORTC 2012, ESMO 2012, SIDeMaST 2011)
Patients with elevated LDH have a reduced likelihood of benefiting from currently available systemic treatment (BAD 2010)
Recommendations from CPGs and from OGDs, if consistent with those of CPGs.
Supplementary information from both CPGs and OGDs, and recommendations from OGDs that are inconsistent with those of CPGs.
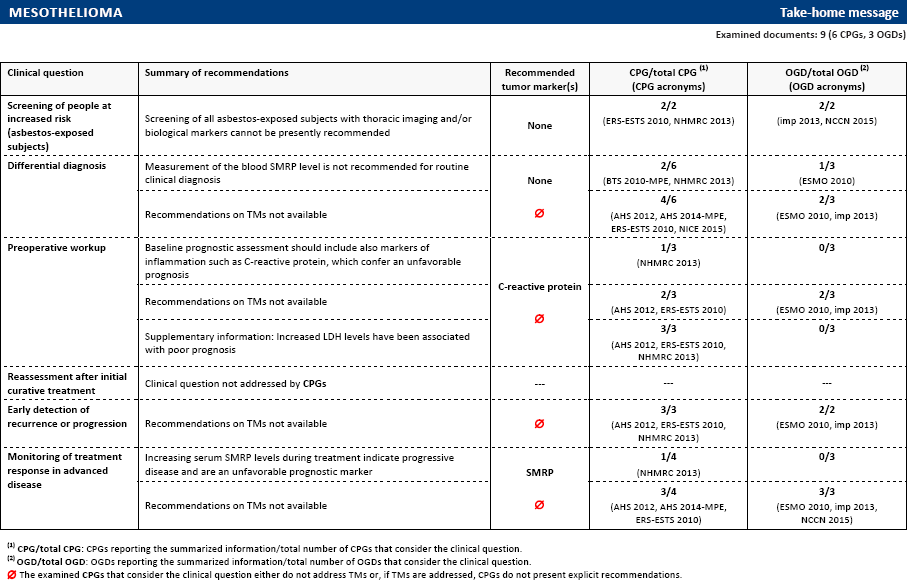
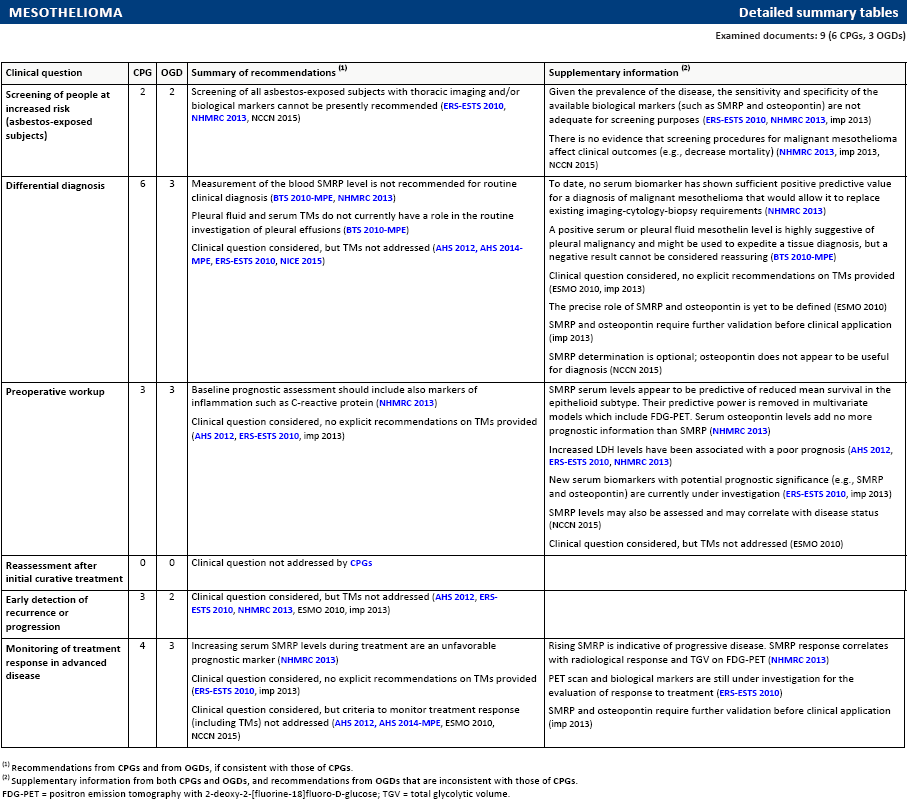
Screening of people at increased risk (asbestos-exposed subjects)
2
2
Screening of all asbestos-exposed subjects with thoracic imaging and/or biological markers cannot be presently recommended (ERS-ESTS 2010, NHMRC 2013, NCCN 2015)
Given the prevalence of the disease, the sensitivity and specificity of the available biological markers (such as SMRP and osteopontin) are not adequate for screening purposes (ERS-ESTS 2010, NHMRC 2013, imp 2013)
There is no evidence that screening procedures for malignant mesothelioma affect clinical outcomes (e.g., decrease mortality) (NHMRC 2013, imp 2013, NCCN 2015)
Differential diagnosis
6
3
Measurement of the blood SMRP level is not recommended for routine clinical diagnosis (BTS 2010-MPE, NHMRC 2013)
Pleural fluid and serum TMs do not currently have a role in the routine investigation of pleural effusions (BTS 2010-MPE)
Clinical question considered, but TMs not addressed (AHS 2012, AHS 2014-MPE, ERS-ESTS 2010, NICE 2015)
To date, no serum biomarker has shown sufficient positive predictive value for a diagnosis of malignant mesothelioma that would allow it to replace existing imaging-cytology-biopsy requirements (NHMRC 2013)
A positive serum or pleural fluid mesothelin level is highly suggestive of pleural malignancy and might be used to expedite a tissue diagnosis, but a negative result cannot be considered reassuring (BTS 2010-MPE)
Clinical question considered, no explicit recommendations on TMs provided (ESMO 2010, imp 2013)
The precise role of SMRP and osteopontin is yet to be defined (ESMO 2010)
SMRP and osteopontin require further validation before clinical application (imp 2013)
SMRP determination is optional; osteopontin does not appear to be useful for diagnosis (NCCN 2015)
Pre-Operative workup
3
3
Baseline prognostic assessment should include also markers of inflammation such as C-reactive protein (NHMRC 2013)
Clinical question considered, no explicit recommendations on TMs provided (AHS 2012, ERS-ESTS 2010, imp 2013)
SMRP serum levels appear to be predictive of reduced mean survival in the epithelioid subtype. Their predictive power is removed in multivariate models which include FDG-PET. Serum osteopontin levels add no more prognostic information than SMRP (NHMRC 2013)
Increased LDH levels have been associated with a poor prognosis (AHS 2012, ERS-ESTS 2010, NHMRC 2013)
New serum biomarkers with potential prognostic significance (e.g., SMRP and osteopontin) are currently under investigation (ERS-ESTS 2010, imp 2013)
SMRP levels may also be assessed and may correlate with disease status (NCCN 2015)
Clinical question considered, but TMs not addressed (ESMO 2010)
Reassessment after initial curative treatment
0
0
Clinical question not addressed by CPGs
Early detection of recurrence or progression
3
2
Clinical question considered, but TMs not addressed (AHS 2012, ERS-ESTS 2010, NHMRC 2013, ESMO 2010, imp 2013)
Monitoring of treatment response in advanced disease
4
3
Increasing serum SMRP levels during treatment are an unfavorable prognostic marker (NHMRC 2013)
Clinical question considered, no explicit recommendations on TMs provided (ERS-ESTS 2010, imp 2013)
Clinical question considered, but criteria to monitor treatment response (including TMs) not addressed (AHS 2012, AHS 2014-MPE, ESMO 2010, NCCN 2015)
Rising SMRP is indicative of progressive disease. SMRP response correlates with radiological response and TGV on FDG-PET (NHMRC 2013)
PET scan and biological markers are still under investigation for the evaluation of response to treatment (ERS-ESTS 2010)
SMRP and osteopontin require further validation before clinical application (imp 2013)
Recommendations from CPGs and from OGDs, if consistent with those of CPGs.
Supplementary information from both CPGs and OGDs, and recommendations from OGDs that are inconsistent with those of CPGs.
FDG-PET = positron emission tomography with 2-deoxy-2-[fluorine-18]fluoro-D-glucose; TGV = total glycolytic volume.
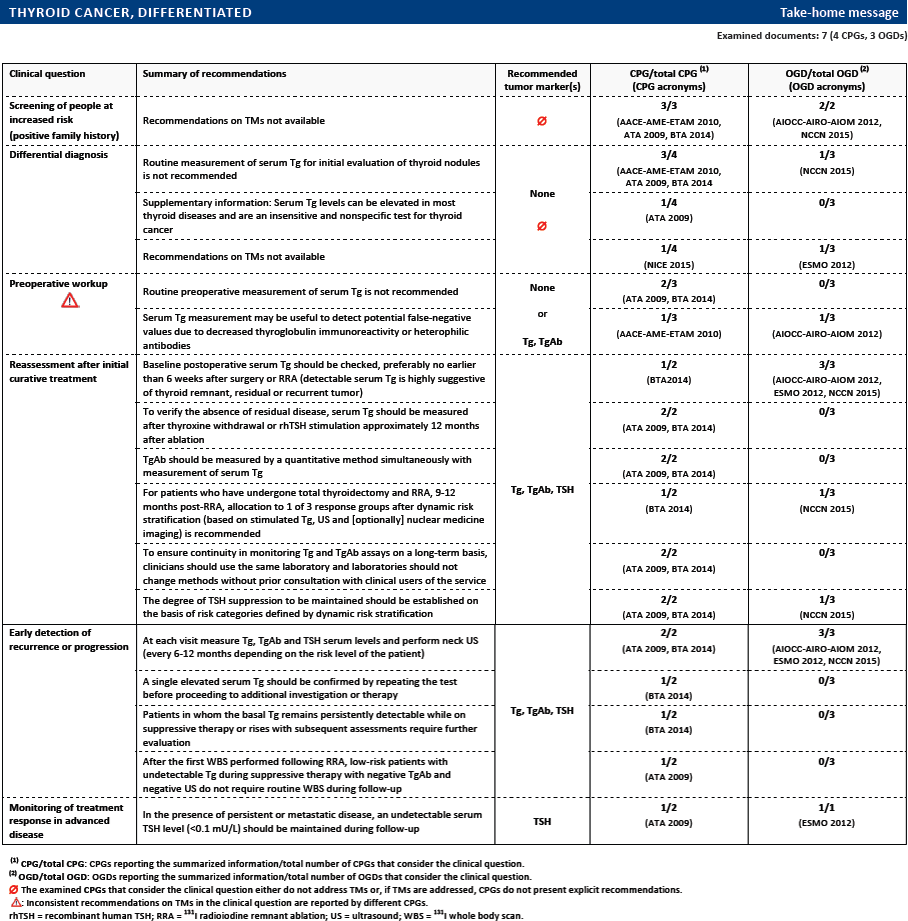
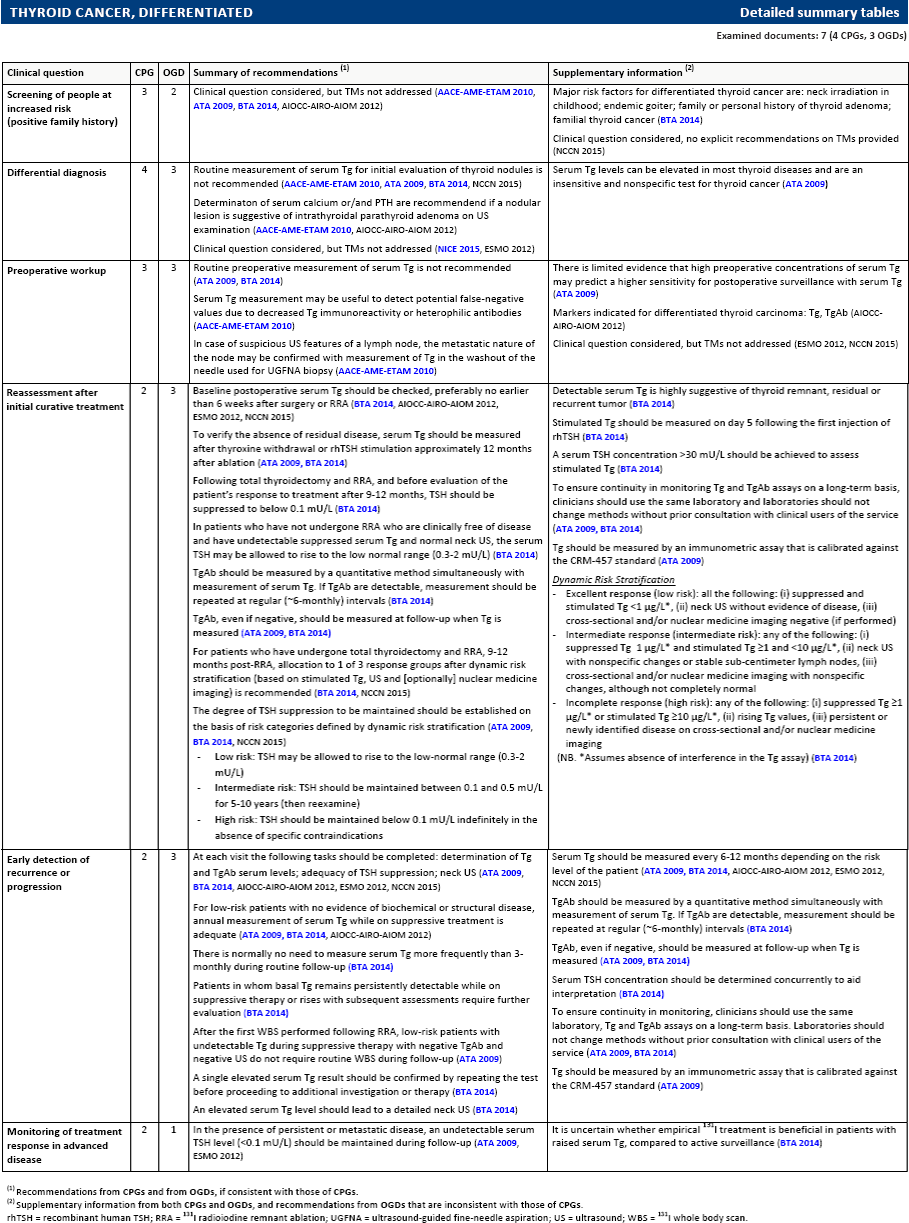
Screening of people at increased risk (positive family history)
3
2
Clinical question considered, but TMs not addressed (AACE-AME-ETAM 2010, ATA 2009, BTA 2014, AIOCC-AIRO-AIOM 2012)
Major risk factors for differentiated thyroid cancer are: neck irradiation in childhood; endemic goiter; family or personal history of thyroid adenoma; familial thyroid cancer (BTA 2014)
Clinical question considered, no explicit recommendations on TMs provided (NCCN 2015)
Differential diagnosis
4
3
Routine measurement of serum Tg for initial evaluation of thyroid nodules is not recommended (AACE-AME-ETAM 2010, ATA 2009, BTA 2014, NCCN 2015)
Determinaton of serum calcium or/and PTH are recommendend if a nodular lesion is suggestive of intrathyroidal parathyroid adenoma on US examination (AACE-AME-ETAM 2010, AIOCC-AIRO-AIOM 2012)
Clinical question considered, but TMs not addressed (NICE 2015, ESMO 2012)
Serum Tg levels can be elevated in most thyroid diseases and are an insensitive and nonspecific test for thyroid cancer (ATA 2009)
Pre-Operative workup
3
3
Routine pre-operative measurement of serum Tg is not recommended (ATA 2009, BTA 2014)
Serum Tg measurement may be useful to detect potential false-negative values due to decreased Tg immunoreactivity or heterophilic antibodies (AACE-AME-ETAM 2010)
In case of suspicious US features of a lymph node, the metastatic nature of the node may be confirmed with measurement of Tg in the washout of the needle used for UGFNA biopsy (AACE-AME-ETAM 2010)
There is limited evidence that high pre-operative concentrations of serum Tg may predict a higher sensitivity for postoperative surveillance with serum Tg (ATA 2009)
Markers indicated for differentiated thyroid carcinoma: Tg, TgAb (AIOCC-AIRO-AIOM 2012)
Clinical question considered, but TMs not addressed (ESMO 2012, NCCN 2015)
Reassessment after initial curative treatment
2
3
Baseline postoperative serum Tg should be checked, preferably no earlier than 6 weeks after surgery or RRA (BTA 2014, AIOCC-AIRO-AIOM 2012, ESMO 2012, NCCN 2015)
To verify the absence of residual disease, serum Tg should be measured after thyroxine withdrawal or rhTSH stimulation approximately 12 months after ablation (ATA 2009, BTA 2014)
Following total thyroidectomy and RRA, and before evaluation of the patient's response to treatment after 9-12 months, TSH should be suppressed to below 0.1 mU/L (BTA2014)
In patients who have not undergone RRA who are clinically free of disease and have undetectable suppressed serum Tg and normal neck US, the serum TSH may be allowed to rise to the low normal range (0.3-2 mU/L) (BTA 2014)
TgAb should be measured by a quantitative method simultaneously with measurement of serum Tg. If TgAb are detectable, measurement should be repeated at regular (~6-monthly) intervals (BTA 2014)
TgAb, even if negative, should be measured at follow-up when Tg is measured (ATA 2009, BTA 2014)
For patients who have undergone total thyroidectomy and RRA, 9-12 months post-RRA, allocation to 1 of 3 response groups after dynamic risk stratification (based on stimulated Tg, US and [optionally] nuclear medicine imaging) is recommended (BTA 2014, NCCN 2015)
The degree of TSH suppression to be maintained should be established on the basis of risk categories defined by dynamic risk stratification (ATA 2009, BTA 2014, NCCN 2015)
Low risk: TSH may be allowed to rise to the low-normal range (0.3-2 mU/L)
Intermediate risk: TSH should be maintained between 0.1 and 0.5 mU/L for 5-10 years (then reexamine)
High risk: TSH should be maintained below 0.1 mU/L indefinitely in the absence of specific contraindications
Detectable serum Tg is highly suggestive of thyroid remnant, residual or recurrent tumor (BTA 2014)
Stimulated Tg should be measured on day 5 following the first injection of rhTSH (BTA 2014)
A serum TSH concentration >30 mU/L should be achieved to assess stimulated Tg (BTA 2014)
To ensure continuity in monitoring Tg and TgAb assays on a long-term basis, clinicians should use the same laboratory and laboratories should not change methods without prior consultation with clinical users of the service (ATA 2009, BTA 2014)
Tg should be measured by an immunometric assay that is calibrated against the CRM-457 standard (ATA 2009)
Dynamic Risk Stratification
Excellent response (low risk): all the following: (i) suppressed and stimulated Tg <1 μg/L∗, (ii) neck US without evidence of disease, (iii) cross-sectional and/or nuclear medicine imaging negative (if performed)
Intermediate response (intermediate risk): any of the following: (i) suppressed Tg 1 μg/L∗ and stimulated Tg ≥1 and <10 μg/L∗, (ii) neck US with nonspecific changes or stable sub-centimeter lymph nodes, (iii) cross-sectional and/or nuclear medicine imaging with nonspecific changes, although not completely normal
Incomplete response (high risk): any of the following: (i) suppressed Tg≥1 μg/L∗ or stimulated Tg ≥10 μg/L∗, (ii) rising Tg values, (iii) persistent or newly identified disease on cross-sectional and/or nuclear medicine imaging
(NB. ∗Assumes absence of interference in the Tg assay) (BTA 2014)
Early detection of recurrence or progression
2
3
At each visit the following tasks should be completed: determination of Tg and TgAb serum levels; adequacy of TSH suppression; neck US (ATA 2009, BTA 2014, AIOCC-AIRO-AIOM 2012, ESMO 2012, NCCN 2015)
For low-risk patients with no evidence of biochemical or structural disease, annual measurement of serum Tg while on suppressive treatment is adequate (ATA 2009, BTA 2014, AIOCC-AIRO-AIOM 2012)
There is normally no need to measure serum Tg more frequently than 3-monthly during routine follow-up (BTA 2014)
Patients in whom basal Tg remains persistently detectable while on suppressive therapy or rises with subsequent assessments require further evaluation (BTA 2014)
After the first WBS performed following RRA, low-risk patients with undetectable Tg during suppressive therapy with negative TgAb and negative US do not require routine WBS during follow-up (ATA 2009)
A single elevated serum Tg result should be confirmed by repeating the test before proceeding to additional investigation or therapy (BTA 2014)
An elevated serum Tg level should lead to a detailed neck US (BTA 2014)
Serum Tg should be measured every 6-12 months depending on the risk level of the patient (ATA 2009, BTA 2014, AIOCC-AIRO-AIOM 2012, ESMO 2012, NCCN 2015)
TgAb should be measured by a quantitative method simultaneously with measurement of serum Tg. If TgAb are detectable, measurement should be repeated at regular (~6-monthly) intervals (BTA 2014)
TgAb, even if negative, should be measured at follow-up when Tg is measured (ATA 2009, BTA 2014)
Serum TSH concentration should be determined concurrently to aid interpretation (BTA 2014)
To ensure continuity in monitoring, clinicians should use the same laboratory, Tg and TgAb assays on a long-term basis. Laboratories should not change methods without prior consultation with clinical users of the service (ATA 2009, BTA 2014)
Tg should be measured by an immunometric assay that is calibrated against the CRM-457 standard (ATA 2009)
Monitoring of treatment response in advanced disease
2
1
In the presence of persistent or metastatic disease, an undetectable serum TSH level (<0.1 mU/L) should be maintained during follow-up (ATA 2009, ESMO 2012)
It is uncertain whether empirical 131I treatment is beneficial in patients with raised serum Tg, compared to active surveillance (BTA 2014)
Recommendations from CPGs and from OGDs, if consistent with those of CPGs.
Supplementary information from both CPGs and OGDs, and recommendations from OGDs that are inconsistent with those of CPGs.
rhTSH = recombinant human TSH; RRA = 131I radioiodine remnant ablation; UGFNA = ultrasound-guided fine-needle aspiration; US = ultrasound; WBS = 131I whole body scan.
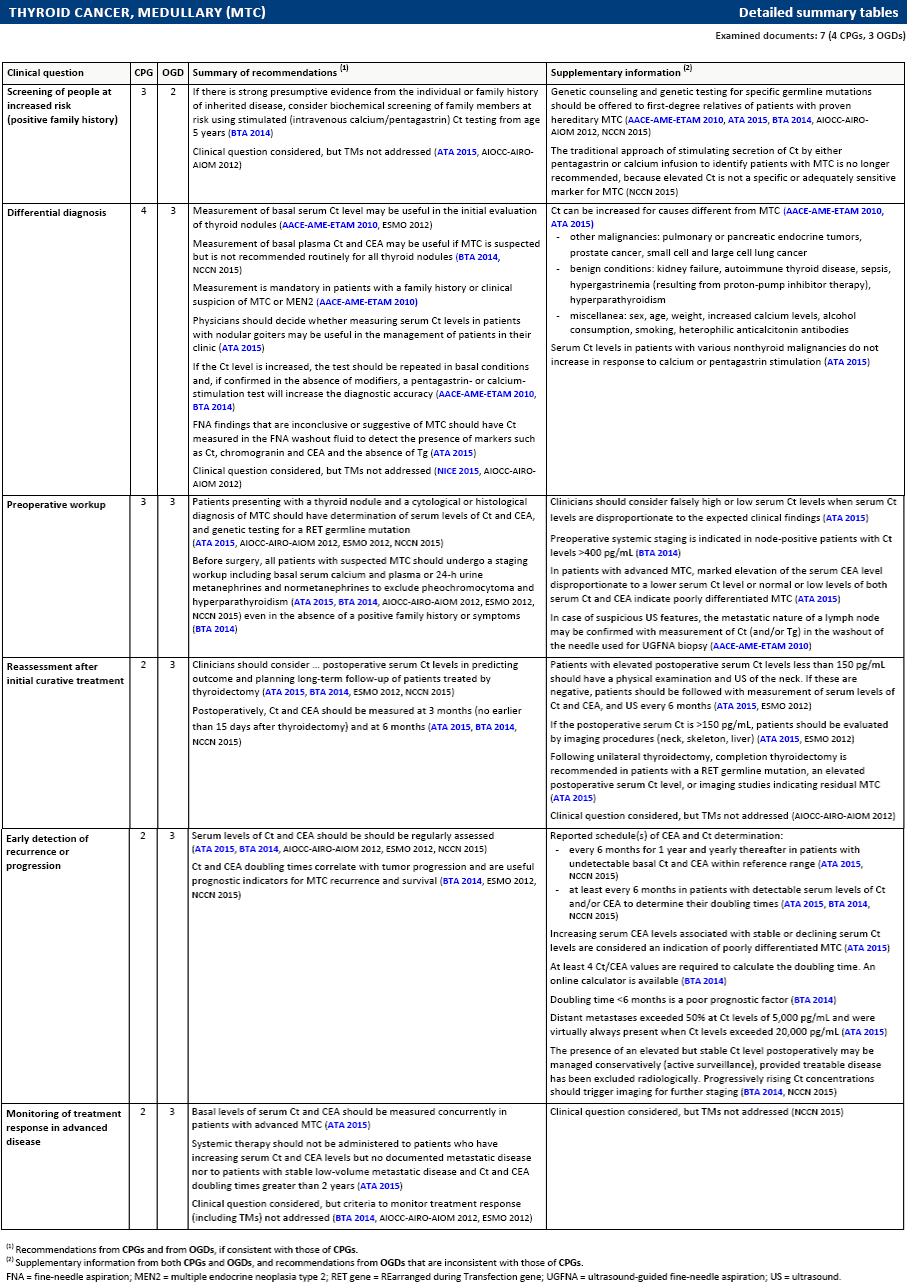
Screening of people at increased risk (positive family history)
3
2
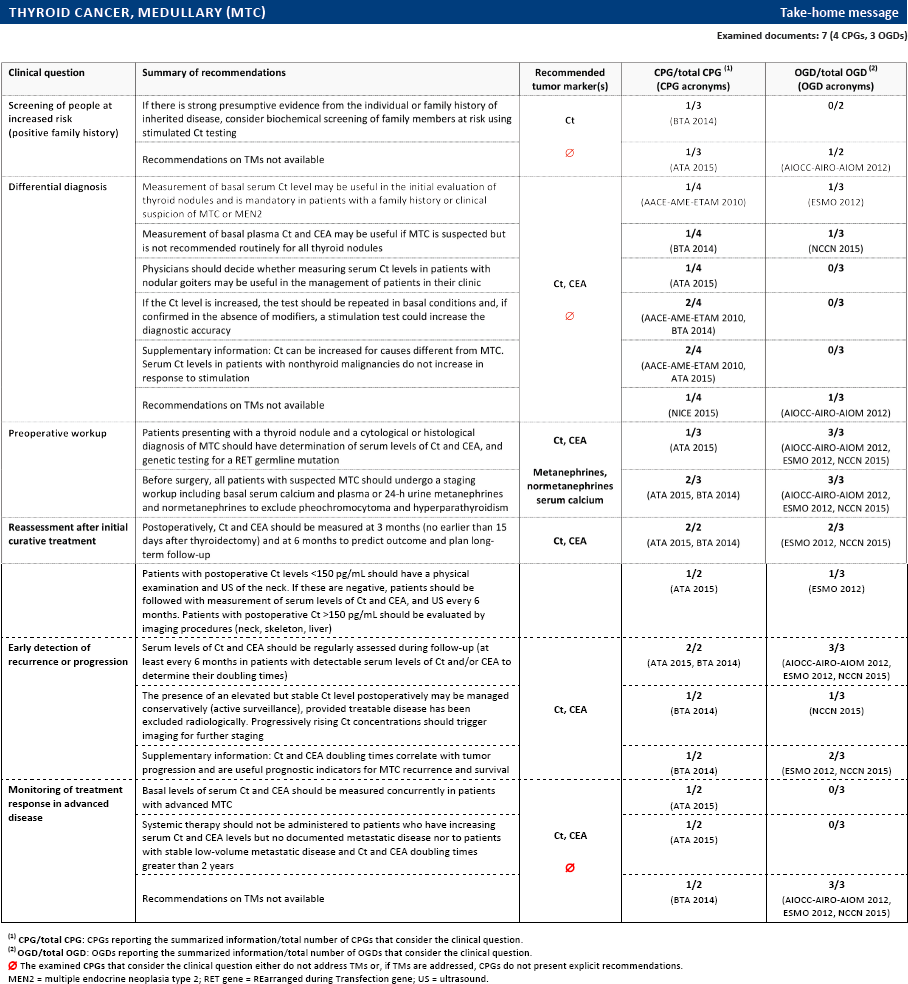
If there is strong presumptive evidence from the individual or family history of inherited disease, consider biochemical screening of family members at risk using stimulated (intravenous calcium/pentagastrin) Ct testing from age 5 years (BTA 2014)
Clinical question considered, but TMs not addressed (ATA 2015, AIOCC-AIRO-AIOM 2012)
Genetic counseling and genetic testing for specific germline mutations should be offered to first-degree relatives of patients with proven hereditary MTC (AACE-AME-ETAM 2010, ATA 2015, BTA 2014, AIOCC-AIRO-AIOM 2012, NCCN 2015)
The traditional approach of stimulating secretion of Ct by either pentagastrin or calcium infusion to identify patients with MTC is no longer recommended, because elevated Ct is not a specific or adequately sensitive marker for MTC (NCCN 2015)
Differential diagnosis
4
3
Measurement of basal serum Ct level may be useful in the initial evaluation of thyroid nodules (AACE-AME-ETAM 2010, ESMO 2012)
Measurement of basal plasma Ct and CEA may be useful if MTC is suspected but is not recommended routinely for all thyroid nodules (BTA 2014, NCCN 2015)
Measurement is mandatory in patients with a family history or clinical suspicion of MTC or MEN2 (AACE-AME-ETAM 2010)
Physicians should decide whether measuring serum Ct levels in patients with nodular goiters may be useful in the management of patients in their clinic (ATA 2015)
If the Ct level is increased, the test should be repeated in basal conditions and, if confirmed in the absence of modifiers, a pentagastrin- or calcium-stimulation test will increase the diagnostic accuracy (AACE-AME-ETAM 2010, BTA 2014)
FNA findings that are inconclusive or suggestive of MTC should have Ct measured in the FNA washout fluid to detect the presence of markers such as Ct, chromogranin and CEA and the absence of Tg (ATA 2015)
Clinical question considered, but TMs not addressed (NICE 2015, AIOCC-AIRO-AIOM 2012)
Ct can be increased for causes different from MTC (AACE-AME-ETAM 2010, ATA 2015)
other malignancies: pulmonary or pancreatic endocrine tumors, prostate cancer, small cell and large cell lung cancer
Serum Ct levels in patients with various nonthyroid malignancies do not increase in response to calcium or pentagastrin stimulation (ATA 2015)
Pre-Operative workup
3
3
Patients presenting with a thyroid nodule and a cytological or histological diagnosis of MTC should have determination of serum levels of Ct and CEA, and genetic testing for a RET germline mutation (ATA 2015, AIOCC-AIRO-AIOM 2012, ESMO 2012, NCCN 2015)
Before surgery, all patients with suspected MTC should undergo a staging workup including basal serum calcium and plasma or 24-h urine metanephrines and normetanephrines to exclude pheochromocytoma and hyperparathyroidism (ATA 2015, BTA 2014, AIOCC-AIRO-AIOM 2012, ESMO 2012, NCCN 2015) even in the absence of a positive family history or symptoms (BTA 2014)
Clinicians should consider falsely high or low serum Ct levels when serum Ct levels are disproportionate to the expected clinical findings (ATA 2015)
Pre-Operative systemic staging is indicated in node-positive patients with Ct levels >400 pg/mL (BTA 2014)
In patients with advanced MTC, marked elevation of the serum CEA level disproportionate to a lower serum Ct level or normal or low levels of both serum Ct and CEA indicate poorly differentiated MTC (ATA 2015)
In case of suspicious US features, the metastatic nature of a lymph node may be confirmed with measurement of Ct (and/or Tg) in the washout of the needle used for UGFNA biopsy (AACE-AME-ETAM 2010)
Reassessment after initial curative treatment
2
3
Clinicians should consider … postoperative serum Ct levels in predicting outcome and planning long-term follow-up of patients treated by thyroidectomy (ATA 2015, BTA 2014, ESMO 2012, NCCN 2015)
Postoperatively, Ct and CEA should be measured at 3 months (no earlier than 15 days after thyroidectomy) and at 6 months (ATA 2015, BTA 2014, NCCN 2015)
Patients with elevated postoperative serum Ct levels less than 150 pg/mL should have a physical examination and US of the neck. If these are negative, patients should be followed with measurement of serum levels of Ct and CEA, and US every 6 months (ATA 2015, ESMO 2012)
If the postoperative serum Ct is >150 pg/mL, patients should be evaluated by imaging procedures (neck, skeleton, liver) (ATA 2015, ESMO 2012)
Following unilateral thyroidectomy, completion thyroidectomy is recommended in patients with a RET germline mutation, an elevated postoperative serum Ct level, or imaging studies indicating residual MTC (ATA 2015)
Clinical question considered, but TMs not addressed (AIOCC-AIRO-AIOM 2012)
Early detection of recurrence or progression
2
3
Serum levels of Ct and CEA should be should be regularly assessed (ATA 2015, BTA 2014, AIOCC-AIRO-AIOM 2012, ESMO 2012, NCCN 2015)
Ct and CEA doubling times correlate with tumor progression and are useful prognostic indicators for MTC recurrence and survival (BTA 2014, ESMO 2012, NCCN 2015)
Reported schedule(s) of CEA and Ct determination:
every 6 months for 1 year and yearly thereafter in patients with undetectable basal Ct and CEA within reference range (ATA 2015, NCCN 2015)
at least every 6 months in patients with detectable serum levels of Ct and/or CEA to determine their doubling times (ATA 2015, BTA 2014, NCCN 2015)
Increasing serum CEA levels associated with stable or declining serum Ct levels are considered an indication of poorly differentiated MTC (ATA 2015)
At least 4 Ct/CEA values are required to calculate the doubling time. An online calculator is available (BTA 2014)
Doubling time <6 months is a poor prognostic factor (BTA 2014)
Distant metastases exceeded 50% at Ct levels of 5,000 pg/mL and were virtually always present when Ct levels exceeded 20,000 pg/mL (ATA 2015)
The presence of an elevated but stable Ct level postoperatively may be managed conservatively (active surveillance), provided treatable disease has been excluded radiologically. Progressively rising Ct concentrations should trigger imaging for further staging (BTA 2014, NCCN 2015)
Monitoring of treatment response in advanced disease
2
3
Basal levels of serum Ct and CEA should be measured concurrently in patients with advanced MTC (ATA 2015)
Systemic therapy should not be administered to patients who have increasing serum Ct and CEA levels but no documented metastatic disease nor to patients with stable low-volume metastatic disease and Ct and CEA doubling times greater than 2 years (ATA 2015)
Clinical question considered, but criteria to monitor treatment response (including TMs) not addressed (BTA 2014, AIOCC-AIRO-AIOM 2012, ESMO 2012)
Clinical question considered, but TMs not addressed (NCCN 2015)
Recommendations from CPGs and from OGDs, if consistent with those of CPGs.
Supplementary information from both CPGs and OGDs, and recommendations from OGDs that are inconsistent with those of CPGs.
FNA = fine-needle aspiration; MEN2 = multiple endocrine neoplasia type 2; RET gene = REarranged during Transfection gene; UGFNA = ultrasound-guided fine-needle aspiration; US = ultrasound.
Selected guidelines (by cancer site)
Head and neck cancer
ADA 2010. Rethman MP, Carpenter W, Cohen EE, et al. Evidence-based clinical recommendations regarding screening for oral squamous cell carcinomas. J Am Dent Assoc. 2010; 141(5):509-20.
AHS 2013. Alberta Provincial Head and Neck Tumour Team. Nasopharyngeal cancer treatment. Edmonton, Alberta: CancerControl Alberta; 2013.
AIOCC-AIRO-AIOM 2012. AIOCC, AIOM, Gruppo di Studio AIRO Testa-collo. Tumori della testa e collo: algoritmi diagnostico-terapeutici AIOCC-AIRO-AIOM – versione 2 (aprile) 2012. www.radioterapiaitalia.it.
AIOM 2015. Associazione Italiana di Oncologia Medica (AIOM). Tumori della testa e del collo. Milano, IT: Associazione Italiana di Oncologia Medica (AIOM); 2015.
CCO 2009. Gilbert R, Devries-Aboud M, Winquist E, Waldron J, McQuestion M; Head and Neck Disease Site Group. The management of head and neck cancer in Ontario. Toronto, ON: Cancer Care Ontario; 2009.
ESMO-EHNS-ESTRO 2010-SCC. Grégoire V, Lefebvre JL, Licitra L, Felip E; EHNS-ESMO-ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010; 21(Suppl 5):v184-6. doi: 10.1093/annonc/mdq185.
ESMO-EHNS-ESTRO 2012-NPC. Chan AT, Grégoire V, Lefebvre JL, et al. Nasopharyngeal cancer: EHNS-ESMO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23(Suppl 7):vii83-5.
NCCN 2015. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Head and neck cancers, version 1.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NICE 2015. National Collaborating Centre for Cancer. Suspected cancer: recognition and referral. London, UK: National Institute for Health and Care Excellence; 2015. https://www.nice.org.uk/guidance/ng12.
USPSTF 2013. Moyer VA; U.S. Preventive Services Task Force. Screening for oral cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(1):55-60. doi: 10.7326/M13-2568.
AHS 2012-NSCLC.s3. Alberta Provincial Thoracic Tumour Team. Non-small cell lung cancer stage III. Edmonton, Alberta: Alberta Health Services, Cancer Care; 2012.
AHS 2012-SCLC.es. Alberta Provincial Thoracic Tumour Team. Small cell lung cancer - extensive stage. Edmonton, Alberta: CancerControl Alberta; 2012.
AHS 2012-SCLC.ls. Alberta Provincial Thoracic Tumour Team. Small cell lung cancer - limited stage. Edmonton, Alberta: CancerControl Alberta; 2012.
AHS 2013-NSCLC.s4. Alberta Provincial Thoracic Tumour Team. Non-small cell lung cancer stage IV. Edmonton, Alberta: CancerControl Alberta; 2013.
AHS 2014-NSCLC.s1. Alberta Provincial Thoracic Tumour Team. Non small cell lung cancer stage I. Edmonton, Alberta: Alberta Health Services, Cancer Care; 2014.
AHS 2014-NSCLC.s2. Alberta Provincial Thoracic Tumour Team. Non-small cell lung cancer stage II. Edmonton, Alberta: Alberta Health Services, Cancer Care; 2014.
AIOM 2015. Associazione Italiana di Oncologia Medica (AIOM). Neoplasie del polmone. Milano, IT: Associazione Italiana di Oncologia Medica (AIOM); 2015.
AIOT 2012-NSCLC. Gridelli C, de Marinis F, Di Maio M, et al. Maintenance treatment of advanced non-small-cell lung cancer: results of an International Expert Panel Meeting of the Italian Association of Thoracic Oncology. Lung Cancer. 2012; 76(3):269-79. doi: 10.1016/j.lungcan.2011.12.011.
ASCO 2015-NSCLC.s4. Masters GA, Temin S, Azzoli CG, et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2015; 33(30):3488-515. doi: 10.1200/JCO.2015.62.1342.
ASCO 2015-SCLC. Rudin CM, Ismaila N, Hann CL, et al. Treatment of small-cell lung cancer: American Society of Clinical Oncology endorsement of the American College of Chest Physicians guideline. J Clin Oncol. 2015; 33(34):4106-11. doi: 10.1200/JCO.2015.63.7918.
BTS-SCTS 2010. Lim E, Baldwin D, Beckles M, et al. Guidelines on the radical management of patients with lung cancer. Thorax. 2010;65(Suppl 3):iii1-27. doi: 10.1136/thx.2010.145938.
CCO 2014-dia. Del Giudice L, Young S, Vella E, et al. Referral of suspected lung cancer by family physicians and other primary care providers. Toronto, ON: Cancer Care Ontario; 2011. Validity verification: 2014.
CCO 2014-fu. Ung YC, Souter LH, Darling G, et al. Follow-up and surveillance of curatively treated lung cancer patients. Toronto, ON: Cancer Care Ontario (CCO); 2014.
CCO 2014-NSCLC.m+. Lung Cancer Disease Site Group (DSG). First-line systemic chemotherapy in the treatment of advanced non-small cell lung cancer. Goffin J, Poon R. Reviewers. Toronto, ON: Cancer Care Ontario; 2010. Validity verification: 2014.
CECOG 2012-NSCLC. Brodowicz T, Ciuleanu T, Crawford J, et al. Third CECOG consensus on the systemic treatment of non-small-cell lung cancer. Ann Oncol. 2012; 23(5):1223-9. doi: 10.1093/annonc/mdr381.
ELCWP 2012. Berghmans T, Pasleau F, Paesmans M, et al. Surrogate markers predicting overall survival for lung cancer: ELCWP recommendations. Eur Respir J. 2012; 39(1):9-28. doi: 10.1183/09031936.00190310.
ESMO 2013-NSCLC. Vansteenkiste J, De Ruysscher D, Eberhardt WE, et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013; 24(Suppl 6):vi89-98. doi: 10.1093/annonc/mdt241.
ESMO 2014 (a). Vansteenkiste J, Crinò L, Dooms C, et al. 2nd ESMO Consensus Conference on Lung Cancer: early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann Oncol. 2014; 25(8):1462-74. doi: 10.1093/annonc/mdu089.
ESMO 2014 (b). Eberhardt WE, De Ruysscher D, Weder W, et al. 2nd ESMO Consensus Conference in Lung Cancer: locally advanced stage III non-small-cell lung cancer. Ann Oncol. 2015;26(8):1573-88. doi: 10.1093/annonc/mdv187.
ESMO 2014 (c). Besse B, Adjei A, Baas P, Meldgaard P, et al. 2nd ESMO Consensus Conference on Lung Cancer: non-small-cell lung cancer first-line/second and further lines of treatment in advanced disease. Ann Oncol. 2014;25(8):1475-84. doi: 10.1093/annonc/mdu123.
ESMO 2014 (d). Kerr KM, Bubendorf L, Edelman MJ, et al. Second ESMO Consensus Conference on Lung Cancer: pathology and molecular biomarkers for non-small-cell lung cancer. Ann Oncol. 2014;25(9):1681-90. doi: 10.1093/annonc/mdu145.
ESMO 2014-NSCLC.m+. Reck M, Popat S, Reinmuth N, et al. Metastatic non-small-cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014; 25(Suppl 3):iii27-39. doi: 10.1093/annonc/mdu199.
ESMO-JSMO 2013-SCLC. Früh M, De Ruysscher D, Popat S, et al. Small-cell lung cancer (SCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013; 24(Suppl 6):vi99-105. doi: 10.1093/annonc/mdt178.
FS 2013. Naidich DP, Bankier AA, MacMahon H, et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: a statement from the Fleischner Society. Radiology. 2013; 266(1):304-17. doi: 10.1148/radiol.12120628.
NCCN 2015-NSCLC. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Non-small cell lung cancer, version 5.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NCCN 2015-SCLC. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Small cell lung cancer, version 1.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NCCN 2015-scr. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Lung cancer screening, version 2.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NICE 2011. National Collaborating Centre for Cancer. Lung cancer. The diagnosis and treatment of lung cancer. London, UK: National Institute for Health and Clinical Excellence (NICE); 2011. https://www.nice.org.uk/guidance/cg121.
NICE 2015-dia. National Collaborating Centre for Cancer. Suspected cancer: recognition and referral. London, UK: National Institute for Health and Care Excellence; 2015. https://www.nice.org.uk/guidance/ng12.
SIGN 2014. Scottish Intercollegiate Guidelines Network (SIGN). Management of lung cancer. A national clinical guideline. Edinburgh, Scotland: Scottish Intercollegiate Guidelines Network (SIGN); 2014. http://www.sign.ac.uk/guidelines/fulltext/137/index.html.
USPSTF 2014-scr. Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014; 160(5):330-8. doi: 10.7326/M13-2771.
Melanoma
ACCC 2012. Dutch Working Group on Melanoma. Melanoma - version: 2.0. Utrecht, The Netherlands: Association of Comprehensive Cancer Centres; 2012.
AHS 2013-FU. Alberta Provincial Cutaneous Tumour Team. Referral and follow-up surveillance of cutaneous melanoma. Edmonton, Alberta: CancerControl Alberta; 2013.
AHS 2013-PROP. Alberta Provincial Cutaneous Tumour Team. Pre-Operative and pretreatment investigations for malignant melanoma. Edmonton, Alberta: CancerControl Alberta; 2013.
AHS 2015-URM. Alberta Provincial Cutaneous Tumour Team. Systemic therapy for unresectable stage III or metastatic cutaneous melanoma. Edmonton, AB: CancerControl Alberta; 2015.
AIOM 2015. Associazione Italiana di Oncologia Medica (AIOM). Melanoma. Milano, IT: AIOM; 2015.
BAD 2010. Marsden JR, Newton-Bishop JA, Burrows L, et al. Revised U.K. guidelines for the management of cutaneous melanoma 2010. Br J Dermatol. 2010; 163(2):238-56. doi: 10.1111/j.1365-2133.2010.09883.x.
EDF-EADO-EORTC 2012. Garbe C, Peris K, Hauschild A, et al. Diagnosis and treatment of melanoma. European consensus-based interdisciplinary guideline–Update 2012. Eur J Cancer. 2012; 48(15):2375-90. doi: 10.1016/j.ejca.2012.06.013.
ESMO 2012. Dummer R, Hauschild A, Guggenheim M, et al. Cutaneous melanoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012; 23(Suppl 7):vii86-91.
NCCN 2015. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Melanoma, version 3.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NICE 2015-ME. National Collaborating Centre for Cancer. Melanoma: assessment and management. London, UK: National Institute for Health and Care Excellence (NICE); 2015. http://www.nice.org.uk/guidance/ng14.
NICE 2015-SC. National Collaborating Centre for Cancer. Suspected cancer: recognition and referral. London, UK: National Institute for Health and Care Excellence; 2015. https://www.nice.org.uk/guidance/ng12.
SIDeMaST 2011. Società Italiana di Dermatologia Medica, Chirurgica, Estetica e delle Malattie Sessualmente Trasmesse. Linee guida e raccomandazioni SIDeMaST. Pisa: Pacini Editore; 2011.
AHS 2012. Alberta Provincial Thoracic Malignancies Tumour Team. Malignant pleural mesothelioma. Edmonton, Alberta: CancerControl Alberta; 2012.
AHS 2014-MPE. Alberta Provincial Lung Tumour Team. Malignant pleural effusion. Edmonton, Alberta: CancerControl Alberta; 2014.
BTS 2010-MPE. BTS Pleural Disease Guideline Group. British Thoracic Society pleural disease guideline 2010. Thorax. 2010; 65(Suppl 2):ii1-76.
ERS-ESTS 2010. Scherpereel A, Astoul P, Baas P, et al. Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma. Eur Respir J. 2010; 35(3):479-95. doi: 10.1183/09031936.00063109.
ESMO 2010. Stahel RA, Weder W, Lievens Y, Felip E; ESMO Guidelines Working Group. Malignant pleural mesothelioma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010; 21(Suppl 5):v126-8. doi: 10.1093/annonc/mdq173.
imp 2013. Pinto C, Novello S, Torri V, et al. Second Italian consensus conference on malignant pleural mesothelioma: state of the art and recommendations. Cancer Treat Rev. 2013; 39(4):328-39. doi: 10.1016/j.ctrv.2012.11.004.
NCCN 2015. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Malignant pleural mesothelioma, version 1.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NICE 2015. National Collaborating Centre for Cancer. Suspected cancer: recognition and referral. London, UK: National Institute for Health and Care Excellence; 2015. https://www.nice.org.uk/guidance/ng12.
Thyroid cancer, differentiated
AACE-AME-ETAM 2010. Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2010; 16(Suppl 1):1-43. doi: 10.4158/10024.GL.
AIOCC-AIRO-AIOM 2012. AIOCC, AIOM, Gruppo di Studio AIRO Testa-collo. Tumori della testa e collo: algoritmi diagnostico-terapeutici AIOCC-AIRO-AIOM, versione 2 (aprile) 2012. www.radioterapiaitalia.it.
ATA 2009. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167-214. doi: 10.1089/thy.2009.0110.
BTA 2014. Perros P, Boelaert K, Colley S, et al. Guidelines for the management of thyroid cancer. Clin Endocrinol (Oxf). 2014; 81(Suppl 1):1-122. doi: 10.1111/cen.12515.
ESMO 2012. Pacini F, Castagna MG, Brilli L, Pentheroudakis G; ESMO Guidelines Working Group. Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012; 23(Suppl 7):vii110-9.
NCCN 2015. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Thyroid carcinoma, version 2.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NICE 2015. National Collaborating Centre for Cancer. Suspected cancer: recognition and referral. London, UK: National Institute for Health and Care Excellence; 2015. https://www.nice.org.uk/guidance/ng12.
Thyroid cancer, medullary
AACE-AME-ETAM 2010. Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2010; 16(Suppl 1):1-43. doi: 10.4158/10024.GL.
AIOCC-AIRO-AIOM 2012. AIOCC, AIOM, Gruppo di Studio AIRO Testa-collo. Tumori della testa e collo: algoritmi diagnostico-terapeutici AIOCC-AIRO-AIOM, versione 2 (aprile) 2012. www.radioterapiaitalia.it.
ATA 2015. Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015; 25(6):567-610. doi: 10.1089/thy.2014.0335.
BTA 2014. Perros P, Boelaert K, Colley S, et al. Guidelines for the management of thyroid cancer. Clin Endocrinol (Oxf). 2014; 81(Suppl 1):1-122. doi: 10.1111/cen.12515.
ESMO 2012. Pacini F, Castagna MG, Brilli L, Pentheroudakis G; ESMO Guidelines Working Group. Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012; 23(Suppl 7):vii110-9.
NCCN 2015. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Thyroid carcinoma, version 2.2015. Fort Washington, PA: National Comprehensive Cancer Network; 2015.
NICE 2015. National Collaborating Centre for Cancer. Suspected cancer: recognition and referral. London, UK: National Institute for Health and Care Excellence; 2015. https://www.nice.org.uk/guidance/ng12.
Contributors
Salvatore Alfieri
SC Oncologia Medica 3 Tumori Testa e Collo
Fondazione IRCCS Istituto Nazionale dei Tumori
Milano - Italy
Emiliano Aroasio
Dipartimento di Scienze Cliniche e Biologiche
Azienda Ospedaliero-Universitaria San Luigi Gonzaga
Orbassano (Torino) - Italy
Alessandro Bertaccini
Clinica Urologica
Azienda Ospedaliero-Universitaria di Bologna Policlinico S. Orsola-Malpighi
Bologna - Italy
Francesco Boccardo
UOC Clinica di Oncologia Medica
IRCCS AOU San Martino IST - Istituto Nazionale per la Ricerca sul Cancro
Università degli Studi
Genova - Italy
Mario Braga
Sistema Monitoraggio Nazionale (Area Monitoraggio Spesa Sanitaria e LEA)
Agenzia Nazionale per i Servizi Sanitari Regionali (AGENAS)
Roma - Italy
Roberto Buzzoni
SC Day Hospital e Terapia Ambulatoriale Oncologica Fondazione IRCCS Istituto Nazionale dei Tumori Milano - Italy
Maurizio Cancian
Società Italiana di Medicina Generale SIMG
Scuola Veneta di Medicina Generale SVeMG
Conegliano Veneto (Treviso) - Italy
Ettore D. Capoluongo
UOS Diagnostica Molecolare Clinica e Personalizzata, Dipartimento di Medicina Laboratorio
Centro e Programma Regionale Biomarcatori Diagnostici, Prognostici e Predittivi
Azienda ULSS 12 Veneziana
AVAPO Venezia Onlus
Venezia - Italy
Vincenzo Scattoni
UO Urologia
IRCCS Ospedale San Raffaele
Università Vita-Salute San Raffaele
Milano - Italy
Holger Schünemann
Department of Clinical Epidemiology & Biostatistics
McMaster University Health Sciences Centre
Hamilton - Canada
Giuseppe Sica
UOC Chirurgia Generale A, Dipartimento di Chirurgia
Fondazione PTV Policlinico Universitario Tor Vergata Università Roma-Tor Vergata
Roma - Italy
Alessandro Terreni
SOD Laboratorio Generale
AOUC Azienda Ospedaliero-Universitaria Careggi
Firenze - Italy
Marcello Tiseo
SC Oncologia Medica
Azienda Ospedaliero-Universitaria
Parma - Italy
Valter Torri
Laboratorio Metodologia per la Ricerca Biomedica, Dipartimento Oncologia
IRCCS Istituto di Ricerche Farmacologiche “Mario Negri” Milano - Italy
Quinto Tozzi
Ricerca e Studio Rischio Clinico
Agenzia Nazionale per i Servizi Sanitari Regionali (AGENAS)
Roma - Italy
Tommaso Trenti
Dipartimento Integrato Interaziendale di Medicina di Laboratorio ed Anatomia Patologica
Azienda Ospedaliera Universitaria e Azienda USL di Modena
Modena - Italy
Chiara Trevisiol
Centro e Programma Regionale Biomarcatori Diagnostici, Prognostici e Predittivi
Azienda ULSS 12 Veneziana
Istituto Oncologico Veneto IOV – IRCCS
Padova - Italy
Paolo Zola
Dipartimento Scienze Chirurgiche
AOU Città della Salute e della Scienza
Università degli Studi
Torino - Italy
Footnotes
Acknowledgments
The authors would like to thank the following researchers for their collaboration: Mauro Antimi (Roma), Alessandro Battaggia (Padova), Nicola L. Bragazzi (Genova), Massimo Brunetti (Modena), Michele Cannone (Canosa di Puglia), Antonette E. Leon (Venezia).
Acronyms
Abbreviations of tumor markers cited in the present article
References
1.
GionM., TrevisiolC., RainatoG., FabricioA.S.C.Marcatori circolanti in oncologia: guida all'uso clinico appropriato. I Quaderni di Monitor.Roma: AGENAS, Agenzia Nazionale per i Servizi Sanitari Regionali2016.
2.
GionM., TrevisiolC., RutjesA.W.S., RainatoG., FabricioA.S.C.Circulating tumor markers: a guide to their appropriate clinical use. Comparative summary of recommendations from clinical practice guidelines (Part 1). Int J Biol Markers.2016; 31: e332–e367.
3.
GionM., TrevisiolC., RutjesA.W.S., RainatoG., FabricioA.S.C.Circulating tumor markers: a guide to their appropriate clinical use. Comparative summary of recommendations from clinical practice guidelines (Part 2). Int J Biol Markers.2017; 32: e1–e52.
4.
GionM.Need for knowledge translation to improve tumor marker application. Int J Biol Markers.2016; 31: e331.
5.
IOM (Institute of Medicine).Clinical practice guidelines we can trust.Washington, DC: The National Academies Press2011.