
Abstract
Introduction
Emergency transplantation of a donor liver that is not matched for the major blood antigens can produce marked immune-mediated cytokine release that can cause donor graft loss. Control of the inflammatory response may be a key element in treatment.
Methods
We present the case of a 46-year-old man with primary graft nonfunction after liver transplantation who underwent emergency retransplantation with an ABO-incompatible graft. A severe inflammatory response syndrome (SIRS) was noted in the perioperioperative period of retransplantation. The patient was successfully treated for this condition with a new hemoadsorption column (CytoSorb®), in combination with continuous venovenous hemofiltration (CVVH) throughout the intraoperative and early postoperative period.
Results
During and after each treatment a significant and rapid decrease of pro- and anti-inflammatory cytokines was observed, especially for interleukin-6 (IL-6), IL-10 and monocyte chemotactic protein 1 (MCP-1). Reduction of cytokines was associated with normalization of cardiac output and systemic vascular resistance, and improved liver function.
Conclusions
We believe this is the first case in which hemoadsorptionin combination with CVVH has been used to manage SIRS in a patient with primary graft nonfunction undergoing emergency retransplantation.
Keywords
Introduction
Primary graft nonfunction (PGN) represents a severe and life-threatening complication following liver transplantation (LT). Although there are several definitions, it is accepted as graft function insufficient to sustain life and leading to death or retransplantation (rLT) in the first week after LT (1). Increased donor age and a high model for end-stage liver disease (MELD) score remain the main risk factors for PGN (2). Although retransplantation is the only therapeutic option for PGN, there are few accepted interventions that are capable of bridging patients until a liver graft is available (3).
The inflammatory response following ischemia-reperfusion (l-R) injury during LT has been well documented but there are few therapeutic options for minimizing organ injury (4). Cytokine release plays a crucial role in the pathogenesis of PGN and multiple organ dysfunction (5), leading to cardiovascular instability, respiratory distress and renal failure. Investigators have described several techniques to reduce the deleterious effects of the immune response in PGN and ABO-incompatible transplant but none of these methods have been extensively evaluated in a patient cohort (6).
We developed a different approach, reasoning that if we could control the plasma levels of cytokines, organ injury in this setting could be minimized. We therefore chose a novel method that used a hemoadsorption column (CytoSorb®; CytoSorbents Europe) in combination with standard continuous venovenous hemofiltration (CVVH). The efficacy of the technique was evaluated by measuring the serum levels of cytokines and examining the association with the clinical condition of the patient.
Case presentation
A 46-year-old male with alcohol-induced cirrhosis and hepatitis B virus (MELD score 27 and MELD-Na 30) received a liver graft from a 77-year-old cadaveric donor with a donor risk index of 2.106 (Custodiol® HTK solution; Essential Pharmaceuticals). Cold ischemic time was 6.5 hours and warm ischemic time was 30 minutes. Duration of surgery was 270 minutes, using total vascular exclusion for 30 minutes. Blood loss was 6000 mL, requiring transfusion of 12 units of packed red blood cells, 9 units of fresh frozen plasma, 6 units of platelets, 1 g tranexamic acid and 3 g of fibrinogen concentrate. Severe postreperfusion syndrome occurred (bradycardia 25 beats/ min) requiring administration of 3 mg of atropine. The maximum dose of vasopressor (noradrenaline) was 1.8 μg/kg per min and it was discontinued at the end of surgery. Immunosuppression was administered according to our local protocol: methylprednisolone 500 mg IV during the anhepatic phase, induction with basiliximab 20 mg IV during the neohepatic phase, followed by mycophenolatemofetil 1 g twice daily.
Postoperatively, the patient remained neurologically unresponsive and could not be extubated. There was an increase in serum transaminases (up to 4550 U/L) and bilirubin (up to 45.8 mg/dL) in the first postoperative day. A hyperdynamic hemodynamic status with a high cardiac index (CI) 6.29 L/min per m2 and low systemic vascular resistance index (SVRI) 850 dyne*s*cm−5*m2 requiring vasopressor support was noted immediately after surgery. Laboratory results showed disseminated intravascular coagulation (high concentration of fibrin degradation products, D-dimers > 20.000 μg/L, factor II 27%, factor V 20%, factor VII 12%, factor X 29%). One session of plasma exchange was performed for severe coagulopathy and cholestasis. The procedure was performed on MultiFitrate® (Fresenius Medical Care Deutschland) using a plasmaFlux® P2 dry filter. The total plasma volume exchanged was 4000 mL (50 mL/kg) and a multiBic® potassium-free solution was used as replacement fluid. No anticoagulation was applied during this procedure. The patient was relisted for emergency rLT and an ABO-incompatible graft became available within 48 hours (A positive graft to B positive recipient, Donor risk index 2.25) (Fig. 1A, B). The duration of surgery was 290 minutes. The intraoperative blood loss was 3,000 mL, requiring a blood transfusion of 3 units of PRBc and 4 units of FFP. Three grams of fibrinogen concentrate and 1 g tranexamic acid were also administered. Of note, most of the blood loss (2,500 mL) occurred during the preanhepatic phase, hence PRBc and FFP were administered only during this time. Intraoperative immunosuppresion consisted of 500 mg metilprednisolone and 20 mg basiliximab. The maximum dose of vasopressor (noradrenaline) was 2.1 μg/kg per min and was discontinued at the end of surgery and hemodynamic parameters returned to near normal (CI 5.1 l/min/m2, SVRI 956 dyne*s*cm−5*m2).
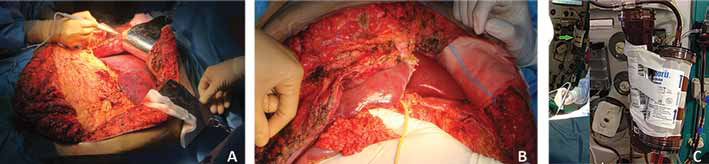
Intraoperative view showing the liver graft before emergency retransplantation (rLT) (
A CVVH treatment combined with a hemoadsorption column (CytoSorb®) was started prior to retransplantation and continued during the procedure, for a total duration of 7 hours. The CVVH procedure was performed on MultiFitrate® using an Ultraflux® AV 600S hemofilter (both from Fresenius Medical Care Deutschland). Normal saline was used as priming solution and multiBic® potassium-free solution was used as substitution fluid. The CVVH prescription was as follows: blood flow 150 mL/min, ultrafiltrate 100 mL/h, substitution of 1500 ml with regional heparin anticoagulation and a predilution of 500 mL/h. The CytoSorb® cartridge was placed upstream of the hemofilter for CVVH (Fig. 1C). The procedure was performed by a femoral vein catheter.
To quantify the effect of CytoSorb® on plasma cytokine levels, blood samples were collected at 3 time points: before starting CVVH (T1), at the end of the anhepatic phase (T2) and at the end of the procedure (T3). Cytokine levels were determined by an immunology multiplex assay (Milliplex MAP Human Cytokine/Chemokine immunoassay panel; Merck Millipore) on a Luminex-200™ System (Luminex).
A change in hemodynamic status occurred 24 hours following retransplantation, with a hyperdynamic pattern (CI 7.2 L/min per m2, SVRI 823 dyne*s*cm−5*m2, central venous pressure 6 mmHg) and vasopressor support was reinitiated (noradrenaline with a maximum dose of 0.88 μg/ kg per min). The patient received a second treatment with CVVH and CytoSorb® for 12 hours. The machine brand and CVVH prescription were the same as in the first treatment. Cytokine levels were measured before (T4) and after (T5) the second treatment (Tab. I). Vasopressor support was discontinued after the second CVVH treatment, hepatic encephalopathy improved and the patient was extubated. One gram of mycophenolatemofetil was administered 12 hours after rLT (14 hours before the second CVVH treatment), but no immunosuppression therapy or blood product transfusion was administered during the second CVVH treatment.
Liver function tests and cytokine levels during the use of CytoSorb® in combination with CVVH
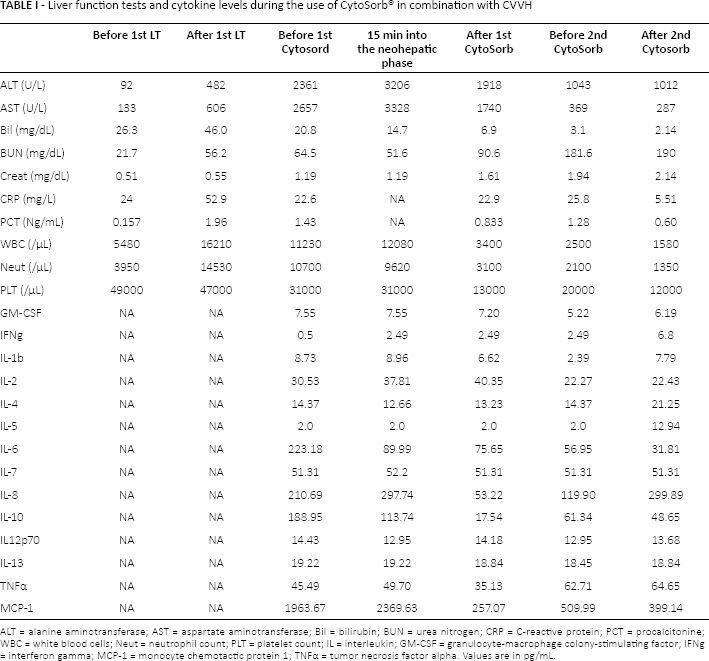
ALT = alanine aminotransferase; AST = aspartate aminotransferase; Bil = bilirubin; BUN = urea nitrogen; CRP = C-reactive protein; PCT = procalcitonine; WBC = white blood cells; Neut = neutrophil count; PLT = platelet count; IL = interleukin; GM-CSF = granulocyte-macrophage colony-stimulating factor; IFNg = interferon gamma; MCP-1 = monocyte chemotactic protein 1; TNFα = tumor necrosis factor alpha. Values are in pg/mL.
The use of CytoSorb® during the second session was associated with an improvement in hemodynamics (CI decreased from 7.2 L/min per m2 to 4.1 L/min per m2, SVRI increased from 823 dyne*s*cm−5*m2 to 1,438 dyne*s*cm−5*m2), normalization of blood lactate levels and an increase in central venous oxygen saturation (ScvO2) to normal values (Fig. 2).
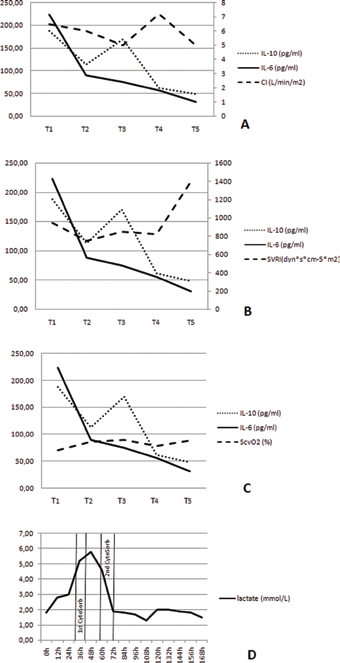
Improvement in hemodynamic parameters observed during the use of CytoSorb®: cardiac index (
During the first treatment of CVVH with CytoSorb®, proinflammatory cytokines: interleukine (IL) -1b, tumor necrosis factor alpha (TNFα), IL-6 and IL-8 levels decreased and anti-inflammatory cytokines IL-4 and IL-13 remained constant and within the normal range. A significant decrease from 10-fold higher than normal to near normal levels of IL-10 and monocyte chemotactic protein 1 (MCP-1) from 10-fold higher than normal to near normal levels was recorded.
A decrease in platelet count was observed during both treatments (attributed to a multifactor etiology: CVVH procedure, use of heparin, intraoperative blood loss, and possibly to the use of a hemoadsorption column). Liver function returned to normal within the next 5 days.
Three plasma exchange sessions were applied after rLT according to our local ABO incompatible protocol (daily determination of isoagglutinin titers, plasma exchange for a level <1:16). The same machine brand, filter and prescription as in the first session were used. Immunosuppression was continued according to our local protocol: 1 g of mycophenolatemofetil twice daily, a repeated dose of 20 mg basiliximab on postoperative day 4 and tacrolimus was started on postoperative day 5.
The patient was discharged from the Postanesthesia Care Unit on postoperative day 7 and from hospital 1 month later with normal liver function. A normal liver function was also recorded at the 1-year follow-up.
Discussion
Our main reason for using CytoSorb® was severe SIRS associated with PGN. Our findings are similar to recent case reports showing a similar effect in patients with septic shock. In their case report on a patient with septic shock due to necrotizing fasciitis, Hetz et al (7) showed a reduction of IL-6 that was associated with a reduction in vasopressor support.
The use of CytoSorb® in combination with CVVH was associated with a positive trend in hemodynamics. This was accompanied by a decrease in proinflammatory cytokines. The cytokines IL-6 and IL-10 were primarily associated with a normalization of hemodynamic parameters (CI and SVRI), a decrease in blood lactate levels and an increase in ScvO2 levels. The use of CytoSorb® during and immediately after emergency rLT may have been responsible for the improvement in clinical outcome observed in our patient. We hypothesize that CytoSorb® reduced cytokine levels produced by the ischemic nonfunctional liver. Investigators do not agree whether both l-R and PGN are associated with an intense immunological response and if this leads to an uncontrolled production of both proinflammatory and anti-inflammatory cytokines responsible for hemodynamic instability, organ failure and severe SIRS (8). Our data show that prior to rLT the levels of proinflammatory cytokines were high, but there was no significant increase during surgery. We attribute this observation to the use of CytoSorb®. We noted the same trend in hemodynamic measurements and cytokine levels following a second session of CVVH with CytoSorb®. The latter provided additional proof of the association between cytokine adsorption and clinical outcome.
In our experience the use of CytoSorb® appeared to dampen the immunological cascade. Our observation suggests a shift from a SIRS state to a more compensated inflammatory response syndrome. Preliminary evidence from our serum measurements suggest that the balance of cytokines may be shifted towards anti-inflammation. However, larger studies with more extensive measures of cytokines are required to confirm this hypothesis. The benefits of CytoSorb® in ABO-incompatible graft remain uncertain and not yet tested in clinical studies. Our reasoning for using CytoSorb® was severe SIRS, not immunological cascade associated with ABO-incompatible liver transplantation, for which plasma exchange was applied according to our local protocol.
Our case presentation has two main limitations. First of all, a significant blood loss and transfusion was noted during the first CytoSorb® therapy during the preanhepatic phase, so that the decrease in cytokine levels observed may be due to the blood volume exchanged during this time. Of note, neither significant blood loss nor transfusion was noted during the rest of the procedure or during the second CytoSorb® therapy; additionally, a continuous decrease in proinflammatory cytokines was observed during this time. Second, CVVH alone can clear cytokines during severe SIRS and sepsis (9). It is difficult to state that the decrease in proinflammatory cytokines was due to the use of CytoSorb® alone. A randomized controlled trial is needed to further assess this issue.
To the authors' knowledge, this is the first reported case in which a hemoadsorption column was used in combination with CVVH to manage severe SIRS in the setting of PGN. The use of CytoSorb® was associated with an excellent outcome in terms of improved hemodynamic parameters, rebalancing proinflammatory and anti- inflammatory cytokines, and patient survival to hospital discharge. The treatment was well tolerated with no obvious adverse effects. A randomized controlled trial is needed to further evaluate efficacy and indications for hemoadsorption in patients with either acute liver failure or chronic liver disease in the perioperative period of LT, especially in patients with severe l-R injury.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.