
Abstract
Purpose
Hernias can be repaired by reinforcement of damaged fascia using biomaterials to provide stabilisation. Repair materials are usually porous, through which cells infiltrate, proliferate and secrete ECM. Their efficacy relies on good tissue integration and resolution of host defence mechanisms. Therefore, understanding the dynamics by which biomaterials interact with tissue will provide knowledge to advance prosthesis design. Furthermore, determining host response in real time would provide significant advantage both clinically and scientifically over the current terminal process of histology.
Methods
3 materials comprising synthetic and composite (synthetic materials hybridised with a resorbable biologic component) meshes were implanted into a rat full-thickness abdominal wall excision model. Their efficacy was evaluated using histopathology whilst also monitoring systemic concentrations of cytokines associated with inflammation and wound healing to predict material outcome over 12 weeks.
Results
The noncomposite material (polyester) and Material B (polypropylene mesh with oligocaprone film and polydioxanone glue) stimulated the largest degree of adhesion from the 3 materials tested, although after 28 days adhesions were stronger to Material B. Histologically, all 3 materials integrated well with abdominal musculature and infiltrated completely with cells.
Conclusions
Analysis of systemic inflammation biomarkers confirmed inflammation elicited by surgeries and meshes irrespective of their composition. However, at an early postoperative endpoint (i.e., 1 week), some biomarkers, namely, IL-18 and RANTES, appeared to discriminate the noncomposite mesh from the composite materials, although in this study all materials successfully repaired the defects without recurrence or external indicators of postoperative chronic pain.
Introduction
Over 800,000 hernias are encountered annually by surgeons in the US alone (1, 2). Repair often involves hernioplasty; restoration of mechanical strength to the weakened fascia using a prosthetic material. Inclusion of a biomaterial is widely acknowledged to be more efficacious than direct fascial abutment or ‘suture repair’, due to the deteriorative condition typically associated with chronically herniated fascia (3). Additionally, suture repair adds a compounding factor in predicting success since yarn material, knot type, running versus interrupted and suture to wound length ratio all impact prognosis (4).
Abdominal hernias are a prevalent defect defined as protrusion of a peritoneal-lined sac through the musculo-aponeurotic covering of the abdomen. Abdominal wall herniorrhaphies are one of the most frequent procedures performed by general surgeons. Although precise incidences are unknown it is estimated 100,000 to 360,000 are treated annually in the US and at any one time 5 million Americans have an abdominal wall hernia (5, 6).
Hernia prostheses should be biocompatible, provide support for defective tissues, maintain tissue elasticity and allow integration of bordering fascial cells with appropriate mechanical properties to confer tissue functionality (7, 8). Historically, these materials are categorised as biologic or synthetic. Biologics are decellularised and/or chemically cross-linked xenogeneic and/or allogeneic tissue, including dermis, pericardium and small intestinal submucosa (9, 10). Biologics are favoured in complex/contaminated hernia where malleability, lack of macro-porosity and persistence in infected fields make them ideal for reconstructing large areas of abdominal wall (11–14). Synthetics are permanent or resorbable, open, porous mesh structures generated from polymers including polypropylene, polyester, poly-lactic acid, polyglycolic acid and polytetrafluoroethylene, varying in knitting pattern, fibre number and configuration. Synthetics are used for small defects or those requiring more intricate repair, such as reconstruction of the inguinal canal (15–19).
Biomaterial augmented tissue repair requires seamless integration between material and tissue, particularly during the inflammatory response: the period during which the body investigates a compromised area to orchestrate a return to normal homeostasis (20). Excessive inflammation results in damage to implanted devices and surrounding tissue by reactive oxygen species and proteolytic enzymes secreted by activated leukocytes (21, 22). However, inflammation is required for healthy wound healing to support material integration, operative site debridement and disinfection. Leukocytes signal to stromal cells via soluble factors, simulating proliferation, infiltration and material stabilisation. Therefore, a thorough understanding of the dynamics with which a material influences inflammatory pathology allows the most patient compliant graft to be selected, which may involve tailoring the prosthesis choice on a patient-by-patient basis (23, 24).
In the incidence of herniorrhaphy, material must discourage visceral adhesions, a cause for postoperative chronic pain, erosion and a morphological indicator of surgical failure. This may involve bowel, nerve and/or omentum adhesion to the interabdominal face of the prosthetic (25, 26).
A new generation of hernia prosthetics, the composite meshes, improve on traditional synthetics by including a film that discourages visceral adhesion without compromising tissue integration. These materials present a temporary/resorbable barrier that modifies the tissue interaction with the underlying base polymer (27).
Previous research has shown that systemic concentration of certain cytokines varies in response to delivery of a synthetic surgical mesh (28), although systemic monitoring of biomaterial compliance is very much an emerging field. To this end, we designed this early-stage study to determine whether the systemic cytokine concentration of any inflammatory biomarkers from a broad panel could dynamically report on the ongoing tissue response in vivo. Two composite meshes comprising a biologic film layer over a macroporous textile and a noncomposite polyester control were implanted in a rat, full thickness, abdominal wall excision model. Levels of systemic inflammatory cytokines were measured using an inflammatory cytokine array to predict their efficacy and biocompatibility, which was validated using macroscopic characterisation and histopathology. The objective of our research was to suggest possible biomarkers that could be used clinically to monitor real-time the interaction of a biomaterial with the tissues around it and ultimately confirm the remission of inflammation, using herniorrhaphy as a benchmark procedure.
Materials and Methods
Materials
Material A was a non-composite flat sheet polyester mesh control; material B was a large-pore polypropylene mesh with 2 oligocaprone films and a polydioxanone gluing layer; and material C was a polypropylene mesh, with sodium hyaluronate/carboxy-methylcellulose film. These materials were selected based on our expectation that the noncomposite material would be adhesion promoting as opposed to the other materials, which would retard or inhibit adhesions. This allowed us to base our analysis on a surgical material that performs poorly versus successful implants in the same anatomical location.
Sample Preparation
Materials were aseptically cut into 3 × 2-cm rectangles in a sterile field (class II cabinet) and maintained in a sterile environment until implanted.
Interperitoneal Implantation
Subjects (Wistar rat, male, 6 weeks old, 250–270 g) were anaesthetised using an equal ratio of O2/N2O supplemented with isoflurane at 2% (v/v). Once the subject was sedate (confirmed by absence of pedal withdraw reflex), the incisional area was shaved and sterilised using Videne. Pain relief (buprenorphine) and prophylactic antibiotic (Baytril™) were administered by subcutaneous injection.
A 3-cm cutaneous depth abdominal incision was made to reveal the abdominal wall, which was elevated to confirm absence of visceral attachment. Using dissection scissors, a cut of 3 cm in length was made across the elevated linea alba such that 3 × 2 cm of musculature was excised. Material was then inserted into the defect, underlying the peritoneum and fixed in place using approximately 6 to 10 interrupted PGA sutures. Where materials were decorated with anti-adhesive coatings, the prosthesis was orientated such that the antiadhesive face was in contact with viscera. After securing the implant, skin was closed over the material using wound clips. Animals were maintained in single cages and checked daily for signs of complications such as seroma, haematoma and wound dehiscence.
Animals were euthanized using an incremental concentration of CO2. Death was confirmed by destruction of the vertebral column before dissection to remove implants.
Explants were performed after 1 (n = 4/material), 4 (n = 10/material) and 12 (n = 4/material) weeks.
All procedures were performed in compliance with the UK home office guidelines on the use of animals in scientific procedures.
Histopathology
Fixation and antigen presentation was performed as previously described (29). Briefly, samples were placed into periodatelysine-paraformaldehyde fixative on a roller for 7 days at 4°C, during which fixative was refreshed 3 times. Fixative was removed and replaced with cold washing solution at 4°C for 24 hours. Cold washing solution was replaced by ice-cold acetone for 48 hours at 4°C. Once samples were dehydrated they were immersed in Technovit infiltration solution for 24 hours at 4°C. Specimens were cast in place in appropriately sized moulds, orientated for optimum cutting and submersed in Technovit embedding solution (TAAB Laboratories Equipment). The preresin surface was covered with mineral oil to prevent oxidation and evaporation, sealed with aluminium foil and placed at −55°C to infiltrate for 7 days followed by −20°C for 2 days to complete polymerisation. Tissue blocks were sectioned (5 μm) using a polycut microtome (Reichert-Jung) and placed onto slides coated with 3-aminopropyl triethoxysilane. Unless stated otherwise, all reagents were purchased from Sigma-Aldrich.
Haematoxylin and Eosin Staining
Samples on APTES coated slides were heat fixed and submersed in Harris's haematoxylin for 5 minutes followed by 5 minutes of development under running tap water. Specimens were the differentiated using 1% acid alcohol (1% HCL/EtOH) for 5 seconds and washed under running water for 1 minute. Samples were then bathed in 1% eosin for 3 minutes and finally washed under running tap water for 1 minute before dehydration using a gradient of ethanol, clearance with xylene and mounting with DPX.
Multiplex Inflammatory Cytokine Array
To systemically quantify inflammatory cytokines in response to the materials, blood was collected by cardiac puncture immediately after euthanasia. Blood was allowed to clot, serum was aspirated from the clot and centrifuged (1,000 G, 4°C, 10 minutes) to remove residual erythrocytes and stored at −55°C.
Inflammatory cytokine arrays were performed using the Milliplex Map method; unless stated otherwise, all array equipment and reagents were purchased in kit form from Merck Millipore. Assays were performed following the manufacturers' supplied instructions and analysed using a Luminex200 cytometer. Analytes measured throughout these studies were: Eotaxin, GMCSF (granulocyte macrophage colony-stimulating factor), GCSF (granulocyte colony stimulating-factor), IL-1α, MCP-1 (monocyte chemotactic protein-1), Leptin, MlP-1α (macrophage inflammatory protein-la), IL-4, IL-1β, IL-2, IL-6, IL-13, IL-10, IL-12, IL-5, IFNγ, IL-17, IL-18, IP-10, GRO/KC (growth regulated oncogene/keratinocyte chemoattractant), RANTES (Regulated on activation normal T cell expressed and secreted), TNFα and VEGF.
The multiplex technology utilises a microbead with a defined spectral signature to which is attached a monoclonal antibody to a single epitope of a protein. This bead/antibody conjugate is incubated with serum obtained from cardiac puncture of the experimental animals that allows the beads to harvest proteins. After this, a FITC-conjugated secondary antibody is added with an affinity to an alternative epitope of the protein of interest. Beads were then analysed using the Luminex200, which reads the spectral signature of the bead (analyte species) and the associated FITC intensity (analyte concentration). Multiplexing was performed by using beads with several spectroscopic signatures, each of which is conjugated to a capture antibody for alternative molecules. The detection hardware was configured to record a minimum of 50 bead events from each user defined spectral signature, allowing a mean analyte concentration to be calculated.
Blood was also collected from animals that had not received any additional surgery, that were of identical age as the experimental subjects and that received the same maintenance regime. This allowed a normal basal cytokine profile to be deduced for each molecule at each experimental endpoint.
Statistics
Statistics on inflammatory cytokines were performed using ANOVA analysis to compare cytokine concentrations at individual time points using the software platform SPSS version 8.0; significance levels were set at *0.05, **0.01 and ***0.005. Error bars on all graphs represent 1 standard deviation from the mean.
Pathological Evaluation
Adhesion severity was classified macroscopically using the Zuhlke criteri, (0: no adhesions - 4: dense adhesions, only dissectible with sharp instruments with organ damage almost unavoidable) (30, 31). Samples were also microscopically evaluated considering biological features and cell populations associated with wound healing, infection and foreign body response. Samples were not blinded to the scorer.
Results
One-Week Explants
Macroscopic
After 1 week in vivo, material A demonstrated large amounts of interabdominal adhesions. Adhesions were predominantly adipose, covering 70% to 100% of the material surface, and were not easily retractable with dissection apparatus.
Material B also demonstrated visceral adhesions, but to a lesser extent than material A. Similarly, adhesions were predominantly adipose. In 1 instance it was not possible to conclude that there were any adhesions in the case of material B, however, in the remaining 3 implants adhesions consumed 40% to 60% of the material interabdominal face.
In 1 instance, Material C was completely engulfed by adhesion tissue, which included adipose, omentum and liver. In the remaining 3 implants only small amounts of connective adipose tissue had adhered, covering between 5% and 20% of the implant visceral surface (Fig. 1).
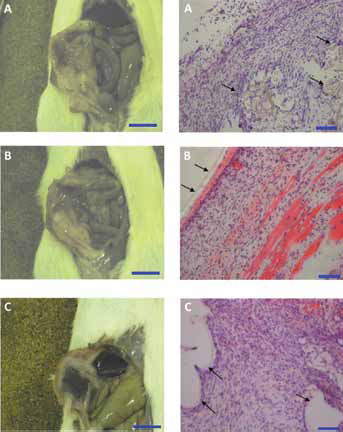
Macroscopic and histopathological observation of tissue interaction with (
Microscopic
Material A showed disordered, random host cell infiltration in and around the material, comprising macrophages, neutrophils and fibroblasts. There was very little fibroplasia and matrix deposition in the prostheses after 1 week.
Material B demonstrated organised association with abdominal wall musculature. It was possible to observe healthy intact peritoneum connected to the mesh by a small ribbon of fibrous connective tissue, which persisted into the abdominal musculature.
Material C was densely populated by host cells comprising fibroblasts, neutrophils and macrophages filling the interfibre spaces. The material was enshrouded with a small amount of fibrous tissue and remained well integrated with existing muscle (Fig. 1).
Four-Week Explants
Material A demonstrated consistent, weak adhesions to underlying viscera. Adhesions were almost exclusively adipose, with the exception of 2 instances in which adhesions persisted between implant and liver. Adhesions were not mechanically strong and they easily dissected from the material. Histologically, material A demonstrated substantial cellular infiltrate of fibroblasts and macrophages with mesh fibres partially encapsulated by foreign body giant cells. Material A integrated well with existing stroma, particularly adipose stroma, which in a number of instances was closely associated with infiltrating cell populations. Material A was not excessively encapsulated nor did it stimulate significant fibrosis (Fig. 2).
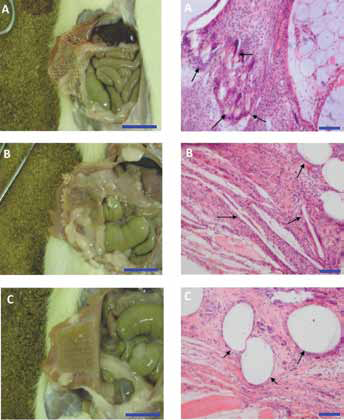
Macroscopic and histopathological observation of tissue interaction with (
Material B supported adhesions of peritoneal adipose and connective tissue in almost all grafts and stimulated a large cell response of predominantly myeloid and fibroblast populations. The large interfibre spaces of material B were completely filled with neomatrix (Fig. 2).
In material C significant adhesions were rare; the participating tissue was adipose in the small amount of adhesions recorded, with 1 exception demonstrating hepatic adhesion. These observations were reflected histologically. Material was well colonised and remained unencapsulated without excessive polymorphonuclear cell recruitment. Material C was well integrated with host musculature (Fig. 2).
Twelve-Week Explants
Macroscopic
After 3 months in vivo, the small amount of visceral adhesions observed after 28 days in material A had expanded to include large amounts of interabdominal adipose that in 3 instances completely engulfed the prosthesis. Adhesions were permanent and difficult to separate from the material. In 2 instances, material A also elicited bowel adhesion, although there was no trace of seroma or haemorrhage at the implant. Despite adhesions, animals did not show any external symptoms associated with abdominal pain, and defects remained closed and load bearing.
Three months postimplant, material B was largely free of interabdominal adhesions. In 2 instances, small amounts of easily resectable adipose had attached to the patch surface; however, no particularly chronic adhesions were observable with material B.
Material C remained adhered to small amounts of interabdominal adipose with the main expanse of the material surface adhesion free; adhesions to bowel or liver were not recorded. Material C remained intact and repaired the defect without any adverse macroscopic reaction after 3 months (Fig. 3).
Microscopic
After 3 months, material A was densely colonised by host cells, including foreign body giant cells throughout the material and interfibre spaces. Material A was encapsulated, although not excessively, with neofibrous tissue with no histopathological indicators of oedema or mesh degeneration.
Material B also infiltrated with matrix secreting cells that filled interfibre voids. Cells surrounding material B secreted fibrous matrix that maintained excellent integration with surrounding tissues. After 12 weeks it was difficult to discern the film coating of the materials histopathologically; however, the underlying polymer was not subject to any noticeable degeneration or resorbtion.
Material C colonised with cells more sparsely than the other materials, however, it did integrate particularly well with surrounding tissue. This is exemplified specifically in Figure 3 by the interaction of the material with native musculature. Similarly to material B, no antiadhesive film was observable after 12 weeks in vivo, however, the underlying polymer remained intact (Fig. 3).
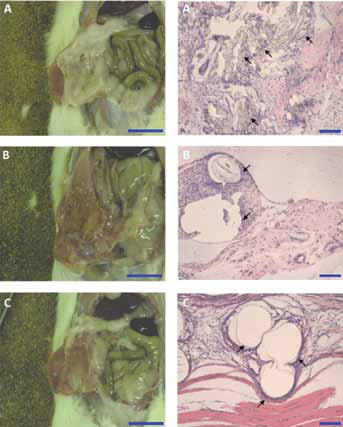
Macroscopic and histopathological observation of tissue interaction with (
Systemic Inflammatory Cytokine Analysis
Inflammatory cytokine analysis was used to elucidate if histopathological or macroscopic indicators of surgical success could be associated with changes in the systemic concentration of a panel of soluble cytokines.
From the large panel of biomarkers analysed, significant intermaterial differences were concluded from a subgroup shown in Figure 4. However, a number of cytokines were only stochastically detectable or fell close to the lower detection limits of the apparatus and as such were discounted from the analysis. These included IL-4, IL-2, IL-13, IL-12 and IP10. In the instance of monocyte chemotactic protein 1 (MCP1), after 1 week all of the materials stimulated an increase in this molecule systemically versus a nonoperated control. Material A stimulated a greater production of MCP compared to materials B and C. After 4 weeks, the response had largely normalised, although small intermaterial differences were apparent. Similarly, after 12 weeks a small but significant difference was recorded in material A versus the nonoperated control.
Interestingly, after 4 weeks leptin production had decreased in the material set versus the nonoperated control, which was found to be statistically significant in the cases of materials A and B. However, throughout the 12-week time course the amount of systemic leptin increased in all subjects, including the control animals (Fig. 4).
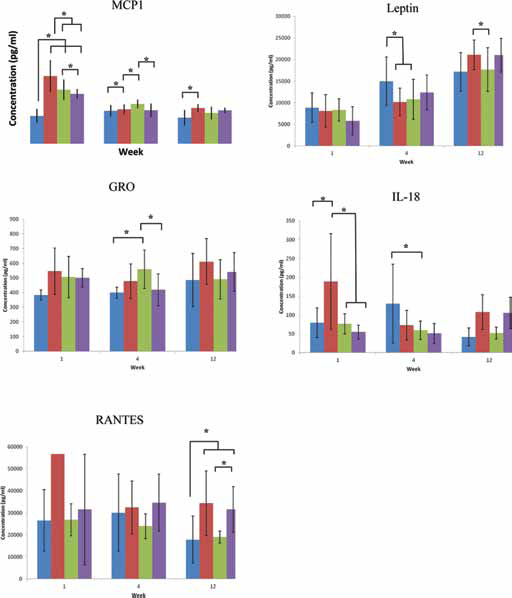
Systemic inflammatory cytokine analysis of serum from experimental animals. Control = non-operated animals maintained identically to operated subjects. n = a minimum of 3 inter animal repeats weeks 1 and 12 and 8 inter animal repeats week 4 (MCP1, Leptin, GROKC, IL-18), a minimum of 3 inter animal repeats for all time points in the control group and a minimum of 2 inter animal repeats weeks 1 and 12 and 7 inter animal repeats week 4 (RANTES) p<0.05. Blue = Control, red = Material A, green = Material B, purple = Material C.
Also worthy of note is the finding that proinflammatory IL-18 production was significantly increased in material A versus the control groups, and materials B and C, which were found to stimulate significantly less IL-18 than material A. This may suggest that this molecule is an appropriate early systemic marker of focal inflammation. After 4 weeks, all of the implant groups stimulated a reduction in IL-18 production versus the nonoperated animals, which may suggest that the tissue had progressed from a destructive to a constructive inflammatory phase (Fig. 4).
An additional proinflammatory cytokine GROKC (CXCL1) was found to be increased in all of the operated animals versus the nonoperated control group after 1 week; it also increased in materials A compared to material C and the control group after 4 weeks. Although the response had largely normalised between the implant and control groups after 12 weeks, RANTES, the pro-inflammatory T-lymphokine, demonstrated large interexperimental variation after 1 week, making it impossible to use to detect significant differences. This cytokine was also significantly increased in materials A and C after 12 weeks (Fig. 4).
Discussion
The use of prosthetic materials to support abdominal wall closure significantly decreases hernia recurrence; they are an essential and clinically successful biomaterial intervention. However, there are still postoperative complications, particularly manifesting as neuropathic chronic pain. The aetiology of this is mostly rooted in host versus material inflammation, and is present as deviations from stable wound healing and material integration. In extreme circumstances this may manifest as intra-abdominal adhesions to the visceral face of the material, incorporating nerves or tissue nociceptors.
Therefore, it is important to engineer materials with thorough prediction of their interaction with a patient's defence mechanisms and inflammatory cascade. The future of this area of biomedicine will undoubtedly rely on targeted, real-time monitoring of material integration using systemic biomarkers. This presents a breakthrough in assessing material performance, by predicting failures before they occur, providing clinicians with the opportunity to reintervene before the onset of chronic pain or healthy tissue destruction by an aggravated leukocyte response. Our study was designed as a preliminary piece of work in this emerging, essential area of biomaterials research. It is intended as a frontline [diagnostic?], using a multiplex approach to identify any potential target cytokines based on levels that have fluctuated as a consequence of material reception, and to potentially extrapolate these findings to poor macroscopic and pathological performances should they have arisen during the research study.
To this end, a group of materials were evaluated in a rat, full-thickness abdominal wall device model to investigate systemic inflammatory cytokine quantification as a tool for minimally invasive dynamic monitoring of material integration. Systemic findings were validated post explant by assessing quantity and strength of visceral adhesions, and histologically to deduce the extent of cellular infiltration and inflammatory cell recruitment.
This study demonstrated that it may be possible to use systemic cytokines at 2 levels whilst monitoring biomaterial integration. A subset of cytokines were hyperproduced, regardless of the material composition, and it was possible to characterise increases in particular cytokines during tissue/material integration in conjunction with the most adhesion-promoting of the materials, namely, material A. Future studies in this area by our group will include a more substantive “poor performer” to enable a definitive conclusion regarding a group of molecules that are elevated or specifically secreted throughout a tissue during a failed attempt at material integration and acceptance.
Our studies suggest that IL-18 was increased in response to the most adhesion-promoting material after 1 week, although this response was present over more chronic time points – times during which we predict that the tissue healing process will have entered the remodelling phase rather than the attacking phase if the material still persists. This cytokine was therefore suggested from the panel of molecules considered in this study as a potential sentinel of material failure. Indeed, we intend to further study the role of this cytokine in biomaterial compliance based on these findings, although our larger aim is for our present work to allow noninvasitve analysis of cytokine profiles in the blood to form part of a prognostic workflow that allows device retrieval/replacement before the onset of chronic pain.
Given the proinflammatory IL-1-like function of this TH1 cytokine, there are reasonable grounds to suggest IL-18 as a possible clinical candidate for monitoring biomaterial failure during the acute inflammatory period (32). This molecule has been previously implicated in the aetiology of failed organ allotransplants and has been shown to fluctuate in systemic concentrations as a function of disease severity (33, 34). Indeed, one study has suggested that IL-18 can be used to predict systemic or distant tissue effects of surgical procedures, such as acute kidney injury as a consequence of liver transplantation, which has been predicted by a rise in plasma IL-18 as early as 1 hour post-surgery (35).
After 1 week, all materials stimulated an increase in systemic MCP1 above a nonoperated control; the greatest increase was in material A. Interestingly, in the instance of IL-18 only material A stimulated secretion above the nonoperated control after 1 week.
RANTES has not so far been clearly correlated as a systemic biomarker of wound healing failures or complications. It is, however, interesting to note that RANTES, secreted by lymphocytes and vascular endothelial cells, has been shown to play a critical role in macrophage recruitment into inflammatory active sites. This may locally influence the angiogenic process and tissue remodelling at the injury site (8).
Histologically, all of the materials infiltrated with host cells. This typically included fibroblastic and myeloid lineages comprising macrophages and foreign body giant cells. Histopathology was graded on a standard visual index scale of 0 to 4, on which statistics could be performed using chi-squared analysis. Across the inflammatory and wound healing indices, the only statistically significant difference was the prevalence of foreign body giant cells.
Conclusions
In this preliminary study into systemic monitoring of biomaterial compliance, inflammatory cytokine analysis was considered in an animal model alongside histopathology to predict biomaterial tissue interaction. All of the materials tested repaired the defect without major adverse reactions or herniation, which therefore suggests that substantial deviations from basal cytokine levels would be unusual given the pathological lack of adverse inflammation. Histologically, the materials all integrated well with the surrounding abdominal musculature and infiltrated completely with cells, which supported the inflammatory cytokine data by the absence of histopathologic indicators of an adverse material interaction.
Future studies in this area will consider these candidate molecules in further detail alongside more macroscopically poorer forming materials in order to truly elucidate and develop an understanding of the roles of these signalling molecules in the biomaterial interrogation process.
Footnotes
Conflict of interest: HA, SW, YB are Covidien employees. The other authors have no financial interest related to this study.