
Abstract
Background
The aim was to investigate factors associated with the successful achievement of ≥21 l/session of substitution fluid volume in patients on post-dilution hemodiafiltration.
Methods
3315 patients treated in 6 European countries with the Fresenius 5008 CorDiax machine including the AutoSub Plus feature were considered. Variables that showed a relationship with convection volume were entered in a multivariable logistic regression model.
Results
Mean blood flow was 379 ± 68 ml/min. Median substitution volume was 24.7 L (IQR 22.0–27.4 L). Mean filtration fraction was 28.3 ± 4.1%. 81.5% of sessions qualified as high-volume HDF (substitution volumes ≥21 L). Higher age, dialyzer surface area, blood flow and treatment time were positively associated with the achievement of ≥21 L substitution volume; higher body mass index, male gender, higher hematocrit, graft or catheter vs. fistula, and start of week vs. mid-week were negatively associated.
Conclusions
Dialysis center policy in terms of blood flow, treatment time, filter size, and perhaps even hemoglobin targets plays a key role in achieving high-volume HDF. All of these are modifiable factors that can help in prescribing an optimal combination of dialyzer size, achievable blood flows, and treatment times.
Introduction
Nobody can deny that current renal replacement therapy, although capable of sustaining life for many patients worldwide, is far from optimal. Among the different factors that can enhance the efficacy of extracorporeal blood purification, Vanholder et al (1) highlighted the value of convective removal of toxins, with β2-microglobulin clearance being the most logical efficacy quantifier (2). Today, medical device producers offer a large portfolio of dialyzers with high β2-microglobulin sieving coefficients. Here, the plasma reduction rate for β2-microglobulin is proportional to the substitution fluid volume exchanged during the treatment (3). For this reason, the actual volume of substitution fluid became the only limiting factor for enhancing blood purification in hemodiafiltration. Regarding hard outcomes, studies published after 2005 demonstrated that the threshold of substitution fluid volume that should be administered in postdilution hemodiafiltration in order to reduce patient mortality is in the range of 20 to 22 liters per session (4–6). Theoretically, substitution volume should be weighted by an anthropometric parameter reflecting the patient's metabolic needs (e.g., body size or body surface area). Several anthropometric parameters have been proposed (7) but Maduell et al was unable to find a better fit than the simple substitution fluid volume or total convection volume (5). Therefore, in terms of both efficacy and outcomes, focus has now shifted to the question of feasibility of attaining this level of substitution fluid dose for a large majority of patients on extracorporeal dialysis treatment.
In the CONTRAST study, failure to demonstrate a positive trend in reducing mortality in patients treated by hemodiafiltration compared to low-flux dialysis was attributed to several factors. However, one of the most important was considered to be the substantially lower average in convection volume (i.e., substitution fluid volume plus ultrafiltration volume) achieved compared to the planned target (20.7 L compared to the targeted 24 l/session) (4). Nevertheless, in the same study, patients treated with more than 21.95 l/session of convection volume showed a significantly decreased mortality rate. The targeted substitution fluid volumes were successfully reached in the other 2 important randomized clinical trials addressing the relationship between hemodiafiltration and outcomes (5, 8). The substitution fluid volume targeted in the Turkish study was quite low (>15 l/session) and, in a post hoc analysis, the subgroup of HDF patients treated with a median substitution volume >17.4 L per session had better cardiovascular and overall survival compared with the high-flux HD group (8). The higher substitution fluid volumes achieved in the study of Maduell et al (>18 l/session targeted, median quarterly volume achieved ranged from 20.8 to 21.8 l/session thanks to training to achieve high values) also resulted in a positive outcome in terms of survival (5). In this latter study the result was obtained with an average blood flow rate of 387 ml/min. In order to reach 21 L of substitution volume in a standard 4-h session with a blood flow of 400 ml/min, a filtration fraction of 24.4% suffices. Lower blood flows translate into a higher demand on the filtration fraction, which could increase the risk for clotting when using conventional machine technology.
Several factors can affect success in reaching planned targets of substitution fluid volume (7). The first are patient characteristics, such as vascular access type, vascular access flow, total protein level, and hematocrit. The second are factors associated with the dialysis prescription and best nursing care practices, such as the dialyzer type, the selected arterial and venous needles, level of blood flow rate (within the limit allowed by the vascular access), and the duration of the dialysis session. The management of the treatment is important as well, since the integrity of the dialyzer is also ensured by a correct anticoagulation regimen. The achievement of the prescribed blood flow is also related to correct cannulation practices (9). The third type of factors are machine features controlling aspects of the treatment. With HDF machines that work on the basis of volume control with a constant UF rate, there is the risk of an increased transmembrane pressure with associated alarms. With HDF machines that work with a UF rate that is adjusted according to the behavior of the transmembrane pressure, there is a risk that the targeted substitution volume will fail to be achieved. Clearly, some of the above-mentioned factors, such as the treatment prescription, are modifiable, while others, such as vascular access patency, are not.
The aim of this study was to investigate the relevance of modifiable and non-modifiable factors associated with the successful achievement of 21 l/session of substitution fluid volume in patients on post-dilution online HDF, all treated with an innovative HDF device that continuously adapts the substitution fluid flow according to blood viscosity and dialyzer performance.
Methods
The patients who were included in the study were younger than 85 years and were treated 3 times a week by post-dilution HDF between June 1 and August 31, 2013 in one of 46 NephroCare clinics located in the Czech Republic, Hungary, Italy, Portugal, Slovenia, and Spain. Postdilution HDF was performed with the 5008 CorDiax dialysis machine (Fresenius Medical Care, Bad Homburg, Germany), which incorporates the AutoSub Plus feature. This relatively new element is an advance on standard online HDF equipment available on the market and manages ultrafiltration by automatically controlling the continuous optimization of the substitution fluid volume rates without any user interaction. The basic principle of AutoSub Plus is to avoid excessive hemoconcentration in the dialyzer by continuously adapting the substitution flow according to changes in blood viscosity in the dialyzer and the performance of the dialyzer. These changes are identified using signal analysis of the pressure pulses transmitted from the peristaltic blood pump. Signal analysis is conducted several times per minute and the substitution rate is automatically adapted based on pressure pulse attenuation and cross-membrane pressure assessment. The result of this loop-back control application is an automatic individualization and maximization of the substitution volume with respect to blood flow, whole blood viscosity, and dialyzer characteristics. The AutoSub Plus option is a specific improvement included in the CorDiax software from the version 4.50 on. At the time of this evaluation, the software version 4.50 was implemented in 46 NephroCare clinics located in the 6 countries listed above. All patients treated with this option and satisfying the inclusion criteria were considered for the study.
The adequate dialysis dose was controlled for each session by Kt/V measurements made with the integrated online clearance tool (OCM; Fresenius Medical Care, Bad Homburg, Germany), based on ionic dialysance (10). High-flux FX CorDiax dialyzers with different surface areas were used almost exclusively for the HDF treatments. The achieved dialysate flow was the prescribed dialysate flow minus the achieved substitution fluid flow. Treatment times were fixed at a minimum of 240 min, and effectively achieved on a schedule of three times a week. Sterile and non-pyrogenic substitution fluids were produced by ultrafiltration of the ultrapure dialysate. Ultrapure quality was defined as bacterial counts <0.1 CFU/ml and endotoxin levels <0.03 EU/ml.
All data considered in the study were automatically collected through the EuCliD database, which has been described in previous publications (11, 12). As prescribing physicians and nurses were not aware of any study intention, the data collected represent the clinical reality as opposed to data collected in a controlled clinical trial. Treatment-related variables, such as effective treatment time, total treated blood volume, substitution volume, and pre- and post-dialysis body weight, were mostly gained directly from the dialysis machine and the associated scale by the TDMS system (Therapy Data Management System; Fresenius Medical Care, Bad Homburg, Germany). The convection volume was calculated as the sum of the substitution volume per treatment and the net ultrafiltration volume defined according to the patient's weight loss. Mean convection flow rate was defined as the convection volume divided by the effective treatment time; for practical clinical purposes, in accordance with the EUDIAL group, mean filtration fraction was defined as the mean convection flow rate divided by the mean blood flow rate. High-volume HDF was defined as a total substitution volume ≥21 L per treatment (7).
Data were reported as proportions, as means with standard deviation (SD), or as median with interquartile range (IQR, 25th–75th percentiles) for non-normal distributions. A pooled logistic regression model was used to account for the correlated data arising from repeated measurements in studying the independent relationship of each variable with substitution volume, whereby 21 L substitution volume was considered the outcome threshold. Patient- and dialysis-related variables that showed an association with the convection volume were entered in a multivariable model. In addition, hematocrit was entered into this multivariable model up front in accordance with the results of 2 previous studies (13, 14). Results were considered statistically significant for P<.05. SAS statistical software (SAS Institute, Cary, NC, USA) was used for all pooled logistic analyses, while SPSS (SPSS Statistics for Windows, Version 21.0, IBM Corp., Armonk, NY, USA) was used in all other cases.
Results
The study considered 3315 patients who were treated for a total of 106 827 sessions of post-dilution HDF using one or more of 6 differently sized dialyzers. Mean follow-up time was 10.7 weeks. The mean age of the patients was 64.5 ± 13.7 years, 60.8% of whom were male, and 27.3% diabetics. The median dialysis vintage was 61.2 months (IQR 24.6–117.2). Hematocrit was 34.9 ± 4.6% and serum albumin 3.81 ± 0.47 g/dl. The FX CorDiax 600 dialyzer was used for 73.2% of the sessions, the FX CorDiax 60 for 9.4%, the FX CorDiax 100 for 4.6%, with other filters of different surfaces of the FX CorDiax and of the FX classic family used for the remaining sessions. Accordingly, most of the patients were treated with dialyzers with a surface of 1.60 m2 (73.8%), 14.4% with dialyzers with a surface of 1.80 m2 to 2.20 m2, and 11.8% with dialyzers that had a surface area below 1.60 m2. The mean effective treatment time was 253 ± 19 min/session. The median substitution volume was 24.7 L per treatment (IQR 22.0–27.4 L) and the mean filtration fraction was 28.3 ± 4.1% (IQR 25.9–30.8%). The percentage of the sessions that qualified as high-volume HDF was 81.5% (substitution volume was ≥21 L); for fistula, graft, and catheter sessions, the percentages were 86.2%, 83.2%, and 55%, respectively.
Table I describes patient characteristics, treatment features, and the results of the hemodiafiltration sessions by the most commonly used dialyzers. The highest percentage of high-volume HDF sessions was achieved with the FX CorDiax 100 filter with a surface area of 2.20 m2 (92.8%). Success rates decreased with decreasing filter surface area but were still very high at 70.2% with the smallest dialyzer tested (FX CorDiax 60 with 1.40 m2 surface area).
Comparison of treatment characteristics with the 4 most frequently applied dialyzers
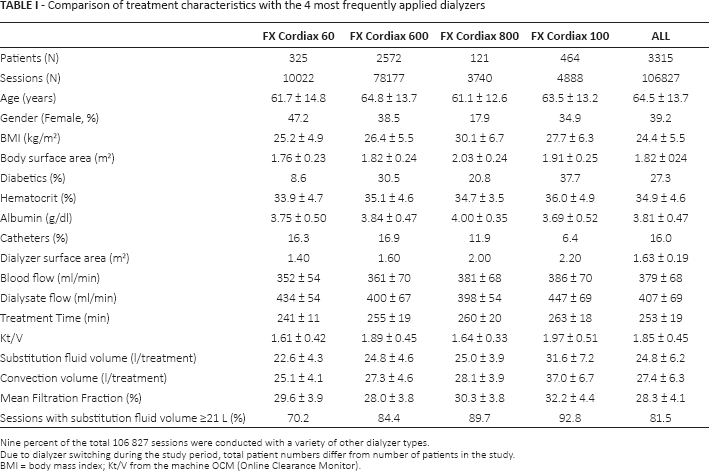
Nine percent of the total 106 827 sessions were conducted with a variety of other dialyzer types.
Due to dialyzer switching during the study period, total patient numbers differ from number of patients in the study
BMI = body mass index; Kt/V from the machine OCM (Online Clearance Monitor).
The mean blood flow rate was 379 ± 68 ml/min. The median blood flow rate by dialyzer surface area varied between 350 ml/min and 400 ml/min (Fig. 1). Of all the patients, 79.5% had a fistula, 4.5% a graft, and 16.0% a catheter. The mean blood flows achieved with the fistulas, grafts, and catheters were 392 ± 64 ml/min, 390 ± 62 ml/min, and 316 ± 602 ml/min, respectively, Figure 2 depicts the proportion of fistulas, grafts, and catheters by dialyzer surface area.
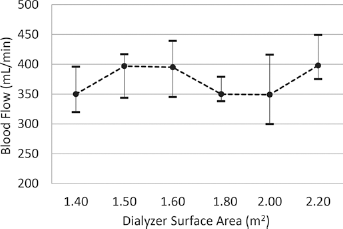
Median blood flow rate by dialyzer surface area (median, 25th and 75th percentile).
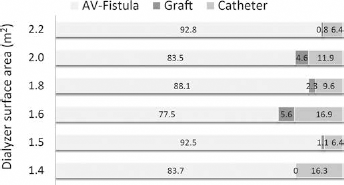
Proportion of AV-fistula, graft and catheters by dialyzer surface area.
The multivariable logistic regression model to predict the achievement of at least 21 L of substitution fluid evaluated the following variables: age, dialyzer surface area, blood flow, treatment time, body mass index (BMI), gender, hematocrit, vascular access type, albumin, and weekday of treatment. Results are presented in Table II.
Multivariate logistic regression analysis with achievement of ≥21 I of substitution fluid as outcome
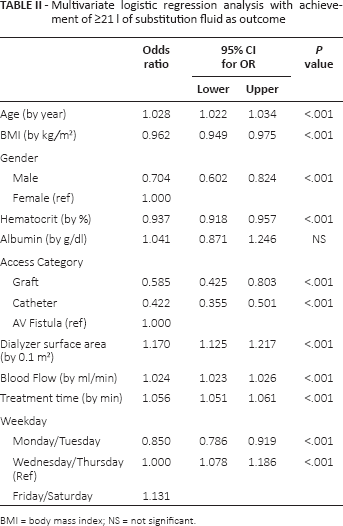
BMI = body mass index; NS = not significant.
Dialyzer surface area was positively associated with the achievement of the target substitution volume (per 0.1 m2 of dialyzer surface: OR: 1.170, 95% CI: 1.125–1.217; P<.001). Also, as expected, higher blood flow was a significant positive factor (per ml/min of blood flow: OR: 1.024, 95% CI 1.023–1.026; P<.001) as well as the treatment time (per min of effective treatment time: OR: 1.056, 95% CI 1.051–1.061; P<0.001). Dialysis treatments conducted at the end of the week were more likely to achieve the substitution volume target compared to mid-week sessions (OR: 1.131, 95% CI 1.078–1.186; P<0.001). Analysis of the weight loss requirements per session weekday revealed that this is likely to be due to the proportionally higher weight loss requirements at the beginning of the week, i.e., 2.78 L and 2.68 L on the first session of the week versus 2.38 L and 2.32 L mid-week, and 2.35 and 2.33 L at the end of the week (Fig. 3).
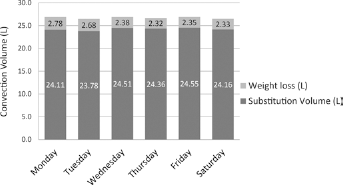
Substitution fluid volume and weight loss contributions to total convection volume.
Higher BMI and hematocrit were negatively associated with the outcome, as was male gender. Having a catheter as vascular access was associated with a 58% significantly lower odds ratio (OR) for achieving the target infusion volume compared to sessions conducted with a fistula (OR: 0.422, 95% CI 0.355–0.501; P<.001). Also having a graft was associated with a significant 41.5% lower OR compared to a fistula (OR: 0.585, 95% CI 0.425–0.803). The serum albumin level was not significantly related to the achievement of the target substitution volume.
Discussion
In this study, the target of at least 21 L of substitution fluid was reached in 81.5% of post-dilution hemodiafiltration sessions. This high number is a reflection of general acceptance of the positive results reported in the literature regarding survival data, but it is also the result of the dialysis network strategy to target high efficiency renal replacement therapy with measures such as high Kt/V and high substitution volumes. Last but not least, the implementation of the AutoSub Plus for the continuous modeling of the substitution fluid flow according to blood viscosity and dialyzer performance certainly contributed to the high success rate.
This study confirmed the influence of some patient-related factors already reported by previous papers, namely BMI and hematocrit (13, 15). Regarding gender, while we found an advantage for female gender, Penne et al reported a positive association of male gender with convection volume in a univariate analysis, which was not confirmed in their multivariable model (13). We did not find a significant association with gender in a previous study of our network (14). This discrepancy in findings can of course result from the extensive adjustments introduced into the current study, in which, in absolute terms, males were found to be more likely to achieve the target substitution volume (82.9% vs. 79.3% in females).
Regarding albumin, it was generally believed that the high ultrafiltration rates in postdilution HDF can result in protein cake formation. These effects can raise transmembrane pressure, causing alarms, reducing clearances and possibly resulting in clotting of the extracorporeal circuit (7). However, in 2 previous studies higher serum albumin was positively associated with the achieved volume of substitution fluid (13, 14). In this study, albumin was not significantly associated with the OR to achieve the target substitution volume. Taken as a whole, since 3 different studies have now been unable to demonstrate the expected negative association between albumin and high substitution volume achievement, it is likely that the positive effect of refilling associated with higher albumin level compensates for the expected negative impact on the membrane functionality (16).
The results pertaining to treatment-related factors are naturally of particular interest due to the potential they offer for adjustment. Penne et al reported that high blood flow and treatment time were critical factors associated with the achievement of the target convection volume (13). These factors have also been confirmed in our current and previous analyses (14). In addition, differently to Penne et al, we found not only the confirmation of our previous observation that catheters are associated with a significantly lower OR to achieve the target substitution volume, but also the novel observation of the importance of the dialyzer surface area. These findings were facilitated by the large number of patients and treatments analyzed, and also by the moderate degree of variability in terms of dialyzer surface areas present in the database (13). Nevertheless, the results reported in Table I are somewhat difficult to interpret. While increases in (a) substitution volume, (b) the proportion of sessions that qualify as high-volume HDF, and (c) dialyzer surface area run in parallel, it is noteworthy that patients treated with small-surface area dialyzers (i.e., 1.40–1.60 m2) tend to have a high percentage of catheters (Fig. 2). In addition, Table I also shows that the important factor treatment time also increases in parallel with the surface area of the filters; the increase is around 20 min moving from the smallest to the biggest dialyzers. Contrary to our expectations, mean blood flows did not increase remarkably with increasing the dialyzer surface area, ranging only from around 350 ml/min to 390 ml/min, in agreement with what is recommended by Maduell et al (5). In general, it seems that patient size is one of the main criteria for the prescription of dialyzers with higher surface areas.
Multivariable analysis revealed the importance of the potentially modifiable treatment factors of vascular access (if options are still open), treatment time, blood flow, but also dialyzer surface area, once adjusted for patient-related variables. An increase of 0.1 m2 of dialyzer surface was associated with a 17% increase of the OR to achieve the target substitution volume.
The question remains regarding how to address the residual 18.5% of sessions where the high-volume target was not reached. First, since the percentage of patients on catheter reaching the target is relatively low at 55%, we need to identify patients who are more likely to be treated with a catheter. The best solution is of course to plan for an arteriovenous fistula or a graft according to the vascular situation, but this is not always possible. Many patients remain with a catheter for life – specifically older patients with some associated comorbidities (17). So should dialysis via a catheter automatically mean acceptance of the risk for inferior treatment? If the answer is no, then we need to search for ways to correct the intrinsic limitation of this type of vascular access with what we can modify in the treatment prescription. This study suggests that not only can the obvious treatment time play a role, but also the dialyzer surface area. Longer treatment time, in the range of an additional 15 to 30 min, can also decrease the ultrafiltration rate required to achieve the same ultrafiltration volume. This can possibly improve treatment tolerance and consequently dialysis dose, as was highlighted by Maduell et al (18) while evaluating nocturnal every-other-day HDF; and by Cornelis et al (19) who reported enhanced removal of solutes by extended HDF. Treatment tolerance is often the most critical point in treating elderly dialysis patients (20, 21). Unfortunately, our data indicate that the option to increase treatment time is often not considered today, since the average effective treatment time of patients with fistula and those with catheter hardly differ (253 ± 18 and 252 ± 21 min, respectively). The prescription of a dialyzer with a higher surface area can be the next step, but in order to ensure that the maximum benefit of the bigger and more expensive dialyzer is received, it should be postponed to after a search has been completed for the highest possible blood flow and after prolonging the treatment time.
When prescribing dialysis, we often forget that the basic principle of postdilution hemodiafiltration is to filter plasma water out through the filter. Consequently, what is actually important is not blood flow but water plasma flow, and this is in relation to the hematocrit (7). Therefore, for all patients under ESA therapy, the hematocrit is also a modifiable factor, and is negatively associated with the achievement of a high volume target. When prescribing and adjusting the dose of ESA, nephrologists should also consider the dialysis dose delivery. In patients not reaching the threshold of adequacy, the option to maintain the hemoglobin level closer to the lower end of the KDIGO recommended target could also be considered.
Last but not least, an optimal filtration fraction can increase the possibility of achieving the minimum dose of the convection volume, making high-volume HDF feasible in cases where high blood flow rate is not attainable as well. However, it is difficult to prescribe and maintain the filtration fraction at a constant high level for the full length of the session. As a matter of fact, it should not be set to extremely high levels even for short period of time, since doing so may reduce the sieving coefficient of the membrane by fouling the membrane pores with proteins. On the other hand, despite the decrease in the sieving coefficient, by increasing the filtration fraction the ultrafiltered convection volume is increased and the mass of solute is removed as well. By using a more open membrane (with a higher sieving coefficient of β2-microglobulin) it is possible to reduce the convection volume required to achieve the same amount of solute removal. In addition, increases in albumin and protein levels due to hemoconcentration induce a high, circulating colloid oncotic pressure. This facilitates refilling from the interstitial space but in turn opposes ultrafiltration through the membrane. Therefore, from a strictly mechanistic view point it is difficult to make any conclusions regarding the optimal level of filtration fraction, since solute mass transfer is sensitive to the interactions between the sieving coefficient, membrane hydraulic permeability changes, and the total ultrafiltered volume.
In treating patients with acute kidney injury (AKI), regional citrate anticoagulation has been recommended by the KDIGO Clinical Practice Guidelines for AKI because this can prevent early filter clotting (22). In the present study, only standard and low-molecular-weight heparin have been used, but we would not exclude the possibility that citrate anticoagulation may be the future first option for maintaining membrane hydraulic permeability during the full HDF treatment.
This study has limitations associated with the fact that it is retrospective and observational in nature, and thus intended to create hypotheses that will need to be tested in appropriately designed clinical trials. In addition, while the almost exclusive use of 1 membrane type lends stability to the study design, it cannot be excluded that different membranes could have a stronger or weaker influence on the achievement of high substitution fluid volumes.
In conclusion, on the basis of the results from this observational study, the policy of the dialysis center in terms of blood flow, treatment time, filter size, and perhaps even hemoglobin targets, plays a key role in achieving high-volume HDF. All of these are modifiable factors. Further studies are needed to validate our model and evaluate the generalizability of our results outside the present network.
Footnotes
Financial support: No financial support was received.
Conflict of interest: All authors are employees of Fresenius Medical Care.