
Abstract
Introduction
Repairs of labral tears are performed for unstable tears, hip instability, and after detachment concomitant to the treatment of femoroacetabular impingement (FAI), but limited data is known about the strength of repair. This study evaluated the effect of simulated axial weight-bearing on suture anchor based repair of the acetabular labrum.
Methods
3 cadaveric pelvises underwent creation of a 1.5 cm anterior-superior labral tear in each hip. The tears were then repaired using 2 suture anchors per hip. Following repair, the hip joint underwent axial cyclic loading to 756 N, and were inspected for separation of the labrum from the acetabulum. The strength of the suture anchor repair was evaluated by testing load to failure, in-line with insertion.
Results
Upon visual examination, all 6 repairs remained fully intact following loading with no visible gap formation or damage at the repair site. In all cases an arthroscopic probe could not be inserted under the edge of the repair. The mean failure force of the 12 suture anchors, in-line with insertion, was 154 N ± 44 N.
Conclusions
Acetabular labral suture anchor repairs may be able to immediately withstand the physiological loads of axial weight-bearing. Labral repair may be able to tolerate axial weight-bearing immediately after repair, preserving the strength and integrity of muscles and soft tissues.
Introduction
Pathological tears of the acetabular labrum have been increasingly recognised as a cause of pain, dysfunction, and instability (1–3). In addition, there is increasing evidence that damage to the labrum is related to the development of osteoarthritis of the hip joint (4–6). The hip labrum appears to primarily function to seal the edge of the joint and has a relatively small role in load bearing (7–10). Loss of the sealing function of the labrum can lead to an increased rate of consolidation of the articular cartilage, resulting in increased contact stresses between the femoral and acetabular cartilage layers, and in some cases progression to arthritis (5, 6, 8).
Recent studies have demonstrated the favourability of labral repair when indicated (6, 11). Repair of the labrum is performed for unstable tears, hip instability, and after detachment concomitant to the treatment of femoroacetabular impingement (FAI) (11, 12). Restoration of the normal seal may slow or prevent the degenerative delamination of adjacent articular cartilage.
Initially, repair of the acetabular labrum was performed with the use of drill holes placed in the acetabular rim, similar to the original repairs of shoulder labral lesions (13). The use of tack-type or suture anchor repairs has been previously described (14). However, there is very little information regarding the mechanical strength of hip labral repairs. Therefore, it remains unclear whether these repairs can sustain the forces generated by full weight-bearing. We hypothesise that suture anchor repairs of the acetabular labrum have sufficient strength to withstand full weight-bearing due to the labrum's limited role in load-bearing. Increased information about the mechanical strength of hip labral repairs may help to better define postoperative guidelines and rehabilitation protocol.
The purpose of this study was to test the strength of suture anchor based repair of the acetabular labrum under conditions simulating a normal weight-bearing load.
Materials and methods
Specimen preparation and alignment
6 macroscopically normal lower extremity specimens were obtained from 3 donors (25-year-old male, 52-year-old male and 62-year-old male). Specimens with osteoarthritis or obvious abnormal morphology were excluded. Muscular soft tissues were removed, leaving the joint capsule, ligaments, and labrum intact.
Specimens were mounted to simulate axial weight-bearing in neutral extension (10). This was performed as follows. Both femoral shafts of each specimen were potted in 3′ schedule 40 PVC pipe using methyl methacrylate. A threaded stud was cemented in the distal end of the PVC pot. The femur was potted to allow loading of the hip in-line with the mechanical axis of the femur while in a neutral position (Line A in Figure 1). To facilitate alignment during potting, the pelvis was placed so that the anterior side of the pelvis lay on the table. The pelvis should rest on the anterior superior iliac spine and the pubic tubercle in this position. Anatomically these landmarks lie in a plane parallel to the frontal plane. A straight edge was used to create a line tangent to the right and left iliac crest (Line B in Figure 1). A line parallel to the longitudinal axis of the femur was drawn on the posterior side of the femur (Line C in Figure 1). In a neutral position the femur is adducted approximately 6°; therefore, a line 6° to Line C was created on the femoral shaft using a goniometer (Line D in Figure 1). Neutral position should be replicated when the 6° line (Line D in Figure 1) is perpendicular to Line B. During potting, the femur was positioned in the PVC pipe so that the longitudinal axis of the PVC pipe was parallel to the 6° line (Line D in Figure 1). In addition, the longitudinal axis of the pipe was positioned in-line with the mechanical axis of the femur (Line A, a line through the centre of curvature of the femoral head perpendicular to Line B).
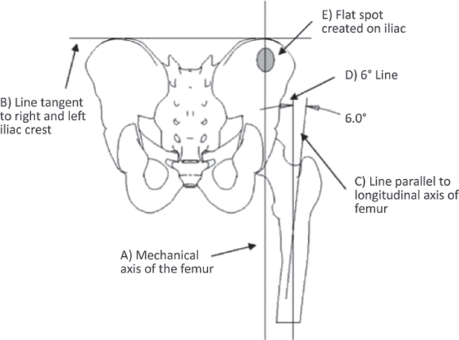
Schematic diagram describes a posterior view of the pelvis and femur in the neutral position tested in the study.
A flat spot was created on both sides of the iliac fossa using a PVC pot and bone cement to facilitate fixation of the pelvis in the INSTRON machine. The flat spot was created in-line with the mechanical axis of the femur in the neutral position as seen in Figure 1.
Creation of labral tears
Labral tears were created and repaired after potting to reduce unnecessary loading to the repairs during the potting process. The anterior-superior rim is the most common location for acetabular tears (15) and is the area reattached in labral repair for injury or in the treatment of femoroacetabular impingement. To simulate these tears, the joint capsule was removed and 1.5 cm of the anterior-superior labrum was sharply detached longitudinally from the acetabular rim, using a scalpel as seen in Figure 2A. If a small partial thickness tear was identified, the labral tear was completed to full thickness and then repaired.
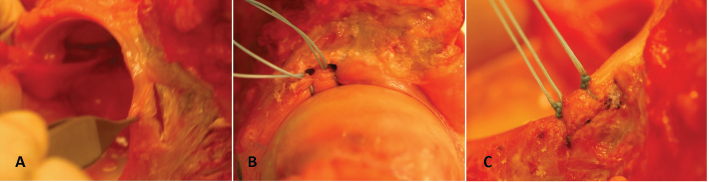
(A) Photograph shows the anterior-superior labrum detached from acetabular rim using a scalpel; (B) Photograph shows a labral repair using Bio-PushLocks; (C) Photograph shows a labral repair using Bio-SutureTaks.
Labral repair
Suture anchors were used to fixate the labrum to the acetabular rim. Labral repairs were performed by placing two suture anchors 5 mm apart, dividing the area of detachment into thirds. Matched pairs of repairs, using either 3.0 mm Bio-Composite Bio-SutureTaks or 3.5 mm Bio-PushLocks (Arthrex, Inc.), were performed in left and right hips of each specimen (FDA-approved for this use). Each specimen received a repair using each type of anchor. #2 FiberWire (Arthrex, Inc.) was used in both suture anchor groups, passed circumferentially around the tear. The tied sutures were secured with alternating half hitches. Figure 2 illustrates labral repair using Bio-PushLocks (2B) or Bio-SutureTaks (2C).
Securing and aligning the specimen
The pelvis and femur were secured in an inverted position in an Instron 8871 materials testing machine (Instron). The flat spot created on the iliac was clamped in an adjustable angle fixture so that the anterior-superior iliac spine and the pubic tubercle were all in a plane perpendicular to the base of the Instron machine (Fig. 3). The pelvis was aligned to be in neutral tilt in the coronal and saggital planes using a carpenter's bubble level. The right and left ischial tuberosity were level relative to each other. The potted femur was attached to the load cell by a vise in 12° of anteversion and 7° of varus with the mechanical axis aligned with the femoral head. The overall alignment was designed to simulate single-leg stance, which was chosen because of its extensive utilisation during daily activities such as walking and climbing stairs.
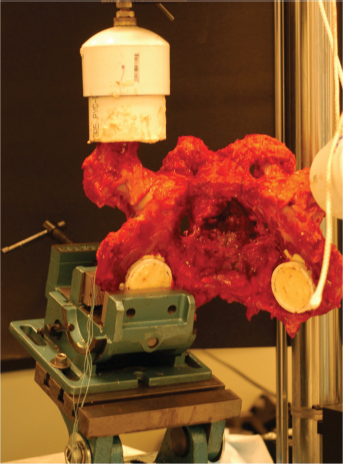
Photograph demonstrates a pelvis and femur mounted in the INSTRON machine in the inverted position tested in the study.
Mechanical testing
The femur was axially loaded to simulate loads placed on the hip joint during activity (10). The hip was preloaded to 132 N (the approximate load during toe-touch weight-bearing). Cyclic loading was conducted from 132 N to 756 N at 1 Hz, for 100 cycles. 756 N was chosen to simulate full weight-bearing of an average adult male (77 kg). Full weight-bearing would not be recommended during rehabilitation; however, it was tested to simulate worse-case loading scenarios. Post cycling, the joint was removed from the frame and the femoral head was distracted from the acetabulum and the labral repair was examined. Using a pair of digital calipers, gap displacement of the labrum relative to the acetabular rim was measured.
Following examination of the labral repair, pull to failure of the suture anchors was conducted. The flat spot created on the iliac of the pelvis was clamped in a vise-clamp fixated to an adjustable angle fixture. The angle of the vise-clamp was adjusted so that pull to failure in-line with the insertion of the suture anchors could be conducted. In-line axial pull of the suture would not be a physiological load applied to suture anchors used for labral repairs; however, it was chosen to test a worse-case scenario. The free ends of the suture strands were clamped in a pneumatic clamp specifically designed for fixating suture. Pull to failure was conducted at a constant displacement rate of 12 in/min. Data was collected at 500 Hz.
Results
All specimens had no gross evidence of osteoarthritis. 4 hips had small partial thickness tears at the articular side of the anterior-superior labrum, consistent with labral tears caused by cam-type femoroacetabular impingement. During examination of the acetabulum of specimen 05 08014, a 1.6 mm pre-existing tear was found in the labrum (Fig. 4A). The pre-existing tear was repaired using Bio-SutureTaks. In this specimen some delamination of the lunate cartilage was present inside the acetabulum (Fig. 4A). 2 hips had minimal changes at the femoral head-neck junction and 2 hips had a bony prominence at the femoral head-neck junction. All hips had a normal centre-edge angle (≥25°).

(A) Photograph shows a specimen with pre-existing tear and associated articular cartilage lesion after repair and cycling; (B) Photograph shows a labral repair after cycling: labrum repaired with Bio-PushLocks; (C) Photograph shows a labral repair after cycling: labrum repaired with Bio-SutureTaks.
Following the creation of the 1.5 cm detachment, the mean amount of displacement of the labrum from the edge of the acetabulum was 3 mm.
Visual inspection following cyclic loading demonstrated no obvious changes at the repair site (Fig. 4B, C). In all cases, an arthroscopic probe (diameter 1 mm) could not be placed under the edge of the repair.
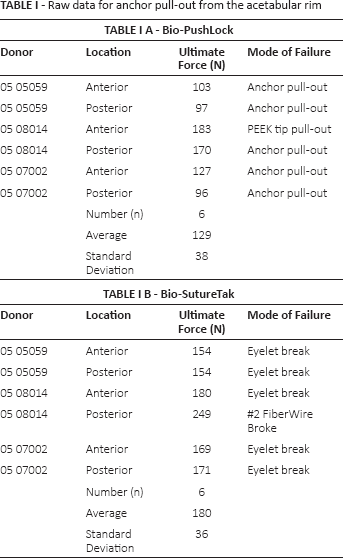
The average pull-out force for all 12 suture anchors from the acetabular bone was 154 N ± 44 N. Bio-SutureTaks had a significantly (p≤0.009) higher pull-out strength than Bio-PushLocks (180 N ± 36 N vs. 129 N ± 38 N). No significant difference between anterior and posterior anchor pull-out was noted (153 N vs. 156 N). The data for each individual specimen can be seen in Table IA, B.
Raw data for anchor pull-out from the acetabular rim
Discussion
There is increasing interest in the treatment of labral pathology of the hip. It is clear that damage to the labrum can cause pain and loss of function. The loss of the sealing effect of the joint may also result in the development of articular cartilage damage and contribute to accelerated osteoarthritis of the hip.
Most labral tear lesions likely occur as the result of femoroacetabular impingement (FAI), which is the repetitive compression from the femoral head and neck on the anterior/anterior-superior labrum. This type of impingement typically occurs with the hip in ≥90° of flexion and internal rotation, but may occur if there are morphological abnormalities of the femoral head-neck junction. In several of our specimens, the combination of a small labral tear, articular cartilage damage and impinging bone at the femoral head-neck junction was seen.
Although the labrum adds to the area of the hip joint socket (16), it is unclear what loads are placed on the anterior-superior labrum during single leg stance or the gait cycle (9, 10) Konrath et al (10) concluded that “In contrast to the meniscus of the knee, the acetabular labrum does not increase contact area, distribute load, or reduce contact stresses in the hip.” Henak et al (9) found that the acetabular labrum supports only 1-2% of the total load placed on the hip during daily activities. Safran et al (17) determined that the greatest strain in the intact labrum in full extension is laterally and strain is highest in the anterior labrum in flexion and adduction. However, the overall magnitude of average strain in the labrum was extremely small (≤0.04 mm). Thus, our results are consistent with Konrath et al (10), Henak et al (9), and Safran et al (17), in that no changes at the repair site were seen despite the repeated loads applied to the hip joint in our described axial positioning. This suggests that labral repairs may have sufficient initial strength to withstand loads associated with axial weight-bearing.
We recognise that this study did not evaluate the hip through a range of motion. Data from Henak et al (9) and Safran et al (17) suggest that magnitude strain in the labrum under higher degrees of flexion is quite low, suggesting that these results are applicable through a relatively broad range. The highest negative displacement of the normal labrum in 90° of hip flexion with abduction and internal rotation was 0.014435 mm. Axial loading to simulate body weight was performed due to recognition that changing the position was unlikely to change the result, given the findings of Safran et al (17).
During these normal activities, the labrum appears to be only minimally loaded. The postoperative recommendations following labral repair are therefore relatively precautionary, with respect to protecting the repair. Typically, they require limited weight-bearing for 4-8 weeks, limited rotation, and no flexion ≥70° (18). Patients are advised to avoid placing excessive load on the repair until biological healing of the damaged tissue can occur. The findings in this study suggest that post-operative weight-bearing may be able to be progressed earlier.
Increased postoperative weight-bearing could help patients maintain normal gait patterns as well as preserve the strength and integrity of muscles and other soft tissues. Further clinical investigation is necessary to determine whether altering rehabilitation protocol and postoperative recommendations is advisable.
We feel that suture anchor-based repair of acetabular labral tears has sufficient initial strength to withstand weight-bearing loads in the postoperative period. It is important that if the mechanism of injury is felt to be femoroacetabular impingement, it be concurrently treated either with open or arthroscopic procedure, otherwise the potential for re-tear exists (19). In the dysplastic hip, a pelvic osteotomy to redistribute the load to the acetabulum may be necessary (15, 20).
In addition, the loads on the labrum of a dysplastic hip are likely to be substantially higher than in the normal joint, since the normal load transmission through the acetabular roof is significantly decreased (9). This study was not designed to evaluate this condition. It is possible that in a dysplastic hip, greater load transmission across the repair would occur, leading to gap formation or fracture of the repair.
The weaknesses of this study include the fact that it was a cadaveric study and confined to anatomically normal hips. Also, the decision was made to use axial loading, which did not simulate the full range of gait. We feel that this study still demonstrates the effects of early weight-bearing on acetabular labral repair and may provide a guide on postoperative and rehabilitation protocols.
Conclusion
Acetabular labral suture anchor repairs may be able to immediately withstand the physiological loads of axial weight-bearing. Labral repair may be able to tolerate axial weight-bearing immediately after repair, preserving the strength and integrity of muscles and soft tissues. Further clinical investigation is needed to determine whether postoperative weight-bearing is advisable immediately following acetabular labral suture anchor repairs.
Footnotes
Financial support: Specimens and equipment were provided by Arthrex.
Conflict of interest: JLK has received funding from Aesculap, Aperion and Arthrex.