
Abstract
Introduction
In recent years a variety of short-stems have been introduced. Stable osteointegration is a key factor for a satisfactory long-term result. The purpose of this study was to evaluate postoperative radiological alterations and subsidence, as a result of using a newly developed device, over a 2-year follow-up.
Methods
216 short-stems were implanted in combination with a cementless cup. Patients were allowed full weight-bearing on the first day postoperatively. Pre- and postoperative x-rays were done using a standardised technique. Radiological alterations, such as bone resorption, radiolucency, osteolysis and cortical hypertrophy were detected and located using modified Gruen zones, and subsidence was measured via a conventional digital technique over a 2-year follow-up. In addition, Harris Hip Score (HHS), rest pain and load pain on the visual analogue scale (VAS) were assessed respectively.
Results
At 2-year follow-up 6 stems (2.9%) showed nonprogressive radiolucent lines with a maximum width of 2 mm. Resorption of femoral bone stock was detected in a total of 8 cases (3.9%). Femoral cortical hypertrophy was seen in a total of 9 hips (4.4%). No patient showed osteolysis. A measureable subsidence of at least 2 mm was observed in a total of 15.7% (32 cases) after 6 weeks, corresponding to an initial settlement given full weight-bearing ambulation. Only 1.1% (2 cases) showed further progression at the 6-month follow-up, whereas at the 1- and 2-year follow-ups no further subsidence was observed. After 2 years HHS was 98.1 (65.0-100.0), rest pain on the VAS was 0.2 (0.0-7.0) while load pain was 0.4 (0.0-7.0).
Conclusions
The results of this radiographic analysis give support to the principle of using metaphyseal anchoring, calcar guided short-stems. The low incidence of bony alterations after a follow-up of 2 years indicates a physiological load distribution. After mild initial subsidence a stable osteointegration can be achieved over time.
Introduction
In recent years, a steadily increasing number of young and active patients have received total hip arthroplasty (THA). It is well known that young patients face higher risks of implant failure (1), and thus in the future, the quantity of revision surgery will multiply. Preservation of bone therefore becomes more important. Most, if not all, femoral components cause a reduction of cortical strain and bone mineral density (BMD) especially in the proximal femur (2, 3). Radiological analysis of several different stem designs showed bony alterations with increasing resorption of the proximal femoral bone due to stress shielding (4–5–6). The clinical relevance of this, however, remains unclear (7). Also, distal femoral cortical hypertrophy as a result of abnormal stress distribution in the loaded femur is a common phenomenon in different stem models, potentially causing thigh pain (8–9–10–11). The appearance of radiolucent lines around the component might be evidence of subsequent loosening (12), although this has not yet been confirmed. Recent studies indicate that adaptive bone remodeling may progress even after long-term follow-up (13), which is presumed to affect long-term femoral component stability.
One of the aims of developing a short femoral implant was to preserve proximal bone and soft tissue and achieve satisfactory osteointegration. Similar to proximally-only coated stems the reduction of diaphyseal fixation may lead to the application of a more physiological load (14–15–16). Recent studies indicate that short-stem implants reproduce a stress distribution at the level of the proximal femur more similar to the physiological femur, limiting the stress-shielding that occurs with fully coated cementless stems (17). Short-stems, by preferentially loading the proximal femur, may retain more proximal bone mass over time than distally anchoring stems (9).
Most concepts follow the idea of a proximal force induction in the metaphyseal and calcar region. Since a short-stem inherently will have less bone contact, to assure stability, the contact area of the endosteal cortex of the calcar has to be increased (8). However, there is a large variety of different models of short-stems, differing in design and function.
Early clinical results, especially of the newest generation of neck preserving, calcar guided short-stem implants are excellent (18, 19). Recent studies also show a good possibility of reconstructing normal hip anatomy in terms of maintaining femoroacetabular offset and a high variety of caput-collum-diaphyseal angle (CCD) (16, 20, 21). At present there is almost no data on the long-term outcomes of short-stems. A major concern in reducing diaphyseal fixation of the femoral stem is still the concomitant reduction of implant stability and the increase of interface micromotion which, by interfering with osteointegration, might increase the risk of implant loosening (22). Therefore, it is of great importance to evaluate these implants at the early stages in order to obtain data that may help predict their survival. The reaction of the environmental bone may be an indicator for force distribution and the bony integration of cementless short-stems and may therefore help to predict long-term outcome, based on short-term results.
The aim of this study was to analyse primary stability and the most common radiological alterations in 216 prospective unilateral and bilateral cases operated on with a neck preserving, calcar guided short-stem up to 2 years postoperatively.
Methods
In the present prospective study, 216 consecutive cases in 162 patients (54 bilateral cases) were included.
In all patients the meta-diaphyseal anchoring short-stem Optimys (Mathys Ltd.) was used. It is a femoral neck preserving prosthesis made of titanium, which is available in 12 different sizes, with a 12/14-mm cone and with 2 different offset versions. The special stem design allows good bone contact at the distal lateral cortex and the proximal medial cortex. The rough titanium plasma sprayed coating is supposed to offer secure anchorage in the bone. In addition, the stem contains an overlying calcium phosphate coating in order to promote rapid osteointegration and achieve secondary stability.
The prosthesis is aligned along the proximal medial cortex and the calcar femorale. Anchoring is based on the fit-and-fill principle, but can be done as classic 3-point anchoring in some cases. In addition, the triple conical shape is thought to achieve good primary stability and prevent migration. The greater trochanter region remains intact.
The Optimys stem was combined with cementless press-fit cups (n = 177 Fitmore, Zimmer; n = 39 RM Pressfit vitamys, Mathys Ltd.) with a ceramic-polyethylene bearing couple. The implantations were performed at the Orthopaedic Clinic at St. Josef's Hospital Wiesbaden, Germany, in the years 2010 to 2012. All operations were performed through a minimally invasive, anterolateral approach using a standardised surgical technique (23). Mean patient age was 63.0 (range 33.4-88.0) years. 73 women and 89 men were operated on. In 54 patients, the treatment was bilateral simultaneously, 108 patients were operated on unilaterally. The indications for implantation were as follows: 91.7% (n = 198) primary osteoarthrosis, 5.1% (n = 11) femoral head necrosis, 2.3% (n = 5) congenital dysplasia and 0.9% (n = 2) secondary osteoarthrosis. All patients started physiotherapy and were allowed full weight-bearing ambulation on the first day postoperatively.
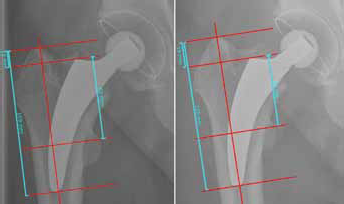
All patients underwent pre- and postoperative digital anteroposterior imaging with a standardised technique. A positioning splint with 20° internal rotation of the hip joint was used in order to achieve a standardized and reproducible image during follow-up. The x-ray tube was positioned at a distance of 1 m from the table in a perpendicular position. Follow-up included a maximum of 5 postoperative radiographs: during hospital stay, 6 weeks, 6 months, 1 year and 2 years postoperatively. Subsidence was digitally measured in a standardised technique from the highest point of the greater and lesser trochanter to the most lateral point of the stem-shoulder according to Bieger et al (24) and Cordero-Ampuero et al (25). Therefore, a coordinate system was digitally included in every postoperative image on each hip. First, femoral axis was defined as vertical axis, secondly 4 horizontal axes perpendicular to the vertical axis were lined at the tip of the greater trochanter, the lateral shoulder of the stem, a prominent part of the lesser trochanter and the distal tip of the prosthesis (Fig. 1). The measurements were done on every follow-up image and subsidence was calculated. According to Bieger (24), resulting measurements of at least 2 mm were considered as reliable subsidence. Using a modification of the zones described by Gruen (26), bone resorption, radiolucency, osteolysis and cortical hypertrophy were analysed on the standardised radiograph after 24 months (Figs. 2, 3). To detect bone resorption, the proximal femoral bone was scanned in order to find areas with enhanced bone-transparency and thinned or resorbed trabaeculae according to the Singh-Index (27). Grades 1-3 were considered to be bone resorption. Lucent lines were detected and the maximal width was measured. Cortical bone width was measured preoperatively and during follow-up in order to detect any increase or decrease of width. To reduce interobserver error, radiological evaluation was performed retrospectively by 1 experienced examiner (KPK), who had not been involved in surgery. Intraobserver variability was not measured. All measures were obtained with the digital radiograph templating software MediCAD (Hectec). Magnification error was addressed using a ball with known diameter as a scaling factor or the known diameter of prosthetic femoral head as an internal reference.

Measurement of subsidence using digitally included coordinate System. Left: postop; right: 6 weeks follow-up. In this case a subsidence of 2 mm after 6 weeks was measured.
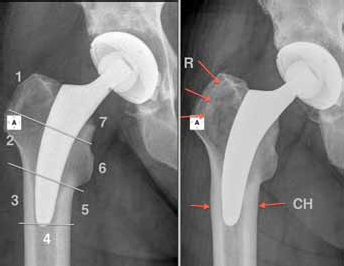
Left: postop; modification of the Gruen zones; right: 2-year follow-up. Resorption of femoral bone in zone 1 and 2 (R) and cortical hypertrophy in zone 3 and 5 (CH).

Left: postop; modification of the Gruen zones; right: 2-year follow-up; Radiolucent lines in zone 1 and 7 (LL) and cortical hypertrophy in zone 3 and 5 (CH).
In addition, HHS as well as rest pain and load pain on the VAS were assessed during follow-up.
Statistical analysis
Data were described by mean and range. For the comparison of HHS and pain scores on VAS preoperative vs. 2 years a Wilcoxon signed-rank test (2-sided) for paired data was used. P-value <0.05 was considered as indication for difference. All statistical analyses were performed using SPSS version 21.0 (SPSS Inc.).
Ethical approval
This study conforms to the Helsinki Declaration. The study was approved by the Freiburg Ethics Commission International Ethics Committee (10/04/2010) (feki Code: 010/2071).
Results
Of the initially included 216 cases, 11 cases were lost to follow-up after 2 years. 4 of these patients are known to be deceased with the prosthesis in situ. A clinical follow-up could only be performed in 1 patient (Fig. 4). Thus, 204 cases in 152 patients could be analysed after 2 years. The mean follow-up time was 30.4 (range 23.0-49.2) months. 1 patient had to be revised due to early deep infection with change of head and inlay without long-term consequences. 1 patient showed an intraoperative crack of the greater trochanter, also without any clinical malfunction. No therapy was required. 1 case of deep vein thrombosis (DVT) was reported despite regular medical prophylaxis, and was treated successfully.
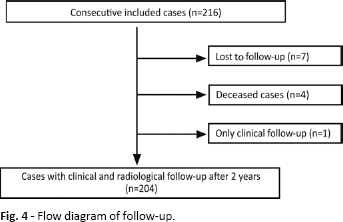
Flow diagram of follow-up.
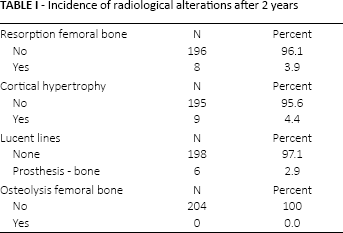
At the 2-year follow-up 6 stems (2.9%) showed radiolucent lines with a maximum width of 2 mm. Radiolucent lines occurred 5 times in Gruen zone 1 and once each in zones 3, 4, 5 and 7 (Fig. 3) (Tab. I). Resorption of femoral bone stock was detected in a total of 8 cases (3.9%), whereas all of these occurred in Gruen zones 1, 2 and 7 (Fig. 2) (Tab. I). Femoral cortical hypertrophy was seen in a total of 9 hips (4.4%) after a follow-up of 24 months. It was localised exclusively in Gruen zones 3 and 5 (Figs. 2, 3) (Tab. I). Osteolysis was not seen in any patient at any time-point.
Incidence of radiological alterations after 2 years
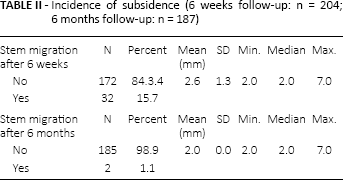
15.7% of all cases included showed measurable subsidence of 2 mm or more after 6 weeks (Fig. 1). Only 1.1% of these showed further progression in the next follow-up. After 6 months there was no further progression of subsidence detected in any of the patients included. Mean subsidence was 2.6 (range 2-7) mm after 6 weeks. The maximum subsidence was 7 mm in 2 cases (Fig. 5) (Tab. II). HHS improved greatly from 45.8 (range 7.0-88.0) preoperatively to 98.1 (range 65.0-100.0) after 2 years (p<0.001). While preoperative rest pain on the VAS was significantly reduced from 5.3 (0.0-10.0) to 0.2 (0.0-7.0) (p<0.001), load pain could be lowered markedly from 7.7 (0.0-10.0) to 0.4 (0.0-7.0) (p<0.001).
Incidence of subsidence (6 weeks follow-up: n = 204; 6 months follow-up: n = 187)
Measurement of subsidence using digitally included coordinate System. Left: postop; right: 6 weeks follow-up. In this case a subsidence of 7 mm after 6 weeks was measured. The left figure shows undersizing with missing cortical contact in the distal part of the stem.
Discussion
In the present study we found a low incidence of typical radiological alterations in patients treated with the investigated short-stem after 2 years. However, some patients (4.4%) showed typical patterns of remodelling with the appearance of cortical thickening predominantly in the distal part of the stem. Resorption of femoral bone stock was detected in only 3.9%, mainly in the proximal part of the stem. After 2 years, 2.9% of the cases showed radiolucent lines up to 2 mm without progression and without any clinical consequences. Subsidence of 2 mm and more occurred in 15.7%, although there was almost no further progression after 6 weeks.
Femoral component stability in cementless THA depends on periprosthetic bone remodelling. Stem design is an important factor influencing bone remodelling; however, to date the design that promotes the most bone remodeling is unclear (28). While many surgeons presume proximally coated stems, or cemented stems, have a lower incidence of proximal bone remodelling and stress shielding accompanied by distal cortical hypertrophy and thigh pain than fully coated stems, this remains controversial (29–30–31). Kinov et al (30) followed up 98 proximally coated THAs radiologically for an average of 33 months and reported thigh pain in 13%, cortical thickening in 14% and stress-shielding with proximal osteopenia in 17% of the patients. McAuley et al (32) analysed a series of 507 extensively coated THAs in a 5-year follow-up and found detectable osteolysis in 11.3% and that stress-shielding was common (25%). In a comparison of cementless and cemented THAs in a 20 year follow-up carried out by Corten et al (33), radiographs showed evidence of mild stress-shielding around 95% of the cemented stems and around 88% of the cementless stems.
Over the past years many studies have been presented concerning the outcome of different short-stems. Some of these studies focused on clinical outcome (34–35–36–37), some also focused on radiographic changes in bone density, bony alterations and remodeling (15, 19, 38–39–40–41).
In an in vitro comparison of the investigated short-stem to a fully-coated conventional straight-stem Bieger et al (42) showed that proximal load transmission was more normal in the short-stem, though both implants showed stress shielding in Gruen zones 1 and 7. Primary stability of the short-stem prosthesis was not negatively influenced compared to the straight-stem. Furthermore, the proximal femoral strain pattern was more normal after insertion of the short-stem prosthesis. Cinotti et al (22), in a study of 148 patients receiving a short-stem, came to the conclusion that the limited periprosthetic bone remodelling observed after a minimum of 9 years follow-up suggests this type of implant may improve mechanical stresses on the host bone compared to standard-stems requiring diaphyseal fixation. Logroscino et al (39) measured the changes of periprosthetic bone mineral density (BMD) with a DEXA-device and evaluated signs of stress-shielding with standard radiographs after implantation of 19 Proxima (DePuy, Johnson & Johnson) and 12 Nanos (Smith & Nephew) stems. Both implants preserve metaphyseal bone stock and increase periprosthetic BMD. They showed satisfactory osteointegration after only 1 year, and therefore present an excellent alternative to traditional straight-stem hip prostheses (39). However, the concomitant reduction of implant stability is still a major concern in reducing diaphyseal fixation of the stem (22, 43).
The investigated short-stem in the present study seems to provide good early osteointegration. We did not observe any aseptic loosening of the implant, nor did we find osteolysis suggesting stem instability. None of the radiolucent lines found were progressive.
One of the most important issues in achieving long-term fixation seems to be the prevention of early continuous stem migration (44–45–46–47). Stem subsidence greater than 5 mm has been reported in up to 6.4% in various cementless standard-stems and short-stems (48–48–49–50–51–52). In the present series, minimal stem subsidence only was observed in the first postoperative weeks in 15.3% of cases. In most cases the subsidence was about 2 mm. As reported by other authors (9, 48, 51), it seems that all kinds of femoral components may need an initial settling-in period within the host bone to gain mechanical stability and subsequent metaphyseal osteointegration of the implant, particularly given the allowance of full weight-bearing on the first day postoperatively. Gustke (9) has reported that of the first 100 implanted Fitmore short-stems an initial subsidence of ≥2 mm was detected in 34%. While these high numbers would seem worrisome it seems that the migration only continued to a position of ultimate stability. Further progression was not seen. Also, in the present study no clinical correlation was obvious. In the whole collective, clinical results are very satisfying, and HHS showed excellent results after 2 years. Pain scores at that time are remarkably low. The 2 cases with measured subsidence of 7 mm seem to be a consequence of “undersizing” during stem implantation. The missing lateral cortical contact in the postoperative radiological follow-up might lead to initial subsidence after ambulation until mechanical stability with lateral cortical contact is achieved (Fig. 5). No correlation with the clinical outcome could be found in those patients. Long-term follow-up will be performed in order to detect, if, despite late stabilisation in the femoral bone, a fibrous union on the interface might jeopardise implant survival.
There are limitations to the present study. First is the short follow-up of 2 years. Although only long-term results should be considered valid, initial evaluation of bony alterations is necessary to identify undesirable results (53). Early migration analysis may allow a prediction of implant survival (47) and the reaction of environmental bone in the early stage may help to predict the long-term outcome. Second, the method used to measure subsidence lacks some accuracy in comparison to radiostereometric analysis (RSA) or EBRA (Einzel-Bild-Röntgen-Analyse) analysis. Nevertheless, Bieger et al (24) recommended the greater and lesser trochanter as well as the shoulder of the implant as reference structures for the evaluation of implant subsidence on plain radiographs. Accuracy was shown to be between ±1.3 mm and ±4.6 mm depending on the different distances measured and the usage of the conventional or digital method. Therefore, according to Bieger et al (24) subsidence of an implant should not be assumed before a determined difference of 2 mm as a minimum. In the near future an EBRA evaluation will be done using the investigated stem to confirm the results. Also, the radiological method used to evaluate femoral bone loss and stress-shielding is rather inaccurate compared to the usage of DEXA scans. However, given the size of the collective this method would have resulted in intense effort and costs. Future investigations will have to verify the results. As a third limitation, since the Orthopaedic Department of St. Josefs Hospital Wiesbaden is a reference clinic of the investigated stem, the results have to be confirmed by other clinics.
Conclusion
The low incidence of bony alterations after a follow-up of 2 years indicates stable and durable osteointegration and normal load distribution of the investigated short-stem. Almost no progression of very mild initial subsidence underlines these findings. The results of this radiographic analysis give support to the principle of using metaphyseal anchoring, calcar guided short-stems. Future investigations should evaluate whether these results are maintained at a long-term follow-up.
Footnotes
Financial support: Mathys Ltd. Switzerland funded the cost for additional outpatient radiological follow-up examinations.
Conflict of interest: Prof. Dr. Joachim Pfeil and Prof. Dr. Werner Siebert have a contract as medical advisor to Mathys Ltd. Bettlach, Switzerland. All other authors declare that they have no conflict of interests.