
Abstract
Purpose
To determine whether gender, femoral head size, acetabular inclination, and time since surgery predicted high blood metal ion concentrations following Birmingham Hip Resurfacing (BHR).
Methods
BHR patients with unilateral bearings at one specialist centre with blood cobalt and chromium concentrations measured up to May 2013 were included. This comprised a mixed (at-risk) group including symptomatic patients and asymptomatic individuals with specific clinical and/or radiological findings. Blood sampling was at a mean of 7.5 years (range 1-15.4 years) postoperatively.
Results
Of 319 patients (mean age 49.3 years; 53% male), blood metal ions greater than 7 µg/l were observed in 9% (n = 28). Blood metal ions were significantly higher in females (p<0.001), femoral head sizes ≤48 mm (p<0.01), and cup inclinations >55° (p<0.001). Linear regression demonstrated femoral head size was responsible for the highest proportion of variance in blood metal ions (cobalt p<0.001, R2 = 8%; chromium p<0.001, R2 = 11%). Analysis of femoral head size and inclination together demonstrated 36% of BHRs with head sizes of 38-44 mm and inclination >55° had blood metal ions >7 µg/l. BHR 10-year survival for this at-risk group was 91% (95% confidence intervals 86.0%-95.0%) with 30 hips revised.
Conclusions
If blood metal ions are used to screen hip resurfacing patients for adverse reactions to metal debris it is recommended those with small femoral head sizes (38-44 mm) and high acetabular inclinations (>55°) are targeted. These findings require validation in other cohorts as they may not be applicable to all hip resurfacing devices given the differences in radial clearance, coverage arc, and metallurgy.
Introduction
Metal-on-metal hip resurfacing can produce excellent clinical outcomes in young individuals with hip arthritis up to 14 years postoperatively when patients and implants are carefully selected (1-2-3-4-5). Despite these promising results, some patients will develop problems related to high bearing wear (6, 7). Patients who develop adverse reactions to metal debris (ARMD) may require revision surgery, though short-term outcomes following revision are reportedly poor (8-9-10). Outcomes following revision may be influenced by the degree of soft-tissue destruction. Therefore, early intervention may result in more favourable outcomes following revision (11). To achieve this, patients who develop ARMD must be identified early using appropriate investigations when the condition is suspected.
Blood metal ion concentrations are an accepted surrogate marker of metal-on-metal bearing wear, and therefore can be useful in identifying patients with ARMD (12). A blood test is quick and minimally invasive. Recommendations from the Medical and Healthcare Products Regulatory Agency (MHRA) suggest that provided the implant has not been recalled blood metal ion sampling should only be performed in patients with metal-on-metal hip resurfacings who are symptomatic (13). However, ARMD lesions have been observed in asymptomatic patients with well-functioning hip resurfacings (14, 15).
If symptoms are not helpful in identifying patients with ARMD there are 2 options. The first would be to perform blood metal ion sampling in all hip resurfacing patients. This is unfavourable because most patients will have negative results, yet will suffer unnecessary anxiety and concern. Also there would be huge cost and resource implications for institutions. The second strategy would involve targeted screening of patients at increased risk of developing ARMD, such as female patients, those with small femoral component sizes, acetabular components outside the recommended ‘safe-zone’, and resurfacings performed for hip dysplasia (7, 16-17-18-19). It would be beneficial to determine which combination of factors optimally identifies hip resurfacing patients at risk of developing ARMD so this subgroup can be screened using blood metal ion sampling.
This study aimed to determine whether high blood metal ion concentrations following Birmingham Hip Resurfacing could be predicted by gender, femoral component head size, acetabular component inclination, or time since index operation.
Methods
Study design, inclusion criteria, and patient demographics
This prospective cohort study was undertaken at a single specialist arthroplasty centre and was registered with the institutional review board. Birmingham Hip Resurfacings (BHRs; Smith & Nephew, Warwick, United Kingdom) implanted at this centre between August 1997 and May 2013 with measured blood metal ion concentrations were eligible for inclusion. Information regarding patient selection and operative technique for BHR surgery performed at this institution has been described (20).
During the study period 3295 BHRs were implanted. Blood metal ion sampling was performed in 606 patients with 738 BHRs (22%). Patients with bilateral hip replacements were excluded (378 hips) because of difficulties associated with interpreting raised blood metal ions in the presence of 2 hip bearings (5, 11). Patients were also excluded if they met any of the following criteria: the BHR was revised prior to blood sampling (37 BHRs excluded); blood sampling was less than 1-year postoperatively (2 BHRs excluded); no information was available on acetabular inclination angle (2 BHRs excluded). Therefore 319 BHRs were eligible for final study inclusion from the 738 BHRs (43%) with blood metal ions measured during the study period (Tab. I). Operations were performed by 12 surgeons, with 1 designing surgeon (RBCT) performing most (n = 87; 27%). Procedures were performed using a posterior (90%) or antero-lateral (10%) surgical approach.
Summary of the study cohort
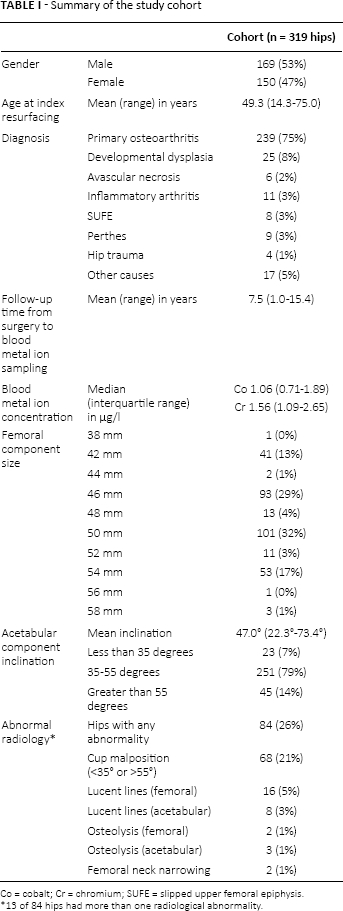
Co = cobalt; Cr = chromium; SUFE = slipped upper femoral epiphysis.
13 of 84 hips had more than one radiological abnormality.
Description of follow-up routine
This institution's standard follow-up regimen is to review all patients at 6 weeks postoperatively in clinic, and subsequently at 1, 5, 10, and 15 years following BHR surgery. Each consultation consists of clinical examination, anteroposterior pelvic radiographs, and completion of the Oxford Hip Score (OHS) questionnaire (21). Blood metal ion sampling was not performed prior to 2010.
After the MHRA published concerns regarding ARMD associated with metal-on-metal hips (13, 22) this institution deemed it unnecessary to recall all BHR patients for clinical review because: 1) good outcomes with this device have been achieved at numerous centres (2-3-4-5); 2) the BHR has significantly lower failure rates for ARMD compared to other devices (7, 23); and 3) the BHR has not been recalled.
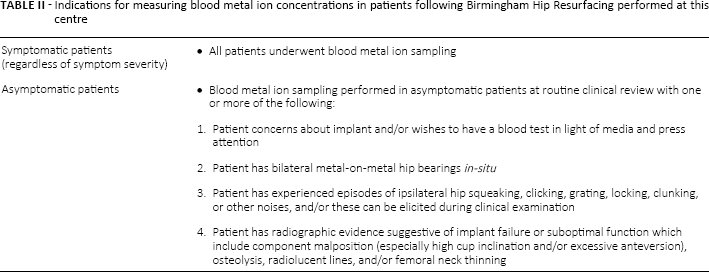
In 2010 all patients who had undergone BHR surgery at this centre were contacted by post. All patients with hip symptoms regardless of severity attended an urgent clinical review, which included blood metal ion sampling. The remaining asymptomatic patients were reviewed according to the standard follow-up intervals. The indications for measuring blood metal ions in asymptomatic BHR patients at this centre (Tab. II) have evolved since 2010 due to the expanding evidence-base (11, 24). The present cohort (n = 319) therefore represents a mixed (at-risk of ARMD) group of symptomatic patients and asymptomatic individuals with specific clinical and/or radiological findings.
Indications for measuring blood metal ion concentrations in patients following Birmingham Hip Resurfacing performed at this centre
Blood metal ion sampling
Whole blood was collected for blood metal ion analysis. Venous blood was obtained using a 23-gauge stainless steel needle connected to a vacutainor system (Vacuette; Greiner Bio-One GmbH, Kremsmünster, Austria) and collected in trace element tubes containing sodium heparin. All samples were then transported to an external laboratory approved by the MHRA for blood metal ion analysis. Cobalt (Co) and chromium (Cr) concentrations were measured in all samples using an inductively-coupled plasma mass spectrometer (Agilent 7500 cx, Agilent Technologies Inc., Santa Clara, US). The limit of detection and the reporting limit were 0.06 µg/l and 0.6 µg/l respectively. Blood metal ions were considered raised if Co and/or Cr concentrations were greater than the MHRA upper limit of 7 µg/l (13).
Description of outcome measures
All study data except for radiographic data were extracted from the institution's prospectively maintained database (MySQL database, Oracle Corporation, Redwood Shores, California). The database contains details on patient demographics, surgery performed, blood metal ion concentrations, and any complications during follow-up.
Acetabular component inclination was measured in each anteroposterior pelvic radiograph using the teardrop line for reference as described (25). Acetabular inclination was measured by 2 authors (GSM and DJD) after excellent inter-observer and intra-observer reliability was confirmed following both authors measuring a sample of 30 such radiographs (no significant difference between the surgeons’ measurements were found with p = 0.82 and intra- and inter-observer 95% limits of agreement of −2.2° to 1.6° and −2.5° to 3.5° respectively; 95% confidence intervals for intraclass coefficients were 0.994-0.998 and 0.984-0.994 respectively) (26). All radiographs were assessed for osteolysis, radiolucencies, and femoral neck thinning as previously described (27-28-29).
Statistical analysis
All analyses were performed using R (30). Linear regression and t-tests were performed to investigate relationships between the base 10 logarithm (log) of blood metal ion concentrations and the 4 covariates (gender, femoral component head size, acetabular component inclination, and time since index operation). The logarithm was necessary to transform the asymmetric blood metal ion distributions so that the residuals in the regression models were more normally distributed; this assumption was checked by examining the regression diagnostic plots. The logarithmic transformation has often been used in previous studies analysing similar data (31, 32). Adjusted R2 was also calculated to give the percentage of variance in log blood metal ion concentrations explained by the models. Femoral head sizes were grouped (38/42/44 mm (n = 44), 46/48 mm (n = 106), 50/52 mm (n = 112), 54/56/58 mm (n = 57)) for t-testing with multiple comparisons. Similarly, acetabular inclination angles were grouped (<35° (n = 23), 35°-55° (n = 251), >55° (n = 45)) as previously described (18). The Holm method was used for adjusting the p-values in this t-testing to allow for multiple comparisons.
Cumulative BHR survival was determined using the Kaplan-Meier method. The endpoint for survival analysis was revision surgery, defined as removal or exchange of either the femoral or acetabular component, or both. Patients not undergoing revision surgery were censored after their last contact with the hospital or after death. A Cox-proportional hazards model was used to compare differences in BHR survival between patients with high (>7 µg/l) and low (≤7 µg/l) blood metal ions. A p-value of less than 0.05 was considered statistically significant with confidence intervals (CI) set at the 95% level.
Results
Median (interquartile-range) blood Co and Cr concentration for the 319 unilateral BHR patients were 1.06 µg/l (0.71-1.89 µg/l) and 1.56 µg/l (1.09-2.65 µg/l) respectively. In the patients with bilateral implants excluded from further analysis, median (interquartile-range) blood Co and Cr concentrations were 2.24 µg/l (1.24-3.95 µg/l) and 2.34 µg/l (1.61-4.42 µg/l) respectively. Log blood metal ion concentrations were significantly higher in the bilateral group compared to the unilateral group (p<0.00001 for both Co and Cr).
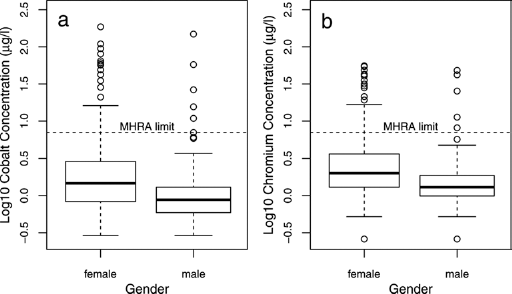
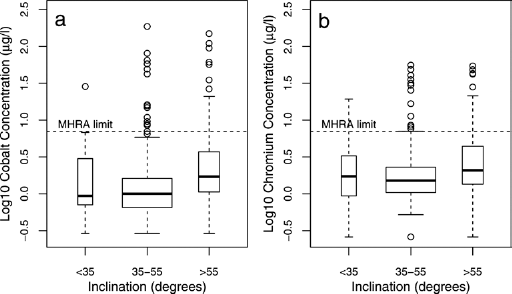
Of the 319 unilateral BHRs, blood metal ions greater than recommended thresholds of 7 µg/l were observed in 28 patients (9%). Blood metal ions greater than 7 µg/l were observed in 15% (22/150) of females compared to 4% (6/169) of males. Females had significantly higher log blood metal ion concentrations than males (t-test with p<0.001 for both Co and Cr; Fig. 1).
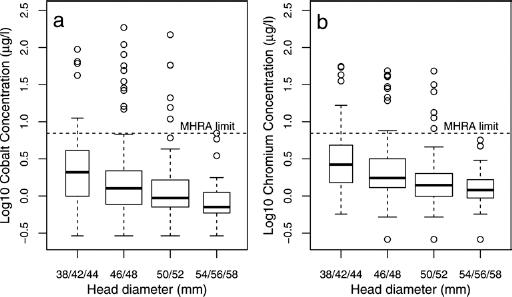
The 38/42/44 mm and 46/48 mm femoral head size groups had significantly higher log blood metal ion concentrations than the 50/52 mm and 54/56/58 mm groups (p<0.01 for both Co and Cr; Fig. 2). Log blood metal ion concentrations were significantly higher in cups with inclination >55° compared to those with inclination of 35°-55° (p<0.001 for both Co and Cr; Fig. 3). There were 84 (26%) BHRs exhibiting abnormal radiology (Tab. I) and log blood metal ion concentrations were significantly higher in this group compared to the normal radiology group (p = 0.002 for both Co and Cr). Blood metal ions above 7 µg/l were observed in 14 of 84 BHRs with abnormal radiology. The most frequent abnormal radiological feature in these 14 hips with raised metal ions was acetabular component inclination outside 35°-55° (11 hips). Of these malpositioned hips, 1 also demonstrated both femoral lucency (zone 1) and acetabular osteolysis (zone 1), and another hip had acetabular lucencies (zones 1 and 2). The other 3 hips with abnormal radiology, raised blood metal ions, but normal acetabular component inclinations all showed evidence of radiographic lucency (1 in acetabular and femoral zones 1, and 2 hips with acetabular lucency in zone 2). All radiological lucent lines were non-progressive on serial radiographs and patients were asymptomatic.
Univariate linear regression modelling demonstrated that the highest proportion of variance in the logarithms of blood metal ion concentrations was explained by femoral head size (Co p<0.001, R2 = 8%; Cr p<0.001, R2 = 11%; Fig. 4) followed by gender (Co p<0.001, R2 = 8%; Cr p<0.001, R2 = 10%), inclination (Co p<0.001, R2 = 4%; Cr p<0.001, R2 = 4%; Fig. 5) and time since index operation (Co p = 0.032, R2 = 1%; Cr p = 0.255, R2<1%). Multivariate linear regression modelling demonstrated the best fitting models for predicting log blood cobalt and chromium levels were additive ones combining femoral head size, gender, time since index operation and an interaction term between acetabular inclination and time since index operation (Co p<0.001, R2 = 13%; Cr p<0.001, R2 = 15%).
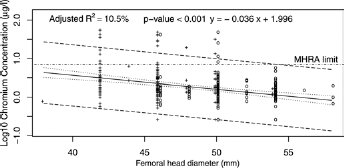
Log10 whole blood chromium concentration modelled on femoral head diameter with regression line (solid), 95% confidence limits (dotted) and 95% prediction limits (dashed). The MHRA upper limit of 7 µg/l is indicated by the dot-dashed horizontal line. Hips from females are indicated by a ‘+’ and from males by an ‘o’. Similar results were obtained for log10 blood cobalt concentrations (Adjusted R2 = 8%, p-value <0.001, y = −0.040x + 2.037).
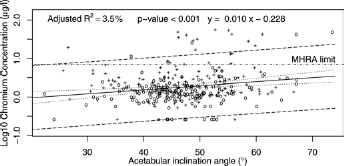
Log10 whole blood chromium concentration modelled on acetabular inclination angle with regression line (solid), 95% confidence limits (dotted) and 95% prediction limits (dashed). The MHRA upper limit of 7 µg/l is indicated by the dot-dashed horizontal line. Hips from females are indicated by a ‘+’ and from males by an ‘o’. Similar results were obtained for log10 blood cobalt concentrations (Adjusted R2 = 4%, p-value <0.001, y = 0.013x-0.515).
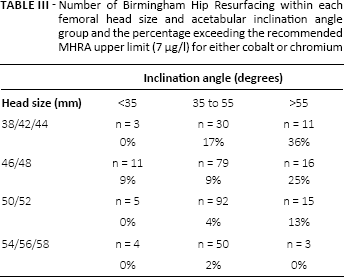
Analysis of femoral head size and acetabular inclination together demonstrated that BHRs with high inclinations and small femoral head sizes were the most predictive for identifying patients with blood metal ion concentrations above the recommended 7 µg/l threshold. Blood metal ion concentrations above 7 µg/l were observed in 36% of BHRs with femoral head sizes of 38-44 mm and acetabular inclination >55° (Tab. III).
Number of Birmingham Hip Resurfacing within each femoral head size and acetabular inclination angle group and the percentage exceeding the recommended mhra upper limit (7 µg/l) for either cobalt or chromium
Hip dysplasia is more prevalent in females who, in general, have smaller femoral head sizes and higher inclination angles due to difficulty in positioning the acetabular component. An exact Fisher test on the proportions of hips with blood metal ions >7 µg/l demonstrated no significant difference (odds ratio = 2.20, 95% CIs = 0.5-7.51, p = 0.251) between BHRs implanted for primary osteoarthritis (19/239 BHRs above MHRA upper limit) and BHRs implanted for developmental hip dysplasia (4/25 BHRs above MHRA upper limit).
All 28 patients with blood metal ions above 7 µg/l were investigated with cross-sectional imaging (ultrasound for symptomatic patients, and metal artifact reduction sequence magnetic resonance imaging for asymptomatic patients). Following cross-sectional imaging, 16 revisions have been performed (15 ARMD and 1 periprosthetic fracture) in the 28 patients with blood metal ions above 7 µg/l. The indications for ARMD revision have evolved over time and between surgeons given no evidence-based guidelines provide thresholds for revision (13). Generally patients with blood metal ions above 7 µg/l and abnormal cross-sectional imaging (periprosthetic effusions and fluid collections) underwent revision regardless of symptoms (Tab. IV).
Details of 15 patients with blood metal ions above 7 µg/l undergoing revision for adverse reactions to metal debris
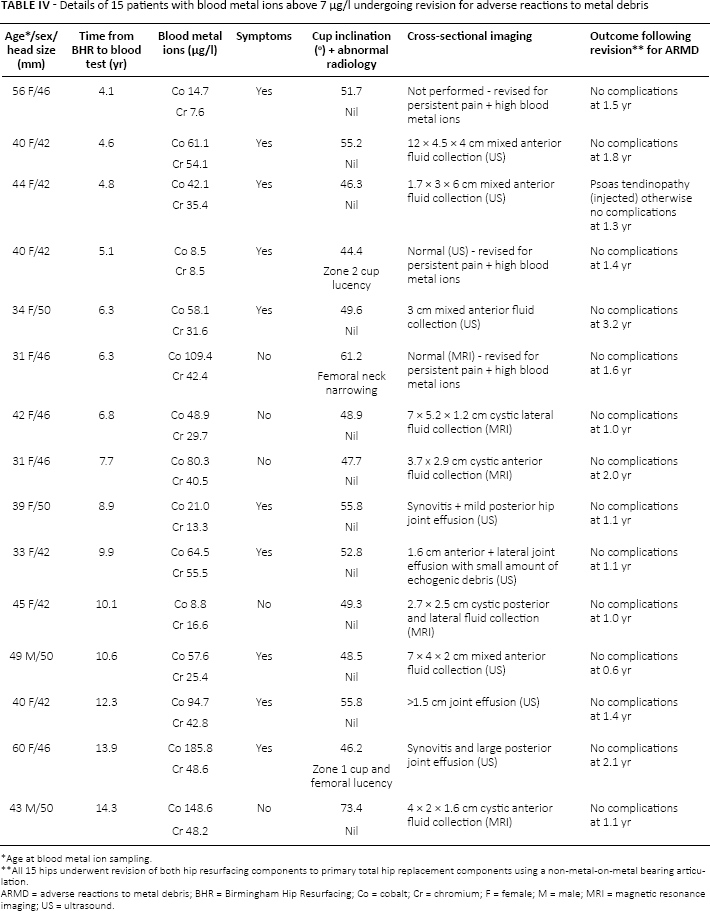
ARMD = adverse reactions to metal debris; BHR = Birmingham Hip Resurfacing; Co = cobalt; Cr = chromium; F = female; M = male; MRI = magnetic resonance imaging; US = ultrasound.
Age at blood metal ion sampling.
All 15 hips underwent revision of both hip resurfacing components to primary total hip replacement components using a non-metal-on-metal bearing articulation.
However, patients with increasing blood metal ions and persistent hip pain were also considered for revision by some surgeons despite normal cross-sectional imaging (Tab. IV).
Of the remaining 12 BHR patients with high blood metal ions, 9 had normal cross-sectional imaging and remain under annual clinical surveillance (repeat blood metal ion sampling and imaging). The remaining 3 asymptomatic BHR patients with high blood metal ions had abnormal cross-sectional imaging (effusions and fluid collections ranging from 5.5 cm3 to 75 cm3) but have refused to undergo revision surgery. These patients remain under 6-monthly review (repeat blood metal ion sampling and imaging).
Revisions have also been performed in 14 patients with blood metal ion levels ≤7 µg/l (5 ARMD, 3 unexplained pain, 2 aseptic cup loosening, 2 aseptic stem loosening, 1 femoral head osteonecrosis, and 1 osteolysis of the femoral neck). The 30 revisions performed in patients at risk of ARMD (n = 319) were at a mean of 8.9 years (range 4.1-15.0 years) from index BHR. For survival analysis mean patient follow-up was 8.0 years (range 1.0-16.4 years). Cumulative 10-year survival for all BHRs (n = 319) was 91% (95% CI 86.0%-95.0%; 107 hips at risk). The cumulative 10-year survival for BHRs with blood metal ions >7 µg/l (n = 28) was 86.0% (95% CI 77.7%-97.4%) compared to 97.9% (95% CI 96.3%-99.5%) for BHRs with ions ≤7 µg/l (n = 291) (Fig. 6). Patients with blood metal ions >7 µg/l had a 6.5 times (95% CI 3.1-13.8; p<0.0001) increased risk of revision than patients with levels ≤7 µg/l.
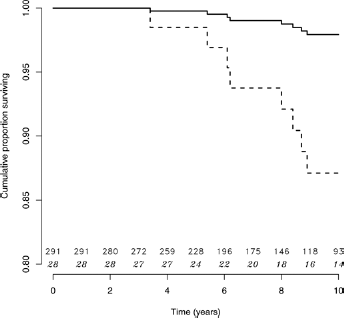
Cox-proportional hazards model comparing implant survival between patients with high (>7 µg/l) and low (≤7 µg/l) blood metal ion concentrations. Dashed line = blood metal ion concentrations >7 µg/l; Solid line = blood metal ion concentrations ≤7 µg/l; numbers on horizontal axis represent the number of hips at risk each year for the respective blood metal ion group (non-italic top row ≤7 µg/l, and italic bottom row >7 µg/l).
Discussion
A relatively low prevalence of high blood metal ion concentrations following BHR was observed in this study compared to previous reports (33-34-35) with 9% of patients having blood metal ions above the MHRA upper limit of 7 µg/l. This is reassuring given the cohort tested was considered at-risk of ARMD (all symptomatic patients and asymptomatic patients with specific clinical and/or radiological findings). It is likely the low prevalence of high blood metal ion concentrations observed is due to the use of a prosthesis with an established record implanted by experienced surgeons (2-3-4-5, 23). This study also demonstrated the best predictors of high blood metal ion concentrations (>7 µg/l) following BHR were hips with small femoral head sizes (38-44 mm) and high acetabular inclinations (>55°).
The relationship between gender and femoral head size to hip resurfacing outcomes appears to be complex. Although most reports suggest smaller femoral head sizes are associated with increasing revision rates (36-37-38), 1 study observed that gender, and not femoral head size, significantly increased the risk of hip resurfacing revision for ARMD (17). With regards to blood metal ion concentrations, the present study demonstrated that although females and hips with small femoral head sizes have significantly higher blood metal ion concentrations, femoral head size was most influential (R2 = 8% for Co and R2 = 11% for Cr). These findings are supported by studies demonstrating higher blood metal ions in patients with smaller femoral head sizes for various hip resurfacing designs (39, 40). Our findings regarding blood metal ions support those relating to revision rates reported by the Australian Joint Registry (41) and another study involving BHR patients (36), with both demonstrating hip resurfacing revision rates were independent of gender once femoral component size was accounted for. Anatomical differences between genders are likely to be responsible for the interactions between gender and femoral head size as smaller components are most often implanted in females (11). We show femoral head size to be the most important factor for high blood metal ions following BHR though recognise the majority of these patients will be female.
This study observed significantly higher blood metal ion concentrations in patients with acetabular inclinations above 55°. These findings have been reported with a range of different hip resurfacing implants and it is suspected the raised concentrations are because of an increased risk of edge-loading with higher inclination angles (16, 39). However, when using linear regression acetabular inclination accounted for a significant but small variation in blood metal ions (R2 = 4% for both Co and Cr). In addition to femoral head size it is likely other factors may be important in contributing to high blood metal ion concentrations, such as implant metallurgy. In contrast to our findings with the BHR a recent large study of a metal-on-metal hip replacement system no longer in clinical use demonstrated the association between acetabular inclination angle and blood cobalt concentration only reached significance with small femoral component sizes (34). The authors concluded the high implant failure rate was more likely related to design flaws rather than modifiable factors.
In the present study the best predictors of high blood metal ions following BHR were hips with high acetabular inclinations (>55°) and small femoral head sizes (38-44 mm). It is therefore recommended this subgroup of BHR patients undergo screening for ARMD using blood metal ion sampling, even if asymptomatic. However, as these parameters only identified 36% of all patients with high blood metal ion concentrations it is recognised other investigations, such as cross-sectional imaging, are important when ARMD is suspected but blood metal ion concentrations are 7 µg/l or below.
Although the present cohort was considered an at-risk group for ARMD, implant survival at 10-years (91%) was comparable to that from independent centres (range 87%-95%) reporting on BHRs performed in all-comers rather than an exclusively at-risk group (2, 3, 5, 35). This study also demonstrated raised blood metal ion concentrations were associated with a significantly higher risk of implant failure (6.5 times increased risk of revision if >7 µg/l versus ≤7 µg/l) which supports previous findings (42).
This study has recognised limitations. First, the findings reported are based on a non-consecutive series of patients which may introduce selection bias. As patients undergoing blood metal ion sampling were mostly symptomatic (median OHS 31.0/48) many patients with well-functioning implants were not tested given the good long-term outcomes we have reported with the BHR (4). The true prevalence of raised blood metal ions in all BHRs performed at this centre may therefore differ to that reported here. Second, it is recognised complex interactions exist between the positioning of the acetabular and femoral components (18), which have been demonstrated to affect blood metal ions (16, 39). Although acetabular inclination was assessed, other factors which may affect blood metal ion concentrations such as acetabular anteversion and combined anteversion were not assessed, as it was not possible to measure these accurately using the software available. These variables may also have been useful in identifying patients with high blood metal ions. Third, the presence of other metal implants in the body was not used as an exclusion criterion. Some similar studies have made patient exclusions on this basis (43) whilst others have not (40, 44). Finally, although the BHR is the most popular resurfacing device implanted in England and Wales (23) the study findings may not be applicable to other hip resurfacing devices with different radial clearances, coverage arcs, and metallurgy (7, 19).
Conclusions
If blood metal ion concentrations are used for screening hip resurfacing patients for ARMD it is recommended the subgroup to target are those with femoral head sizes of 44 mm or less and acetabular component inclinations over 55°. As smaller femoral head sizes tend to be implanted in females it is recognised the population to be screened will predominantly be female. It is recognised our findings may not be applicable to all hip resurfacing devices, therefore these findings require validation in hip resurfacing cohorts at other centres prior to any widespread implementation as part of screening for ARMD.
Footnotes
Acknowledgment
The authors would like to thank The Royal College of Surgeons of England and The Arthritis Research Trust, which have provided one of the authors with funding in the form of a Surgical Research Fellowship.
Financial support: GSM: has received financial support in the form of a Surgical Research Fellowship from The Royal College of Surgeons of England and The Arthritis Research Trust. PBP, RBCT, DJD: Funding received by the institution from Smith and Nephew for maintaining the hospital database, which was used for this study and other projects.
Conflict of interest: FB: Salary paid by Smith and Nephew. The other authors have no conflicts of interest to declare.