
Abstract
Introduction
Scyon Orthopaedics AG developed a new mode of cementless fixation of the femoral component that provides immediate and permanent anchorage by monocortical locking screws. The aim of this study was to evaluate the stability of the Scyon total hip replacement (THR) stem in-vivo.
Methods
A total of 15 patients, with an average age of 50 years had surgery between 2008 and 2011. Each patient received a Scyon THR. Standard questionnaires were completed at each follow-up visit for evaluation of functional outcomes. RSA, patient reported outcomes, and plain radiographic follow-up were obtained at 6 months, 1 year, 2 years, and 5 years postoperatively.
Results
The median ± standard error (SE) stem subsidence (negative y-translation) was 0.07 ± 0.07 mm at 1 year, 0.05 ± 0.04 mm at 2 years and 0.04 ± 0.13 mm at 5 years. The median ± SE stem rotation (y-rotation) was 0.1 ± 0.21 degrees at 1 year, 0.51 ± 0.31 degrees at 2 years and 0.60 ± 0.37 degrees at 5 years. Plain radiographs showed bone on-growth onto medial aspect of the stem. Median HHS improved from 55 preoperatively to 93 at 1 year and 97 at 5 years. The median UCLA Activity Score improved from 4 preoperatively to 6 at 1 year and 5 years.
Conclusions
RSA results indicate that the Scyon stem with its 5 monocortical locking screws is stable at 5 years. Immediate surgical fixation of the stem and bony on-growth onto the femoral component may ultimately decrease the rate of aseptic stem loosening in these THR patients.
Keywords
Introduction
Total hip replacement (THR) is one of the most successful orthopaedic procedures of the 20th century (1). Since the first THR, the field of hip replacement surgery evolved rapidly in part by the introduction of acrylic cement for fixation of the THR components (2). Fatigue of the cement mantle around the femoral stem was a common precursor of aseptic loosening of the component, which was the leading cause of stem failure (3-4-5). After 2 decades of experience with cemented hip replacements, the use of cementless devices increased in the 1980s (6). However, the technological modifications in various cementless devices have not yet offered the desired improvement partly due to polyethylene wear issues (7-8-9-10-11).
Despite registry data indicating superior survivorship of cemented THRs, the use of cementless prostheses have been steadily rising. Experimental investigations show that canal-filling cementless metal stems are not uniformly stable at all contact areas with the femur under physiological loading (12, 13). Furthermore, cementless stems can result in more intense stress-shielding and higher shear loads, leading to increased micromotion at the bone-implant interface. If micromotion occurs before the bone-prosthesis interface is established through bone ingrowth or ongrowth to the implant, a fibrous layer develops, preventing solid anchorage of the prosthesis (14, 15). To prevent this from happening, the hip should be protected from overloading during the 12 to 16 week period necessary for the bone to remodel and provide solid support. However, most rehabilitation protocols typically include different isometric exercises, which result in hip loads similar to those recorded during normal gait (16, 17). As a result, stability of the majority of press-fit stems is jeopardised. Failure to preserve a stable bone-implant interface can lead to aseptic loosening of the stem resulting in pain and ultimately leading to revision.
Scyon Orthopaedics AG (Waedenswil, Switzerland) developed a new mode of cementless fixation of the femoral component. This new technique provides immediate anchorage by solving 2 complementary problems: load-induced micromotion at the bone-implant interfaces; and stress-shielding of the proximal femur. The Scyon THR stem is anchored to the medial cortex through monocortical locking screws, which includes pre-loading of the stem collar against the calcar in the immediate post-operative period. Transfer of the joint force directly to the medial cortex, closely resembles the physiological loading, unlike conventional press-fit stems that induce non-physiological hoop and bending stresses to the proximal femur. The stable fixation of the stem creates a micro-motion free condition necessary for good bone apposition onto the stem. The concept was inspired by the research and development of the “PC-Fix” internal fixator at the AO Research Institute, in Davos, Switzerland (18-19-20), and the clinical application of the Zurich Cementless THR in more than 12,000 dogs during 2 decades (21).
The objective of this study was to evaluate the stability of the Scyon THR stem in-vivo using radiostereometric analysis (RSA), plain radiographic analysis, and patient reported outcomes at 6 months, 1, 2, and 5 years postoperatively.
Materials and methods
After obtaining institutional review board approval, all patients provided informed consent to participate. In total 15 patients, all with a primary diagnosis of osteoarthritis were enrolled in this clinical study. The patients, 6 males and 9 females, with an average age of 50 years (range 35-62 years) had surgery between April 2008 and May 2011. Inclusion criteria were: non-inflammatory arthritis with Harris Hip Score (HHS) ≤60; good bone quality (subjectively assessed from radiographs); no prior active infection in the affected joint; no current systemic infection; and the ability to return for follow-up visits at 6 months, 1, 2 and 5 years postoperatively. Potential candidates were excluded from participation in the study if they presented any of the following: immunological disorder; need for revision arthroplasty; known sensitivity to materials in the device; pregnant women or women with suspicion of pregnancy, or plans to become pregnant within follow-up period; or subjects unable to comprehend the study protocol for any reason.
All procedures were performed by a single surgeon who used the direct lateral, transgluteal approach according to Hardinge (22). Each patient received a Scyon THR stem, a Scyon THR press-fit fossa acetabular cup, and a 28 mm cobalt-chromium alloy head. The acetabular cup was metal-backed by a double titanium (Ti grade 4) shell, the outer of which was perforated with a pattern of 1.4 mm diameter holes giving a surface porosity of 55% and rough blasted (Ra = 5 µm). The liner was made of ultra-high molecular weight polyethylene with a slightly aspherical bearing geometry which reduced surface stresses and improved lubrication. After machining, the stem was shot peened for improved fatigue strength and then rough blasted on the anterior, medial and posterior surfaces (Ra = 5 µm). The lateral surface of the stem is not rough blasted leaving a smooth finish to discourage bone ongrowth. The screws were anodised for easy identification of the different lengths. The Scyon stem and screws were manufactured from titanium alloy (Ti6Al4V).
For Scyon stem insertion, most of the cancellous bone was removed from the medial endosteum to allow for tight contact of the stem to the medial cortex. Broaching of the medullary cavity was performed by hand using 2 broaches; 1 for the medial and 1 for the lateral aspect of the stem. The broaches, non-canal filling, U-shaped in the cross section, were designed to prevent increase in medullary pressure and thus minimise the risk of fatty marrow induced embolisation (23). A significant amount of the medullary cancellous bone and some vascular supply were preserved. Reaming towards the lateral cortex only needs to exceed the size of the stem by 1 or 2 mm. In the distal region of the stem, the amount of lateral cancellous bone and vascular supply preserved depends on the size of the femur, and, in the proximal femur, the greater trochanter remains largely untouched. In Figure 1 a gap of approximately 2 mm can be seen lateral to the stem. The bone lateral to this gap remained intact. For ease of stem insertion, an insertion guide is fixed to the neck of the stem and serves as a handle. To facilitate stem insertion, the femur is externally rotated to expose the anteromedial aspect of the femur. Following insertion of the stem, drill sleeves are placed through the insertion guide and tightened against the bone between vastus medialis and vastus intermedius. Tightening of the drill sleeves brings the stem into position against the medial endosteal surface for final control of stem position. Drilling of holes for the screws and insertion of the screws is performed through the drill sleeves into the medial cortex. For the size M stem used, 5 monocortical locking screws were tapped through the medial cortex and locked in the stem. The most proximal screw extended through the stem to engage the lateral cortex for added rotational stability. For the purpose of monitoring the stability of the stem by RSA, 3 tantalum markers (0.8 mm in diameter) were attached to the stem at the time of production. A total of 8 tantalum markers (1.0 mm in diameter) were inserted into the polyethylene liner equidistant around the equator and 1 additional marker to indicate the fossa position. Additionally, tantalum markers (0.8 mm in diameter) were inserted intraoperative into specific areas of the pelvis surrounding the acetabular cup and proximal femur surrounding the stem (Fig. 1).

AP hip radiograph showing the distribution of the tantalum beads for the purpose of RSA.
Postoperative rehabilitation consisted of passive motion for 1 week followed by progressive weight bearing: 30% weight bearing for 3 weeks using 2 crutches; 60% weight bearing for an additional 3 weeks. Full weight bearing starting at 7 weeks postoperative.
Standard preoperative and postoperative questionnaires (HHS and UCLA Activity Score) were completed for all patients at each follow-up visit for evaluation of functional outcomes. RSA, patient reported outcomes, and plain radiographic follow-up were obtained at 6 months, 1 year, 2 years, and 5 years postoperatively. RSA was used to compare immediate postoperative radiographs to films taken at each subsequent follow-up interval utilizing UmRSA 6.0 software (RSA Biomedical, Umeå, Sweden) in order to evaluate micromotion of the stem segment relative to the proximal femur segment. A uniplanar calibration cage (model 43, RSA Biomedical, Umeå, Sweden) was positioned under the hip, and the supine patient was oriented such that the femur was centered within each of the foci with the femur parallel to the y-axis. Stereoradiographs were taken concurrently from 2 x-ray tubes (1 ceiling-mounted and 1 portable) at convergent angles, enabling the reconstruction of a 3D image of the implant and bone segments. Each segment was defined by at least 3 beads. The stem had 3 beads (the distal tip marker and 2 collar markers on the stem) and the centre of the head defining the segment (Fig. 2). The analyses were performed using segment motion, comparing stem segment with the femoral bone segment. One patient's stem did not have 3 visible points, therefore point motion was utilised to compare the centre of the head to the femoral bone segment. Double RSA examinations were completed for 6 of the 15 patients. These exams estimated the 95% confidence interval for the error of the RSA setup. Any kinematic measurement that was outside this interval was considered true motion, and conversely, any measurement that was within this interval was considered indiscernible due to the error of the radiographic setup. The postoperative and 6 month films of the first 8 patients were printed and then scanned for evaluation. The remaining films for these patients and all films for patients 9 to 15 were transmitted directly as digital radiographs for evaluation. All digital radiographs had a resolution of 5 pixels/mm. As a result of the lower resolution caused by scanning of the printed films in the early follow-up of the first 8 patients, the tantalum beads were difficult to visualise. Therefore, the maximum acceptable condition number was set at 250 (24). The maximum mean error was 0.25 mm in the RSA kinematics rigid body fittings. Plane x-rays were evaluated for 6 conditions: resorption under the collar, resorption of the medial cortex around any of the screws, radiolucency around proximal screw in lateral cortex, sclerotic line at lateral edge of the stem, hypertrophy of the medial cortex, and bone apposition onto the tip of the stem. If the observation of the condition was positive, that patient at that time period was assigned a 1. If the observation of the condition was negative, a 0 was assigned.
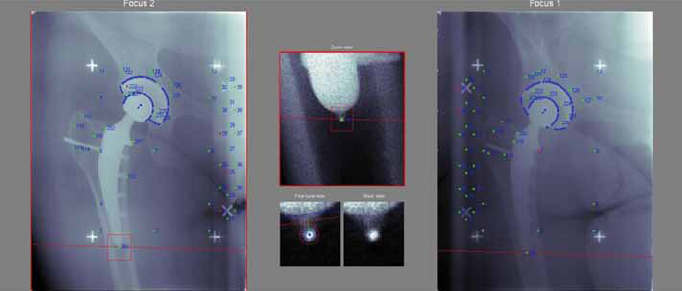
An RSA film pair showing the stem and femoral bone segments oriented within the confines of the calibration cage which was placed beneath the supine patient.
To determine if there was significant migration of the implant between the 6 month, 1, 2, and 5 year films, a Wilcoxon paired signed ranks test was used. This test was also used to determine differences in patient reported outcomes over time. A power analysis was performed for a 1 sample, 2-tailed t-test with 80% power and the chance of a Type I error of 5%. Results of the analysis indicated that 5 patients were necessary to show 400 µm of clinically relevant subsidence of the femoral component with a standard deviation of 200 µm (25). Significance in all tests was established at p≤0.05.
Results
At the time of data analysis, all 15 patients had 6 month, 1 and 2 year follow-up, and 8 patients had 5-year follow-up. The postoperative film pair was established as the baseline for all RSA assessment of translation and rotation and was taken after mobilisation. The median ± standard error (SE) stem subsidence (negative y-translation) was 0.07 ± 0.07 mm at 1 year, and 0.05 ± 0.04 mm at 2 years, and 0.04 ± 0.13 mm at 5 years (Fig. 3). The median ± SE stem rotation (y-rotation) was 0.1 ± 0.21 degrees at 1 year, 0.51 ± 0.31 degrees at 2 years and 0.60 ± 0.37 degrees at 5 years (Tab. I). A Wilcoxon signed-rank test showed that there was no statistically significant change in the median proximal/distal translations or rotations among any of follow-up intervals.
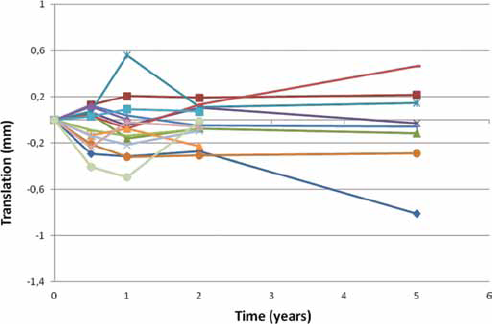
The y-translation at 6 months, 1, 2, and 5 years for all patients.
The median (range) y-translation and rotation of the Scyon stem at 6 months, 1, 2, and 5 years as well as the precision of the radiographic set-up defined by the 95% confidence interval

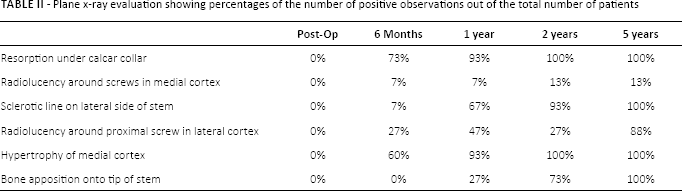
The plain radiographic results showed bone remodelling that is expected with this type of implant (Tab. II). Resorption under the calcar collar was observed in all patients at 2 years. Radiolucency around a single screw was observed in 1 patient at 6 months and in a second patient at 2 years. A sclerotic line on the lateral side of the stem became evident in 14 of the 15 patients at 2 years, and was seen in all 8 of the 8 patients at 5 years. Radiolucency in the lateral cortex around the most proximal screw was seen in almost all patients at 5 years. Hypertrophy of the medial cortex reached 100% at 2 years. Bone apposition onto the tip of the stem appeared first at 1 year and increased to 100% at 5 years (Fig. 4).
Plane x-ray evaluation showing percentages of the number of positive observations out of the total number of patients

AP hip radiographic 5 year after surgery showing the hypertophy of the medial cortex indicating bone ongrowth and sclerotic line along lateral aspect of the stem indicating inhibition of the bone ongrowth.
The median HHS improved from 55 preoperatively to 93 at 1 year and 97 at 5 years. The median UCLA Activity Score improved from 4 preoperatively to 6 at 1 year and 5 years. All postoperative scores were statistically higher than all preoperative scores for both the HHS and the UCLA Activity score (p = 0.001 for all comparisons). Improvement was also observed between the 6 month and 2 year interval for both the HHS and UCLA Activity Score (p = 0.022 and p = 0.033, respectively). Neither score changed significantly from the 2 year to 5 year interval. There was 1 serious postoperative complication; 1 patient developed a pulmonary embolism on the first day after surgery and made a full recovery. The patient is still an active participant in the study.
Discussion
RSA results indicate that the Scyon stem with its 5 monocortical locking screws is stable at 5 years. Immediate surgical fixation of the stem via these screws appears to inhibit early micromotion and thus may prevent the formation of a fibrous layer between the bone and the component. In the absence of a fibrous layer, bone on-growth onto the femoral component may ultimately decrease the rate of aseptic stem loosening in these THR patients.
The median stem subsidence from 1 to 5 years was minimal and did not increase significantly over time. Kärrholm et al concluded that cementless stems evaluated by RSA that subside more than 1 to 1.5 mm 2 years after surgery have a significantly greater likelihood of failing (25). The subsidence measured at 1, 2 and 5 years was well below the range set by Kärrholm et al and thus deemed clinically acceptable. There was no measured median stem rotation at any interval except the 5-year interval, since the median rotations at these time points were within the 95% confidence interval defining the precision of the radiographic setup. Although the 5-year rotation was true motion, this rotation was not significantly different than the previous intervals. Since the precision of the setup, defined by the 95% confidence interval, was strong as evidenced by the narrow intervals, we conclude that if the stem is rotating, it is an amount so small that it is undetectable by RSA.
The 95% confidence interval, as calculated by the double examinations, showed that there was a high level of precision for measuring femoral stem migration. Additionally, the attachment of the tantalum beads to the femoral stem at the time of manufacturing makes this a particularly strong RSA study because the stem beads form their own segment characterising the entirety of the stem, instead of using only the centre of the femoral head as a surrogate for the entire stem. The use of stem segment motion instead of femoral head point motion compared to the bone segment yields rotation in addition to translation of the stem. Femoral head point motion alone, without additional beads defining the stem yields only translational kinematics, and not rotation. Although the precision was strong, a limitation of the study was the necessity of increasing the maximum acceptable condition number from 150 to 250, due to some early RSA films that were scanned instead of digital. Despite this, the reproducibility of the kinematics at each interval suggests a strong RSA set-up.
Appropriate load transfer onto the femur is crucial in long-term maintenance of bone density and volume. Insertion of a femoral stem imposes a new biomechanical state in the surrounding bone. While the exact mechanism remains elusive despite decades of research, reduction of bone density in response to reduced bone stresses is commonly referred to as stress-shielding. The process of the load transfer mechanism is strongly influenced by the design and stiffness of the implant. The stiffer the stem is compared to the bone, the more pronounced stress-shielding is in the proximal femur (26). The quantity of bone loss due to stress-shielding is also greatly increased by stem engagement of the medial and lateral cortices of the proximal femur (27-28-29). Stress-shielding is an ongoing concern in cementless stem fixation due to clinically relevant issues such as periprosthetic fractures and the difficulty of some surgical techniques, such as the complicated removal of the stem with strong distal anchorage at revision surgery. As opposed to the press-fit concept, the Scyon stem preserves near-normal physiological loading of the proximal femur. By averting the need to engage, and thus biomechanically couple the lateral and medial cortices, the Scyon stem provides consistent fixation within the femur, which highly diminishes stress-shielding of the proximal femur. The bone remodelling around the screws reduces stress concentration while bone apposition onto the stem takes over as the primary load transfer mechanism. Once bone apposition has occurred, the role of the screws as means of load transfer in the long-term could be negligible. However, their presence in the bone is necessary to prevent stress concentrations around the screw holes after bone remodelling and adaptation to the screws.
A similar canine THR stem system, called the Zurich Cementless THR (Kyon AG, Zurich, Switzerland) has gained broad recognition over the past decades as an evolutionary step in veterinary surgical practice (30). After 20 years of clinical use, the Zurich Cementless THR has been implanted in over 12,000 dogs by more than 180 surgeons. The long-term data from different clinical studies reported by leading experts in canine THR have shown that stable stem fixation, followed by bone on-growth, has resulted in a statistically significant decreased risk of aseptic loosening in comparison with standard cemented canine THR (31). As it is well accepted that dogs are a valid model for research and development of human THR components, these long-term canine results are encouraging. The measured stability of the Scyon stem in this population at 5 years suggests that the stabilised stem in humans may also decrease aseptic loosening of cementless stems in the long-term. The process of reaming the bone to the cortex followed by insertion of the metallic press-fit stem limited remodelling from the endosteal side of the bone. Conversely, the locked screw fixation of the Scyon stem to the medial cortex alone allows re-vascularisation and remodelling to proceed without risk of loosening of the femoral component.
Evaluation of plain radiographs
Resorption under the collar: Loss of bone at the calcar directly under the collar of the stem was expected. The calcar support of the collar of the stem is preloaded when the stem is screwed into position. This preload gives initial stability to the proximal support. Once the load transfer from the stem to the bone occurs through the bone ongrowth onto the stem, the transfer of load at the calcar/collar interface will diminish and resorption of the bone there is expected.
Resorption in medial cortex around any screw: The screw heads in the medial cortex are radially preloaded and share the load transfer from the stem to the bone. Once bone ongrowth onto the stem occurs, the transfer of load through the screws will be reduced. However, the screws should remain well integrated in the bone.
Radiolucency around proximal screw in lateral cortex: The lateral end of the proximal screw provides initial rotational stability of the stem at the proximal end. Once the bone ongrowth onto the stem occurs, there is no further need for contact to the lateral cortex. The tip of the screw was left smooth on purpose so that the screw tip will not become integrated into the lateral cortex and no coupling of forces occurs between lateral and medial cortices. Thus, due to the difference in deformations between the medial and lateral cortices, there will be micromotion occurring between the screw tip and the lateral bone. This has led to radiolucency around the screw tip as anticipated.
Sclerotic line at lateral edge of the stem: The stem was rough blasted on the medial, anterior, and posterior surfaces for bone ongrowth. The lateral surface of the stem was left smooth so that integration of the lateral cortex was inhibited. By design, the stem was not to be press fit with ongrowth from the lateral cortex. Coupling of the lateral and medial cortices causes stress shielding. Since bone will grow towards the stem from the lateral intramedullary surface, but not attach to the stem, a sclerotic line at the lateral edge of the stem was expected.
Hypertrophy of the medial cortex: As the joint load is shifted to the medial cortex, thickening of the medial cortex was expected.
Bone apposition onto the tip of the stem: When the stem is stable and fixed to the medial cortex, bone will start to fill in between the medial cortex and the stem, including around the distal tip of the stem. This is an indication that the construct is stable and a sign of bone adaptation once the load carrying by the stem ends at its distal tip. This is in contrast to bone formation separated by a lucent zone distal to the stem as a consequence of stem pistoning.
In conclusion, based on the results of the 5-year follow-up, we believe that this new stem model may decrease the aseptic loosening rate of the THR by means of a more reliable and consistent fixation of the femoral stem, which could diminish stress-shielding of the proximal femur. Longer-term follow-up of this cohort is necessary to definitively determine if this stem will remain stable and eliminate the problems associated with stress-shielding.
Footnotes
Acknowledgements
Recruiting of patients into the study was assisted by Prof. A. Muljacic from the Hospital for Traumatology in Zagreb, Croatia. The RSA data analysis was performed in part by Bryan Jarret, at the Harris Orthopaedic Laboratory, Massachusetts General Hospital, Boston, MA.
Financial support: This study was supported by Scyon Orthopaedics AG, Au, Switzerland.
Conflict of interest: None.