
Abstract
There is limited knowledge regarding the anatomic relationships and functional anatomy of the Obturator Externus muscle (OE). It is described as a muscle which originates from the external bony margin of the obturator foramen with a cylindrical tendon which passes like a sling under the femoral neck and inserts in the trochanteric fossa. The primary aim of this study is to describe the OE morphology and its anatomic relationship to the acetabulum. A secondary aim is to postulate its action. Eighteen fresh human cadaveric hips were dissected to investigate the anatomy of the OE. A plastic model of the pelvis and femur was used to create a string model based on a technique previously described by Beck et al. The plastic model was used to determine the function of the OE.
We conclude that the Obturator externus muscle helps to stabilise the head of the femur in the socket. The mechanical model demonstrated that the primary action of the obturator externus muscle was to externally rotate the femur when the hip was in neutral position and flexed at 90°. Its secondary function was as an adductor when the hip was in flexion.
Keywords
Introduction
Knowledge of the functional anatomy and the anatomic relationship of the obturator externus muscle (OE) is limited. It is described as a muscle which originates from the external bony margin of the obturator foramen and the obturator membrane with a cylindrical tendon passing like a sling under the femoral neck and inserting into the trochanteric fossa. Solomon et al in their anatomical study explored the function of the obturator externus as a hip stabiliser following total hip replacement (1). The function of the OE has not been assessed in detail. The OE is considered to be a short external rotator which has a function of external rotation of the hip. Our interest in this muscle was stimulated by noting the different course of this muscle compared to the other short external rotators. We believe it has different functions dependent upon the position of the hip joint. Recently several reports were published regarding the obturator externus bursa and impingement syndrome after total hip replacement, which is of interest with regard to the OE anatomical relation with the hip joint/acetabulum (2-3-4). The purpose of the study is to describe the OE morphology and its anatomic relationship to the acetabulum. A string model of the OE as described previously was used to investigate the potential function (5).
Methodology
IRB approval (E-23715) was obtained from the University of Calgary Medical Bioethics for the study. In total, 22 fresh human cadaver hips were used in this study. In 4 specimens the exposure of the muscle was sub-optimal and those specimens were discarded. Therefore, 18 hip specimens were included in this study (11 females and 7 males, 76 ± 6 years old, obtained from the Anatomy Lab-Health Sciences Centre at University of Calgary).
The initial dissection was carried out through an anterior approach in the supine position with the dissection extended to the adductor compartment. The adductor muscles were detached from their origin. The OE was exposed up to the inferior margin of the acetabulum. The origin and its anatomic relationships were noted. The lengths of the muscular and tendinous portions were noted as was the direction of the fibres. The cadaver was then placed in the lateral position and the dissection was continued through the posterior approach. The short external rotators were carefully dissected. The short external rotators were identified individually and the OE tendon insertion was noted. An arthrotomy was performed and at this stage a sequential release of the piriformis and the conjoint tendon was performed. The OE function as a hip stabiliser was assessed.
The plastic model of the pelvis and femur was used to create a string model of OE based on an investigation of the gluteus minimus previously described (5). Based on the anatomy the muscle was divided into 5 equal sectors, with sector 1 being the most superior part of the muscle origin. The excursion of various parts of the muscle was noted after positioning the hip joint in different positions. Each sector was represented by a non-stretchable line which was firmly fixed both at its origin and insertion and directed by eyelets along the muscle pathway.
The hip was positioned in full extension, neutral and 90° of flexion and the excursion distance measured in internal and external rotation. The excursion distances of abduction and adduction with internal and external rotation were also noted. There were 3 measurements taken at each position and the mean values were calculated. Shortening of the string was interpreted as contraction and elongation as the ability to resist that particular movement.
Results
The OE muscle originated from the external bony margin of the obturator foramen in clockwise direction from 12 o'clock around to the10 o'clock position (right hip viewed from the front) and a few fibres arose from the obturator membrane (Fig. 1). It formed a musculo-tendinous junction at the level of femoral neck. The fibres passed laterally along the inferior margin of the acetabulum acting like a sling at the inferior part of the neck (Fig. 1). The muscle inserted as a cylindrical tendon into the trochanteric fossa with some fibres extending towards the piriformis fossa. The fibres originating from the superior margin of the obturator foramen twisted at the insertion site inserting postero-inferiorly and the fibres originating from the inferior margin inserted antero-superiorly (Fig. 2).
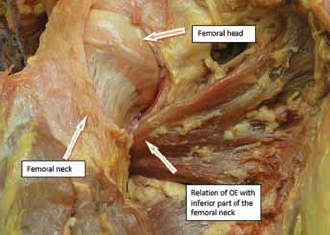
The OE is passing inferior to the femoral neck in right hip.
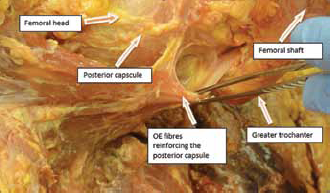
OE fibres reinforce posterior capsule in left hip.
After positioning the hip in flexion, it was observed that the fibres originating from the superior part of the obturator foramen are more relaxed compared to the fibres originating from the inferior margin. All the fibres are straight with the hip at 90º of flexion and externally rotated. The mean muscular length of the tendon is 12.6 cm and it is more muscular than tendinous. There are distinctive fibres reinforcing the posterior hip capsule (Fig. 2).
The OE runs closely to the inferior margin of the acetabulum (Fig. 1). Positioning the hip in abduction and external rotation brings the muscle very close to the caudal border of the acetabulum. Transecting the transverse acetabular ligament brings the OE muscle into direct contact to the inferior margin of the acetabulum. With the hip in a neutral position the tendon is away from the inferior margin of acetabulum. A bursa with bursal fluid was noted between the muscle and the transverse acetabular ligament in 6 of the specimens (Fig. 3). Methylene blue test confirmed that the bursa is communicated with the hip joint in all 6 specimens.
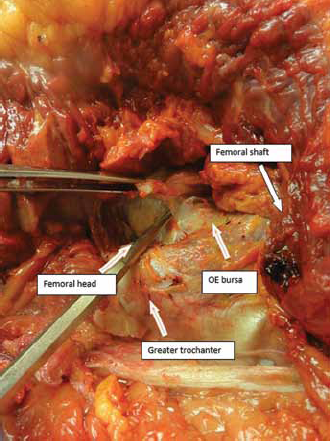
OE bursa at the inferior part on the neck in left hip.
The function of the OE was simulated using a string model (Fig. 4), positioning the hip in different positions. Flexion and external rotation of the hip caused shortening of the strings, indicating a primary function of external rotation. Internal rotation elongated the strings resisting the movement in this position. This also confirms the role of the hip stabiliser function of the OE in flexion and internal rotation. With the hip in extension there is very limited excursion, suggesting the OE muscle does not function as an external rotator in this position. The contractions of all the sectors are nearly similar with the hip in flexion. While moving the hip from abduction to adduction sectors III - V shortened and sectors I and II elongated (Figs. 5-6-7).
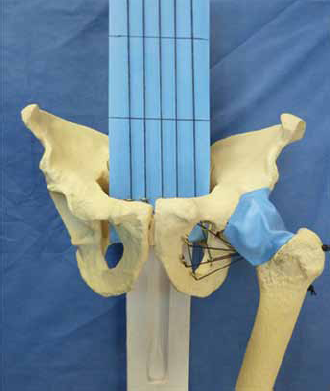
OE function simulated using a string model.
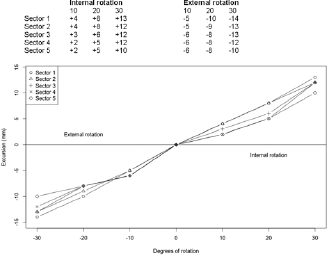
Hip in 90 degree flexion with different degrees of internal and external rotation.
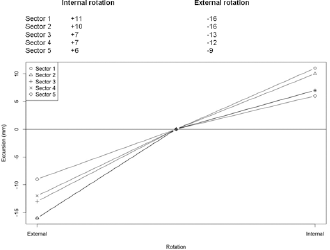
Hip in neutral position.
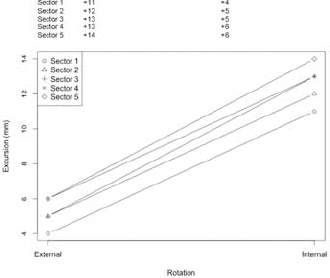
Hip in extension.
Discussion
Current knowledge regarding the functional anatomy of the OE muscle is limited. It's different course and innervation by the posterior branch of the obturator nerve compared to the other short external rotators suggested it may serve a different role (6, 7).
In this study, we explored the special characteristics of the OE muscle including its role as hip stabiliser, anatomic relations and significance and the function of the muscle.
The fibres reinforcing the posterior capsule are noted in 13 out of 18 specimens. This has special implications in providing hip stability. Solomon et al explored the role of the short external rotators in hip stability following a total hip replacement through a posterior approach. They noted that preservation of the piriformis and the external obturator reduces the risk of dislocation (1). We found similar findings in our study using native cadaver hips. The dissections were done through the posterior approach of the hip joint. We preserved the piriformis, and obturator externus and hip joint stability assessed for posterior dislocation and noted to be stable even at 90 degree flexion and internal rotation. In another specimen we followed the similar steps as above and released the OE insertion which made the hip joint prone to dislocation. We noted that the OE with its fibres which reinforce the posterior capsule acts as a hip stabiliser.
Recently several reports have been published which describe OE bursa and obturator impingement syndrome. In these dissections, an OE bursa with bursal fluid was present between the transverse acetabular ligament and the OE muscle in 6 of the 18 specimens. There is evidence of extensive osteoarthritic changes in all these 6 specimens and no arthritic changes noted in the rest of the specimens suggesting that the bursa is present in diseased hips rather than normal hips. This corresponds to the findings reported by Kassarjian et al (4). In their study they looked into 200 consecutive hip MR arthrograms and noted 11 cases of OE bursa. All these patients had intra-articular disease demonstrated by a labral tear and arthritis. Robinson et al (8) noted an OE bursa in their series of patients with histopathologically confirmed pathological hips. Their reports and our study suggest that OE bursa is prevalent in hips with intra articular pathology.
Recent reports have also described OE impingement syndrome following total hip arthroplasty. In our dissections we noted a close relationship between the musculo-tendinous part of the OE muscle and the inferior margin of the acetabulum. Releasing the inferior hip capsule did not bring the OE muscle closer to the caudal border of the acetabulum. However releasing the transverse acetabular ligament did bring the OE muscle in contact with the acetabulum. This is more pronounced while the hip is in the flexed position. While performing a total hip arthroplasty, an acetabular cup position protruding beyond the caudal rim can risk pathological contact of the OE muscle and can cause impingement. Releasing the OE insertion attachment to the posterior capsule decreased the risk of impingement.
The string model helped to assess the function of the OE muscle. Stretching of the string in hip flexion and external rotation suggests that the primary function is that of an external rotator. We also noted a similar function with the hip in the neutral position (acts as an external rotator both in flexion and neutral position). The OE muscle doesn't act as an external rotator in hip extension. Shortening of the string in adduction suggests that the OE muscle acts as an adductor with the hip in the neutral position.
It was also noted that the course of the muscle helps to stabilise the head of the femur in the socket. It also protects the femoral neck as it acts as a suspension sling. We conclude that the primary action of the OE is external rotation in flexion and the neutral position and its secondary function is as an adductor in flexion.
Gauthier et al demonstrated that the obturator externus protects the deep branch of the medial femoral circumflex vessel from stretch or disruption. In their dissections, the integrity of the artery was protected as long as the tendon of the obturator externus was intact, even after release of all other rotators and a circumferential capsulotomy (9).
This study has a number of limitations. A small number of specimens were examined. The cadaveric material was generally from an older population. The string model is a simple representation of the anatomical specimens and it does not replicate muscle contraction and relaxation.
Our study describes the functional anatomy of the OE muscle and its importance as a hip stabiliser. It also described the anatomical relation to the caudal margin of the acetabulum and describes the OE bursa. Findings from our study adds to the current knowledge about the obturator externus muscle.
Footnotes
Financial support: None.
Conflict of interest: None.